Today, 'orthopedic treatment' is associated with the latest complex technology, which is mostly not applicable in the tight environment. It is a great pleasure to write a foreword to this new book on trauma surgery in the harsh environment.
Part III Management Challenges in the Austere Environment
Ian Pallister, FRCS (Ed) FRCS DA (UK) DTM&H Departamento ti Trauma ken Ortopedia, Ospital ti Morriston, Unibersidad ti Swansea, Swansea, Wales, UK. David Shearer, MD, Departamento ti Ortopediko a Operasion ti MPH, Unibersidad ti California San Francisco, Sapasap nga Ospital ti San Francisco, Instituto ti Ortopediko a Trauma, San Francisco, CA, E.U.A.
Setting the Scene: The Austere Environment
How to Prepare for a Mission in a Confl ict or Disaster Zone
- Skills and Experience
- Invitation to Respond
- Coordination
- Standards
- Authorisation to Practice
- The Exceptional
- Make Sure This Work Is for You It is not without risk. It will place considerable
- Join an Established Organisation
- Mental and Physical Fitness Working in an austere environment requires a
- Garnering Core Skills and Competencies
- Completion of Training in a Relevant Surgical
- Surgical Training for the Austere Environment
- Experience Beyond Surgery Public health and emergency medicine bring a
- Understanding the Context in Which You Will Work
- Field Training
- Field Craft
- Communications
- Safety and Security
- Departure
It is especially important to understand the principles of public health that apply to unexpected disasters. To be most effective in this area, it is important to understand the nature of conflicts and disasters.
Understanding Your Working Environment
- Category 2: Developing Country with Higher Level
- Category 3: Less-developed Country
- Category 4: Non-state Actors, Guerrilla Groups
- Category 5: Non-man-made Disaster, Earthquake,
The medical emergency response team (MERT) helicopter flies to the scene of the injury, and the patient is transported back to the Role 3 Field Hospital at Camp Bastion. You will be limited in what you can do in this environment and to consider the surgical aspects of the hospital, as a dressing station may be the best option (Fig. 2.3.
Epidemiology of Fatalities
Methods
- Wars and Armed Confl icts
- Natural Disasters
- Other Causes of Fatalities and Trauma
- Strengths and Limitations of the Information Sources
Many of the available information sources were also inaccurate in specifying information such as the exact number of fatalities, non-fatal injuries and casualties (fatal and non-fatal injuries combined), the year and country in which the fatalities and casualties occurred, the affected troops (often troops from other countries). There was also a lack of reporting or other evidence for some forms of fatalities and trauma, such as animal attacks and industrial accidents, in less developed countries.
Wars and Armed Confl icts
- Type of Confl ict, Geography and Fatalities
- Causes of Casualties: Type of Device
- Explosive Devices and Fragments
- Anti-tank Mines
- Anti-personnel Mines
- Gunshot Wounds
- Other Devices: Stab Wounds, Burns and Infections
- Anatomical and Tissue Type Distribution
- Head and Neck Injuries
- Thoracic Injuries
- Abdominal Injuries
- Injuries to the Limbs
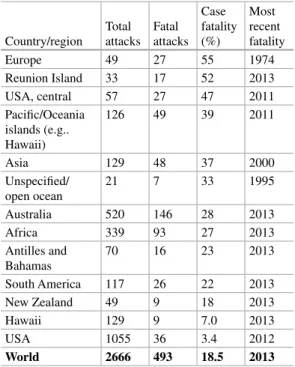
- Case Fatality
Infections are often a major cause of mortality and morbidity in wars and armed conflicts. Abdominal injuries usually account for up to 20% of casualties in wars and armed conflicts (Table 3.5.

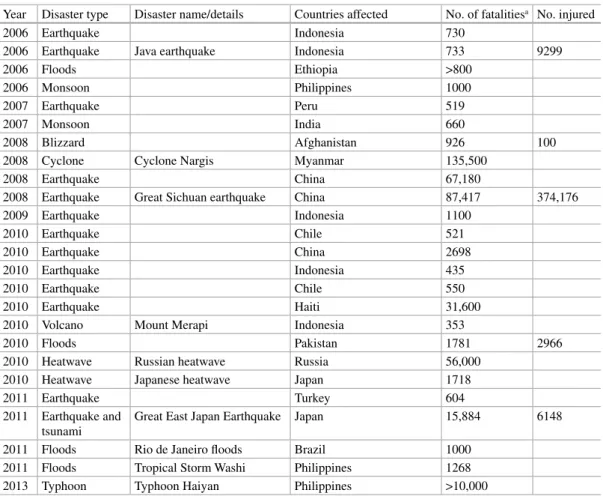
Natural Disasters
- Type of Natural Disaster, Geography and Fatalities
- Causes of Natural Disasters Natural disasters can be classifi ed into four cate-
- Geophysical Disasters
- Earthquakes and Tsunamis
- Volcanoes
- Meteorological Disasters
- Typhoons
- Hydrological Disasters
- Floods
- Climatological Disasters
- Heatwaves
- Wildfi res
Other earthquakes since 1990 that have caused many deaths have occurred in Afghanistan, China, Haiti, Iran, Pakistan, and Turkey (Table 3.8; Figures 3.5 and 3.6). Since 1990, typhoons (or cyclones/hurricanes) have been responsible for more than 300,000 deaths worldwide, mainly in Bangladesh, the Philippines, the United States, and the Gulf of Mexico (Table 3.8; Figures 3.5 and 3.6.
