An empathic therapist tries to experience the world from the client's perspective without judgment or criticism. Empathy involves a nonjudgmental attitude in which the therapist tries to see the world from the client's point of view. What this implies is that behaviors are more understandable when understood from the customer's perspective.
In MI, the therapist pays particular attention to the client's arguments for change, compared to his or her arguments for not changing. In MI, the therapist strives to understand and respect both sides of the ambivalence from the client's perspective. In the first, the client is ambivalent about change and motivation may be insufficient to achieve change.
In MI, the client should do most of the talking, and open-ended questions are used to achieve this goal. In particular, summaries are used to collect and reinforce "change talk," the client's own statements of motivations for change.
MI: Commitment and Action
When the therapist notices that the client may be moving toward a resolution of the ambivalence, an open-ended question is asked such as, "What do you think you are going to do right now?" could be used. The MI style encourages a change plan that comes primarily from the client, not the therapist. The role induction interviewer discussed the rationale for the therapy with the client and the client's and therapist's expectations in the therapy process.
MI can offer advantages in cross-cultural counseling, particularly because of the therapist's focus on understanding the client's unique context and perspective. Furthermore, when barriers to change are empathically explored, reasons for change often emerge naturally and spontaneously in the client's words. One of the strengths of MI is that it encourages the client—rather than the therapist—to articulate the reasons for change.
The therapist facilitates the client's exploration and elaboration of arguments for change, addressing both the negative sides of anxiety/avoidance as well as the potential advantages for change. As this example illustrates, communicating the therapist's agenda can be quite subtle, but still chosen by the client. In this example of MI, the therapist is empathically resonating with the client's expressed dilemma (trying to understand it from her perspective).
The client is not instructed that he or she should do this (or any technique), but it is simply offered as part of the process of collaboration.
Group Review and Possible Problem Identification
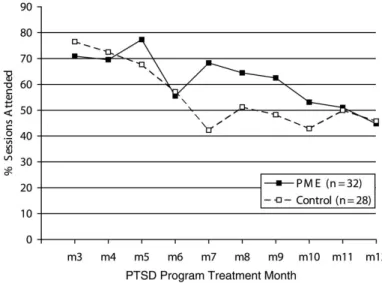
The rationale for the PME group is that increased recognition of the need to change specific PTSD symptoms and other problems will lead to better treatment adherence and outcome because patients will view coping skills learned in treatment as more personally relevant to they. As explained to the patients, the purpose of the group is to help them avoid being "blindsided" by unrecognized problems after treatment. In addition, a key part of the intervention, assessment of possible unrecognized problems, takes place in this first session.
Participants then use decision-making tools taught in subsequent PME group sessions to help them decide whether these "Might Have" problems are actually problems they definitely have. Homework is also given after each of the first three sessions, including reading in preparation for the next session and completion of additional session-specific decision-making activities. As presented to group participants, the purpose of the group is to help patients make decisions about problems they may have that are either definitely or definitely not a problem that requires change.
There is a clear difference between problems listed as "Maybe" and behaviors and cognitions they are certain they need to change. At the end of the rationale review, the therapist emphasizes that the ultimate goal of the group is to help patients avoid being “blindsided” by unrecognized problems after discharge. The section of the PME group that deals with this issue tries to walk the fine line between being overly directive and encouraging people to take responsibility for managing symptoms (often not seen as symptoms, eg distrust, isolation, "controlling" or perfectionistic).
In particular, one goal of the PME group is to help participants understand that unrecognized issues can contribute to their problems, that their past traumatic experiences can influence their responses to situations that trigger or worsen symptoms or cause difficulties for them, and that she may need to take more responsibility for dealing with difficult situations. As in all parts of the assessment of the group's rationale and purpose, group leaders ask patients for answers and feedback on the questions asked, and also read out the desired answer. Each group participant also reads one of the statements from the “Self-Talk Checklist for Continued Progress After Treatment.” This checklist is included in appendix 3.2.
The goal is for patients to eventually sort the items listed under "Maybe" into "Definitely Have" or After the participants have had some time to complete the worksheet, they are asked to read aloud what they have listed in each of the four columns. Does success in this group mean you have to move all the mightiness out of the middle columns.
Pros and Cons”
I bring the issues I definitely have to the other Trauma Recovery Program and PTSD treatment groups where I can work with them. Homework is assigned before the group ends; specifically, it is suggested that patients read sections of the patient workbook that review this first session and also the upcoming session on decisional balance.
Comparison to the Average Guy
Roadblocks
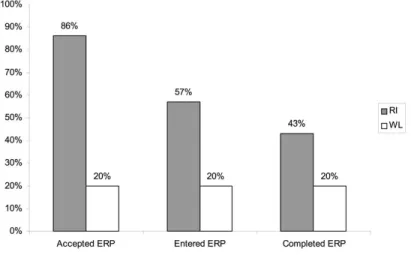
The group process—particularly seeing peers engage in the group's self-exploration activities—also seemed to encourage Albert to think about the need for change. The purpose of this activity was to provide a realistic example of the effects of ERP. This also led to a discussion about the elements that can block habituation (avoidance, safety cues, not repeating, not staying in the situation until anxiety levels are reduced).
At the end of the readiness intervention, her fear of starting ERP, now at 50 to 100-. We conducted a small pilot RI study with 12 OCD patients who refused treatment (see Maltby & Tolin, 2005, for a full description of the study). From the data, it appears that the decision to enter ERP treatment was most strongly associated with decreased fear of treatment.
Motivational interviewing (MI; Miller & Rollnick, 2002) emphasizes the meeting of patient and therapist treatment aspirations within a client-centered relationship. I could definitely use some help dealing with some of the things going on. The rest of the week I have to be at work and take care of Johnny.
Therapists may choose to look for moments in the standard interview in which they can insert elements of the engagement session—. Paper presented at the annual meeting of the Society for Psychotherapy Research, Montreal, Canada. In this sense, motivational interviewing is an evolution of the client-centered approach that Rogers developed.
We found that working with MI in the action phase can be done in the context of the spirit of MI and can use MI methods as well as those of other therapeutic approaches. We believe that it is most beneficial if the therapeutic strategies used are implemented in the context of the spirit of MI. At Level 2, the focus was on the need to express and process some of the emotions associated with the abuse.
Over the next four sessions, we explored her ambivalence about talking about the abuse. So far, there are no controlled studies on the effectiveness of MI in depression. Subjects in the motivational group showed a large reduction in Beck Depression Inventory scores at the end of the first 30 days of outpatient treatment.
The results of the studies reviewed above tentatively suggest that MI may be effective for depression.