The authors and editors of the material contained herein have consulted sources believed to be reliable in their efforts to provide information that is complete and consistent with standards accepted at the time of publication. Some product names, patents and registered designs referred to in this book are in fact registered trademarks or proprietary names, although they are not always specifically referred to in the text.
Accompanying Videos
The first time I looked at the temporal bone through the microscope reminded me of my experience when I was twelve and visited the Grand Canyon in Arizona as a family. These cameras were small enough to avoid altering the balance of the microscope and interfering with the surgeon.
Preface
Acknowledgments
Contributors
Fernando Gonzalez, MD Assistant Professor of
Walter Kutz, Jr., MD
Luxford, MD House Clinic Associate Clinical Professor of Otolaryngology Keck School of Medicine. Wilkinson, MD, FACS Clinical Fellow House Adjunct Research Scientist House Research Institute Clinical Assistant Professor of.
Orbitozygomatic Craniotomy 1
The muscle must be lifted completely from the pterional region down to the level of the zygomatic arch. The final step in the orbitozygomatic-transcavernous exposure is resection of the posterior clinoid process.

The Subtemporal Approach 2
Extradural elevation is performed along the entire floor of the middle fossa, extending forward toward the temporal cusp. After removing the main part of the tumor from Meckel's fossa, the trigeminal nerve can be followed peripherally to the extradural spaces or centrally to the posterior fossa.

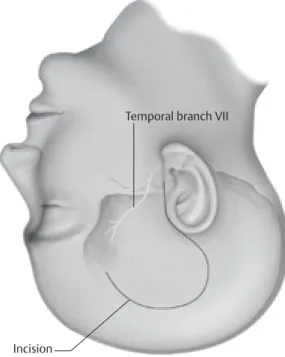
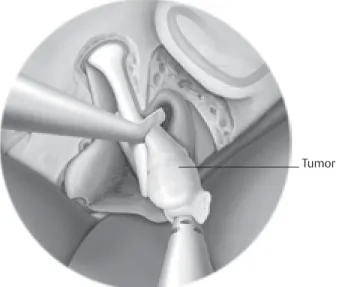
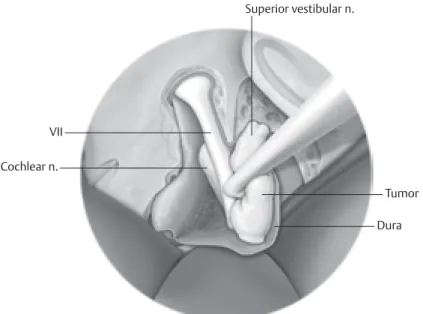
The Middle Cranial Fossa 3
Approach to Vestibular Schwannomas
The distance from the cochlear base to the ampulla of the superior semicircular canal is approximately 2.5 mm. The IAC is skeletonized in its entirety with preservation of the cochlea and the superior semicircular canal.

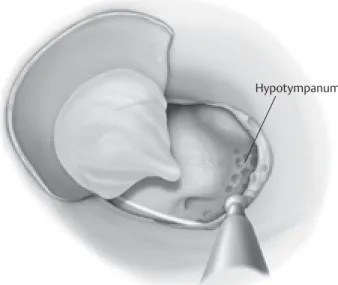
The Infracochlear/ 4
Infralabyrinthine Approach to the Petrous Apex
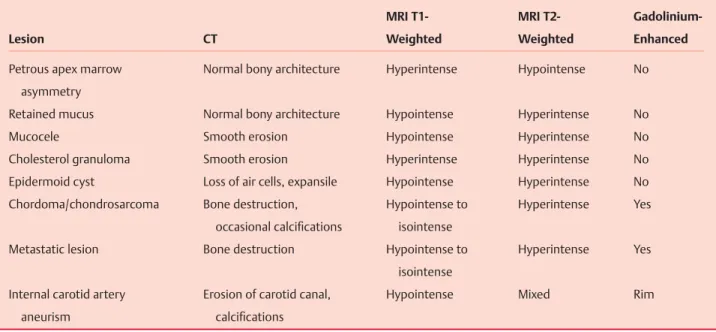
The boundaries of the infracochlear approach include the cochlea, carotid bulb, facial nerve, and petrous carotid artery. Access to the petrous apex is dependent on the location of the lesion and the surrounding vital structures.