Other Causes of Trauma
- Animal Attacks
- Snakes
- Crocodiles and Alligators
- Other Animals
- Occupational Injuries
- Road Traffi c Accidents
Road traffic accidents are one of the world's leading causes of traumatic injury and death and. Epidemiology of venomous and semi-venomous snakebites (Ophidia: Viperidae, Colubridae) in Kashan City of Isfahan Province in Central Iran. Terrestrial snakebites in the southeastern Arabian Peninsula: patient characteristics, clinical presentations, and management.

Is Evidence-Based Orthopedic
Traumatology Possible in the Low- Resource Environment?
- Why Conduct Research?
- Identifying Partners
- The Research Question
- Feasible
- Interesting
- Novel
- Ethical
- Relevant
- Choosing a Study Design
- Implementing a Study Protocol
- Summary
This may lead to the selection of a less rigorous study design to make completion of the study more feasible. At the same time, it is important that the principles of quality design are not compromised because the study is carried out in an environment with low resource consumption. At the same time, although some questions may have been studied previously, it is important to consider whether the findings are generalizable to the setting in which the study is proposed.
Cultural, Legal, and Ethical Considerations
- Are You Prepared?
- Safety First
- Patient Autonomy
- Relationships with Colleagues
- Training
- Equal Rights
- Fostering Resilience
- Research
- Your Own Safety
- Case 1
- Discussion
- Case 2
- Discussion
- Case 3
- Discussion
Instead of describing "the way this is done," always talk about "a way it is done." By describing certain methods as superior, the visiting surgeon may undermine not only the local physician's confidence, but may risk shaming or offending certain members of the medical hierarchy. While this is certainly understandable with few resources, it can also hinder the development of a sustainable local health system. Also, we don't have the new sheets that you're using, and all our other sheets we have aren't sterile.” The surgeon closes and the patient is taken to the recovery room.
Causes of Trauma in the Austere Environment
Motor Vehicle Accidents
The Scourge of the Developing World
- Road Traffi c Injuries
- Epidemiology
- Own Experience
- Earthquakes
- Tsunamis
- Tornadoes
- Hurricanes/Tropical Cyclones/Typhoons
- Floods
- Avalanches, Mudslides, and Other Causes
- Management Principles
- Wounds
- Amputations
- Fractures
RTIs were the most common cause of injury-related death, and for nonfatal injury, the extremities were the most injured part of the body. First aid for wounded victims, search and rescue efforts and initial medical management of the injured are secondary priorities in the initial stage. One of the most common chronic complications was persistent cutaneous infection with mixed and unusual pathogens.
Orthopedic Ballistic Trauma
- Treatment Principles
- First Steps
- Intra-articular Bullets
- Compartment Syndrome and Fasciotomies
- Fracture Management
- Soft Tissue Management
- Amputations
- Physiotherapy
This is the part of the bullet trajectory with maximum energy transfer, the amount of which can be visualized by the volume of the abdominal part. The final channel can be single or multiple according to a possible fragmentation of the bullet. The kinetic energy is directly proportional to the mass while it is proportional to the square of the velocity.

Orthopedic Blast and Shrapnel Trauma
Biophysics of Blast Trauma All explosive weapons are composed of three
After the initial blast wave has dissipated, blast-activated ballistics can cause severe penetrating or shear damage. Secondary blast injuries are more common than primary injuries because these ejected fragments typically travel long distances at high velocities and the effective range for such injuries exceeds that of the blast wave by a factor of. Tertiary blast injuries involve displacement of the victim's entire body, or crush injuries.
Initial Management of Blast Injuries
- Spanish Windlass Technique 1. A piece of rubber tubing (not narrow) is
- Index Surgical Procedure
The tourniquet should be placed as close to the limb as possible, outside the zone of injury. Prophylactic fasciotomies of the bone compartments should be considered in all patients with tibial fractures undergoing external fixation. Repeated irrigation and debridement are essential, as the zone of injury continues to develop in the context of the systemic inflammatory response.