The Retrosigmoid Approach 5
Vascular disorders of the vertebrobasilar system and parenchymal lesions of the brainstem and cerebellum. The craniotomy is based on the posterior aspect of the sigmoid sinus and the inferior aspect of the transverse sinus (Figure 5.3). Bone is first removed from the posterior part of the canal to expose the dura of the IAC.
Once the exposure of the IAC is complete, the dura overlying the canal is opened. The tumor is exposed and the vestibular fibers are divided on the lateral domes of the tumor. Another explanation for headaches is adhesion of the posterior fossa dura to the suboccipital musculature.
The advantages of the retrosigmoid approach are the wide access of the CPA and the potential for hearing preservation.

The Translabyrinthine 6
Approach to the Skull Base
The horizontal semicircular canal is a landmark, which helps in identifying the facial nerve and labyrinth. The stapedius muscle is frequently found medial to the vertical segment of the facial nerve. The labyrinthine segment of the facial nerve is then traced just anterior to the ampulla of the superior semicircular canal.
Dissection of the bone above the IAC is performed last because of the presence of the facial nerve at this location. The dura can be reflected from the tip of the IAC, allowing complete exposure of the facial nerve. The tumor must be rotated laterally near the brainstem to allow identification of the facial nerve.
The tumor is rotated upward or downward depending on the direction of the facial nerve.
The Transcochlear Approach 7
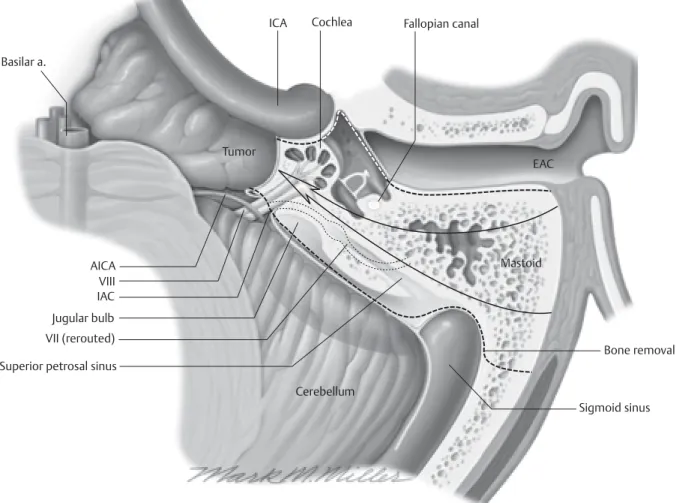
Careful handling and constant monitoring of the facial nerve during rerouting prevents damage to the intratemporal portion of the nerve. The periosteal flap is elevated to the spine of Henle and to the level of the external auditory canal. In some cases of far anteriorly located lesions, removal of the external ear canal is necessary.
The dissection of the perilabyrinthine cells down to the lateral semicircular canal is completed (Fig. 7.5). The facial nerve is identified in the vertical portion between the unampulated end of the lateral semicircular canal and the stylomastoid foramen. The junction of the intracranial portion of the facial nerve and the skeletal intratemporal portion has now been identified.
The opening of the mastoid cavity is expanded posterior to the sigmoid sinus, exposing 1 to 2 cm of suboccipital dura.
The Combined 8
Petrosal Approach to the Petroclival Region
A combined petrosal approach is used to access extensive lesions of the petroclival region. A key difference between the combined petrosal approach and other approaches to the lateral skull base is the transection of the tentorium cerebelli. Alternatively, the anterior limb of the skin incision is extended inferiorly, in the preauricular region.
Completion of the transmastoid drilling is facilitated by removal of the middle fossa bone plate. A posterior/inferior extension of the craniotomy window can be performed to fully decompress the middle fossa dura (Fig. 8.4). Division of the tentorium cerebelli must be performed behind the insertion of cranial nerve IV in the dural folds.
Venous drainage of the inferolateral temporal lobe in relation to transtemporal/transtentorial approaches to the cranial base.

The Far Lateral Approach 9
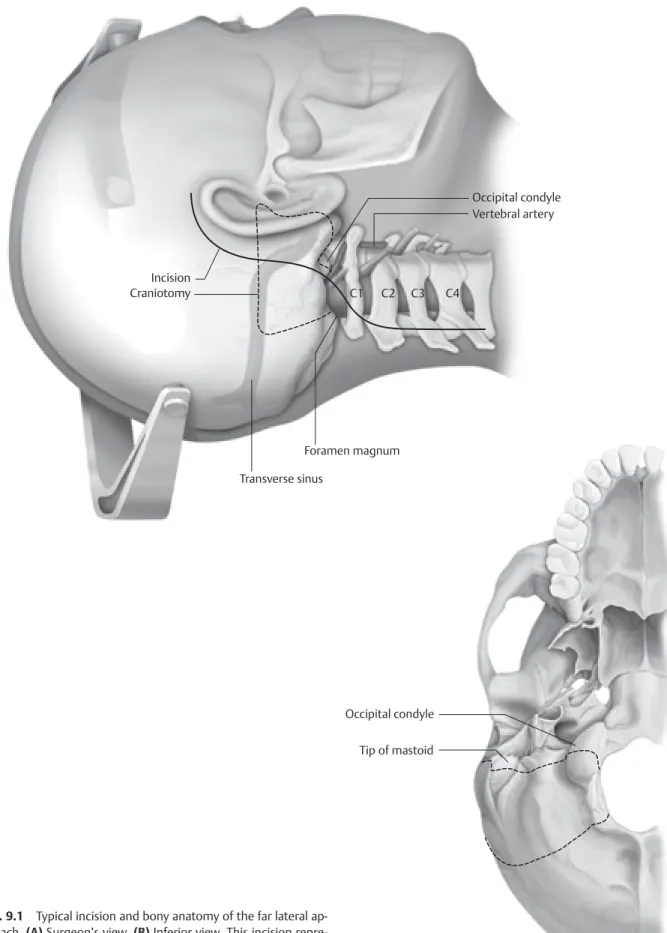
The hypoglossal nerve often crosses the vertebral artery at the origin of the posterior inferior cerebellar artery. Additional bone is then removed to transfer the bony opening to the horizontal part of the occipital bone. Extent of bone removal up to the foramen magnum and the posterior edge of the occipital condyle.
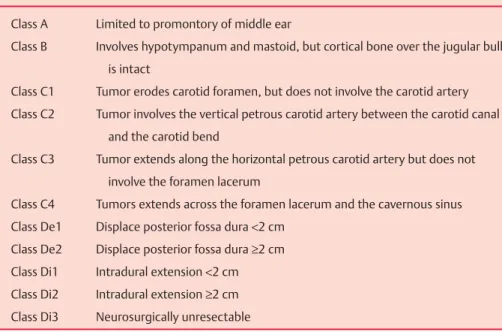
Resection of the jugular tubercle can be performed intradurally (in the same way as intradural resection of the anterior clinoid process) or extradurally. Review preoperative imaging to understand the anatomy of the vertebral artery and any anatomic variations. Quantitative description of the far lateral transcondylar transtubercular approach to the foramen magnum and clivus.
Quantitative analysis of variants of the farlateral approach: condylar fossa and transcondylar exposure.
The Fisch Infratemporal Fossa 10
Approach: Type A
The skin of the external auditory canal is then elevated away from the underlying cartilage. Tumor intimately involving the facial nerve should be removed with small scissors at the end of the dissection. The carotid artery should be followed distal to the tumor to ensure safe removal of the tumor.
The jugular vein is then passed under the accessory spinal nerve to the level of the jugular bulb. The medial wall of the jugular bulb is a useful plane between the tumor and the lower cranial nerves. When displacing the facial nerve outside the fallopian tube, use sharp dissection for the medial attachments.
Use the medial wall of the occiput as a plane between the tumor and lower cranial nerves.
The Fisch Infratemporal 11
Fossa Approach
Types B and C
The muscles of the infratemporal fossa include the medial and lateral pterygoid muscles and the temporalis muscle. This layer encloses the frontal branch of the facial nerve and the superficial temporal artery. This incision extends to the level of the superficial layer of the deep temporal fascia.
The nerve lies in the plane deep to the superficial temporal fascia and the superficial layer of the deep temporal fascia. The anterior limit of the dissection is partially limited by the frontal branch of the facial nerve. The zygomatic arch acts as the main barrier for the inferior mobilization of the temporalis muscle.
Great care is taken to avoid stretching the anterior branch and main trunk of the facial nerve.
The Preauricular 12
Infratemporal Approach
If the tumor is highly vascular on imaging, obtaining a biopsy of the lesion is not recommended. The frontal branch of the facial nerve passes within or just deep to the temporoparietal fascia at the level of the superior orbital rim. Under a microscope, the dura of the temporal lobe is elevated with an elevator from the middle cranial fossa floor.