Defi nitive Management of Blast Wounds
Microbial profiling of combat wound infection by detection microarray and next-generation sequencing. Temporary vascular shunts as initial treatment of proximal extremity vascular injuries during combat operations: a new standard of care in Echelon II facilities. The Range of Wounds Encountered by Victims of the Global War on Terror: From the Battlefield to the Tertiary Treatment Facility.
Injury from Traditional Bonesetter Fracture Management
- What Is a “Bonesetter”?
- Who Do Bonesetters Treat?
- Why Do People Go to Bonesetters?
- Complications
- Management of Complications Secondary to Bone Setting
- Case Study
- Case 1: Early Presentation
- Case 2: Late Presentation
- What Can Be Done
Of the many complications that result from bone setter treatments, one of the most tragic is gangrene secondary to tight bandages. The cases below illustrate examples of the consequences of some of the practices by bone setters. The next day, examination of the limb showed reduced swelling, normal sensation through the fingers and hand, and normal movements.
Management Challenges in the Austere Environment
Malnutrition and Orthopedic Injuries
- Epidemiology
- Defi nition and Evaluation of Malnutrition
- Consequences of Malnutrition
- Management
- Preoperative Treatment
- Postoperative Treatment
- HIV/AIDS: The Disease
- Closed Fractures
- Wound Healing
- Fracture Union
- Late Implant Sepsis
- Open Fractures
- Wound Infection
- Microbiology
- Pin Site Infection
- Fracture Union
- Functional Outcome
- Polytrauma
- Osteoporosis and Fragility Fractures
- Working with Patients Who Are HIV Positive
HIV disease can be classified according to two general classifications - The World Health Organization (updated 2005) and the Center for Disease Control (updated 2008) classifications [4, 5.
Malunion, Non-union and Delayed Presentation: The Norm,
Malunion
- Long Bone Malunions
- Upper Limb
- Lower Limb
- Malunions Around Joints and Neglected Dislocations
Malunions of the distal radius can also result in significant loss of function; the most common treatment for this is corrective osteotomy and fixation. Malunions of the femur and tibia may be acceptable depending on the degree of severity (Figs. 13.2 and 13.3. In young and physically challenged patients, or if arthroplasty is not available, joint arthrodesis may be the best option of treatment (Table 13.1.
- Aetiology
- Classifi cation
- Management of Aseptic Non-union
- Optimisation of the Patient’s General Health
- Increased Mechanical Stability Without Bony
- Resection Back to Viable Bone
- Provision of Appropriate Mechanical Stability
- Provision of Biologic Stimulus
- Soft Tissue Reconstruction Vascularised soft tissue cover is desirable in non-
- Polytherapy
- Infected Non-union
- Classifi cation
- Management of Infected Non-union
- Limb Salvage for Infected Non-union
- Optimisation of Patient’s General Health
- Radical Surgical Debridement
- Skeletal Stabilisation
- Dead Space Management
- Soft Tissue Reconstruction It is important for debrided bone to be covered
- Targeted Antibiotic Therapy Ideally , several samples from the surgical debride-
- Bony Reconstruction
In some cases of long bone nonunion, additional stabilization of the fracture using closed methods may be all that is required for union to occur. The management of dead space is now recognized as an important part of the management of osteomyelitis and infected non-union [69. Treatment of infected nonunions and segmental defects of the tibia with staged microvascular muscle grafting and bone grafting.
Pathophysiology
Environmental factors include poor access to clean water, poor infrastructure and lack of access to high-quality health care (Fig. 14.1. If the host's response (+/− antibiotics) is sufficient to stop further bacterial spread and the abscess is 'shielded' the infection can be remarkably well tolerated by the patient (subacute osteomyelitis) or actually subside.Pus may track circumferentially around the bone, break through the periosteum into the soft tissue, or continue down the bone in an intramedullary manner ( Fig. 14.3.
Management ofOsteomyelitis
Acute Osteomyelitis
- Surgery for AO
If a child has bone pain, especially in the shin, no blood tests are available and X-rays will not show any changes. In particular, check whether the percussion is sensitive at the point of pain.
Subacute Osteomyelitis
Chronic Osteomyelitis
Preoperative Care and Investigations
- Preoperative Planning
- Surgical Equipment
Surgical planning should include identification of all active sinuses, examination of the superior and inferior joints preoperatively to evaluate for septic arthritis, and identification of any soft tissue collections. The Beit CURE classification [14] is a radiological classification that is useful in surgical planning of the disease. Although less well known than the Cierny-Mader classification [15], it was developed specifically for use in resource-poor settings and is a valuable tool in surgical planning as well as in comparative research.
Infection Control Surgery
Patients with systemic signs of sepsis should be given antibiotics, as well as fluids and oxygen if available. However, if there is no structural involucre after 3 months of follow-up, a sequestrectomy should be performed and the bone defect treated subsequently. Similarly, if a sequestrectomy is performed (leaving a bony defect), the bone should be stabilized for 3 months to allow a structural involucre to form.
Soft Tissue Management
When the sequestrum is identified, a level between it and viable bone should be developed using an elevator or probe to loosen it, which can then allow removal in one complete piece using hemostats. Some advocate that the sequestrum remain in place until the periosteum has laid down sufficient structural envelope. The advantage of this approach is that the sequestrum is ideally situated to provide structural support while waiting for casing to form.
Dead-Space Management This refers to the management of the void that is
There is controversy regarding the timing of sequestrectomy in those cases where the sequestrum provides stability, when the involucrum is not structurally sufficient. The disadvantage is that the longer the infected sequestrum remains in place, the more likely it is that the periosteum will be damaged, potentially jeopardizing the formation of quality involucrum. The advantage of this approach is that infection control is achieved at an earlier stage, and this potentially protects the periosteum.
Bony Stabilisation
Others advocate removing the "structural sequestrum" as quickly as possible, leaving a bone defect that requires stabilization with plaster or framing. There should be good quality cortical continuity in 3 of the 4 cortices on the AP and lateral radiographs to ensure stability. If more than one-third of the bone in a given segment is resected intraoperatively, the limb should be immobilized for six weeks and weight restricted to control the risk of fracture.
Bone Defects
Postoperative Care
- Follow-up
- Rehabilitation
Complications
- Cautions
Bone tumors (primary and secondary) – can present in a very similar way to osteomyelitis and can have very similar x-ray appearances. Resistant / atypical bacteria – although less common in the developing world, resistant bacteria (eg MRSA) can still occur.
- Tutorial 2
- Tutorial 3
Note the creation of a window in the medial border of the tibia and the absence of the sequestrum that is on the front. He has had no exuding wounds for 6 months, but is now unable to bear weight at all. Bone transport.] He requires plaster immobilization for many months but continues to heal (Fig. 14.7c.
Summary
Note the formation of a window in the medial border of the tibia and the absence of the sequestrum, clearly visible on the previous radiograph. 14.7 (a) Radiograph of a boy who presented with a two-year history of leg pain and previously discharged sinuses. b) Contralateral free fibula graft with ipsalateral. Treatment of bone defects in children caused by chronic hematogenous osteomyelitis: a retrospective review of 57 patients.
Types of Bone Defects
- Contained Defects
- Segmental Defects
- Distraction Osteogenesis
- Interposition Techniques
- Non-vascular Tissue Autograft
- Vascular Tissue
Tibialization of the fibula, where the ipsilateral fibula is used to fill a segmental gap in the tibia, has also been reported by some authors to have good results. Cancellous bone blocks and rigid fixation to bridge bony gaps have been described by Nicoll [29] and have shown good results in the upper limb [30. This is done in two stages; in the first, a cement spacer is used to fill the bony defect.
- Articular Defects
What About the BMP?
Distraction osteogenesis using a monolateral fixator for infected femoral nonunion with bone loss. Nonvascularized fibular graft as an intramedullary strut for infected nonunion of the humerus. Vascularized free fibula for the treatment of traumatic bony defects and nonunion of the forearm.
Perioperative Management in the Austere Environment
What? No Lab? Preparing the Patient for Operation
Laboratory Medicine
- Social and Economical Concerns
- Quality
Clinical decisions often occur without laboratory confirmation, even when tests were available. Conversely, when tests are performed and results conflict with clinical judgment, treatment may be based on clinical judgment alone [ 2. They may be performed in marginal health facilities with little technical expertise and require minimal sample preparation. - tion or preservation and are kit-based (with reagents resistant to extreme temperatures).
Preparation for Surgery
- Preoperative Laboratory Test Laboratory investigations in austere environment
Therefore, the infrastructure of public health care, although inadequate, is gradually destabilized by these competing parallel systems [ 2. The problem is further complicated by the decentralization of the health care system, in which governmental, non-profit (e.g., missionary or private philanthropic) or commercial (for-profit) organizations often manage independent laboratories, thereby creating a parallel environment of donors of varying quality levels, which is somewhat confusing. In conclusion, confirmation of the critical importance of basic and high-quality (albeit affordable and sustainable) laboratory testing among clinicians, NGOs and policy makers is mandatory to ensure more effective treatment and optimize the use of healthcare resources. .