A compression bandage can be placed, but only if there is little risk of vascular compromise of the reconstruction. A cosmetic deformity may result from atrophy or loss of the temporalis muscle attached to the anterior temporal fossa. The preauricular infratemporal approach provides excellent access to the contents of the infratemporal fossa from above.
The advantage of the top approach is the minimal risk of morbidity to the facial nerve and the absence of postoperative hearing loss.

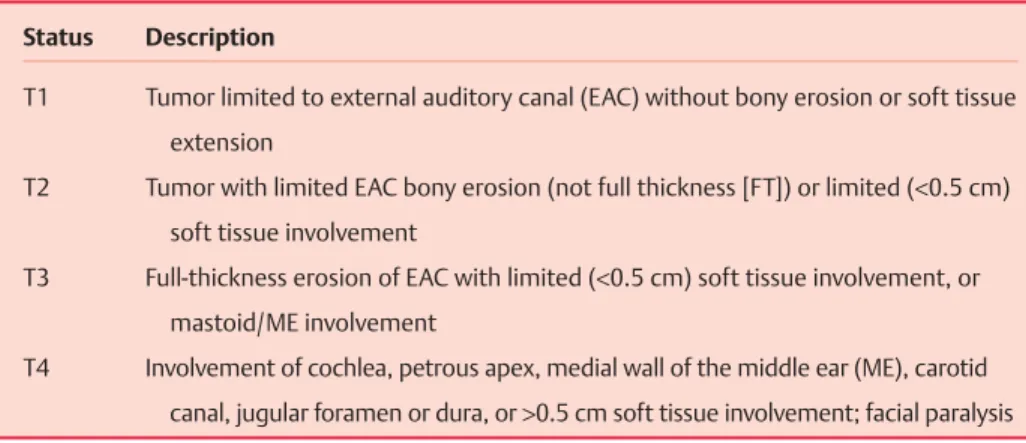
Temporal Bone Resection 13
Lateral resection of the temporal bone is used for tumors lateral to the tympanic membrane without involvement of the mastoid. This dissection moves forward to the anterior wall of the mastoid tip, to the periosteum of the mandible. Bone flakes along the dura can be sent to the pathology laboratory as a medial margin specimen.
Continuing the dissection of the posterior semicircular canal below leads to the jugular bulb, which is skeletonized. Mobilization of the nerve can cause temporary facial paresis (House-Brackmann grade 3 or 4). The pterygoid muscles can be resected along with any large tumor of the infratemporal fossa.
The outcome of radical surgery and postoperative radiotherapy for squamous cell carcinoma of the temporal bone.
Microvascular Cranial 14
Nerve Decompression
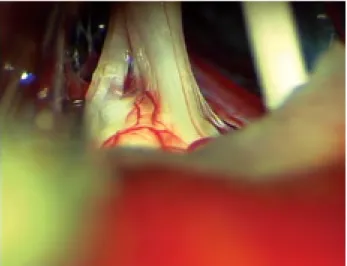
An inferior dural opening is made, extending to the lower edge of the exposed sigmoid sinus. It is necessary to visualize the entire length of the trigeminal nerve from the pons to the entrance to Meckel's cave (Fig. 14.1). Decompression of the facial nerve is particularly difficult because of its proximity to the vestibulocochlear nerve, which is particularly vulnerable to trauma, including distension.
Branch loops of the anterior inferior cerebellar artery (AICA) may be located along the course of the facial nerve in the cistern. Examination of the surface of the brain stem at the entry zone of the root of the facial nerve is also mandatory. AICA or posterior inferior cerebellar artery (PICA) loops may be in contact with the facial nerve or its root entry zone.
A loop of the AICA is often found at this location and in contact with the nerve.
Complications of 15
Neurotologic Surgery
In any surgical approach to the acoustic neuroma, the pneumatized air cell system of the temporal bone is entered, and a potential communication between the temporal bone and the subarachnoid space may persist, resulting in leakage of CSF through the skin incision or the eustachian tube ( posing as a youth). Air cells or dehiscences on the floor of the middle cranial fossa are depilated or covered with fascia. Management of the patient with postoperative CSF leak should be tailored to the patient's hearing status as well as the site of the fistula.
This is done so that the anterior bony ring can be removed to expose the introitus of the eustachian tube. This technique allows for an interruption of communication with the middle ear without relying on Eustachian tube packing materials that can potentially become porous or non-obstructive over time. The apex of the semicanal for the tensor tympani is removed and the eustachian tube is identified inferiorly.
If indicated, preoperative balloon occlusion angiography of the internal carotid artery (ICA) may be performed.