The publisher makes no warranty, express or implied, with respect to the material contained herein. Alpert expertly discusses in detail, the history provides clues to the clinical diagnosis while the complementary neurological examination localizes the lesion(s).
Acknowledgments
A rapid CT scan of the brain revealed prominent subcortical ischemic changes, greater on the right than on the left. A subsequent brain MRI scan confirms vascular pathology due to multiple scattered T2 hyperintensities.
Common Neurologic Signs
Localizing Value
Cerebral
The patient asks the resident, "When will I be transferred?" then say, "I mean dismissed." The patient is alert, has fluent speech and is oriented to person, place and month. When asked to repeat "no ifs, etcs or buts," he replies "no ifs, ands, and buts." The remainder of a complete neurological examination is normal.
Extrapyramidal
However, the patient has a positive glabellar reflex, known as Myerson's sign, which is a rapid, sustained blink when the bridge of the nose is tapped. Paying attention to the patient's facial mobility and leg movements provide the two primary diagnostic clues.
Brainstem/Cerebellum
Left heel-to-shin ataxia is consistent with involvement of the left inferior cerebellar peduncle (restiform body). Hypoesthesia on the right side of the body indicates involvement of the lateral spinothalamic tract on the left side.
Spinal Cord Lesions (Myelopathies)
In this case, this is due to the involvement of the corticospinal tract in the spinal cord. The sympathetic nervous system is represented in the intermediolateral cell column of the spinal cord.
Radiculopathy
Medial calf sensory loss is due to involvement of the saphenous branch of the femoral nerve. This is a sensory branch of the femoral nerve and is rarely involved in lumbar radiculopathies.
Plexopathy
Neuropathy
The ulnar nerve is often exposed to injury in the cubital tunnel at the elbow. The peroneal nerve can be compressed in the popliteal fossa, causing a dropped foot and a "step-page" gait.
Neuromuscular Junction
She has had rheumatoid arthritis for 12 years and has multiple joint deformities affecting wrists, proximal interphalangeal joints and knees.
Myopathy
Meningeal Disease
A traumatic tap is virtually excluded due to the presence of xanthochromia in the supernatant after centrifugation of the spinal fluid. In the first hours after a subarachnoid hemorrhage, the spinal fluid often looks pink, which is due to oxyhemoglobin.
Synopsis
Early signs may be distal sensory loss to temperature and pin (small fiber) and/or decreased vibratory perception distally (large fiber).
Multiple Choice Questions
Answers
Cerebral disease does not cause fasciculations or pain and usually affects the distal musculature. Neuroimaging is accurate, but if the wrong structure is imaged, it is worthless.
Bibliography
An MRI scan of the lumbar spine may be completely normal, which baffles the patient's doctor. Conversely, a herniated disc with nerve root compression can be treated surgically without relieving the patient's symptoms due to a brain tumor.
The Neurologic History Holds the Diagnostic Keys
The neurologist questions the patient, who expresses some annoyance and resists his insistence on clarifying her comment: "They don't last very long." Finally, she responds to the question, "Do they keep seconds, minutes or closer to an hour?" She replied, "Closer to an hour." "Do you have a headache?" "No." "Does your eye or head hurt afterwards?" "Of course my eye and forehead hurt a little." "Have you ever had bad headaches?" "I used to get bad sinus headaches during allergy season in my 20s." "Were you ever nauseous with them?" "Sometimes, but usually in the sun when my headache was worse." The diagnosis is migraine. This patient exhibited the cry-for-help syndrome, that is, "take me seriously." The take-home lesson is never dismiss a complaint despite circumstances implying dishonest behavior.
Neurologic Symptoms in Psychiatric Disease
When leg weakness is one of the symptoms, the patient is examined on his back and asked to raise one leg. As noted by Max Wintrobe, the eminent internist, “Physical examination should be done with a watchful eye, a sensitive touch, a perceptive ear, and a keen sense of smell.
Vital Signs
Above all, what is needed is an alert mind free from dogma and routine.” Nowhere is this more essential than in the specialty of neurology. Despite the detailed description of required observations, a thorough neurological examination is easily completed within 15 min in an uncomplicated patient.
Neurologic Examination
Blood pressure should be measured in both arms to assess for subclavian stem syndrome. If there is a history of loss of balance, blood pressure should be monitored while standing if no other obvious etiology is found.
Mental Status Examination
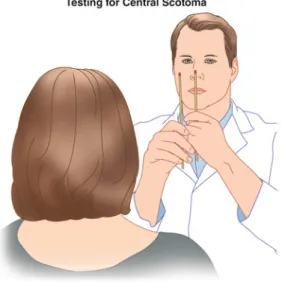
Autotopagnosia refers to the patient's inability to recognize their own limb or body part. The patient receives two touch stimuli, one on each side of the body, on different parts.
Cranial Nerve Examination Olfactory Nerve (I)
The main sensory nucleus is located in the rostral part of the pons just to the side of the motor nucleus. Briefly, the right cerebral hemisphere initiates head movements to the opposite side.
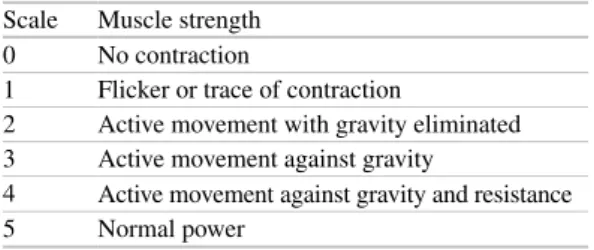
Motor Examination
Among the first observations made upon entering the examination room are those of the patient's posture and movements. Spasticity of the arm can be most easily evaluated by rapid supination movements (biceps) of the patient's relaxed arm.
Gait and Station Examination
The patient walks slowly with a wide base, short stride and often reaches out for support. Astasia-abasia is typically found in the patient with a conversion reaction who makes wobbly, irregular steps.
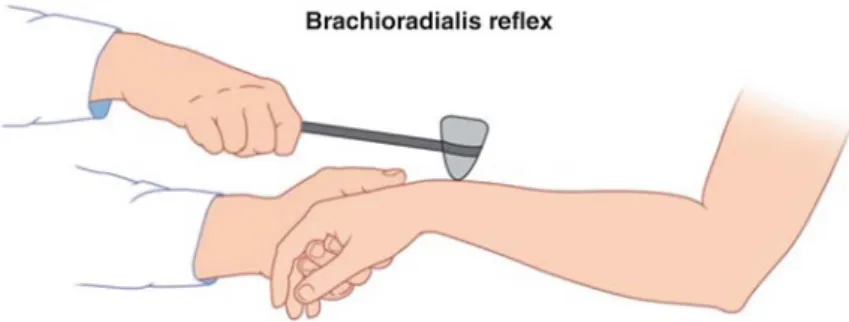
Reflex Examination
The foot is partially dorsiflexed by placing upward pressure on the ball of the foot. Reflexes of doubtful significance The snout reflex is elicited by tapping the patient's upper lip.
Sensory Examination
Lesions of the sensory cortex tend to involve the hand, and loss of position sense is preferentially involved. There is a tendency for the arm to be involved and position sense is preferentially involved.
Dermatome Patterns (Fig. 4.18)
L4 is the medial part of the big toe, L5 is the medial part of the dorsum and sole from the big toe to the fourth toe.
Mechanical Signs Meningeal Disease
Questions (True or False)
The primary question when evaluating a poorly responsive patient is to distinguish between a focal lesion, multifocal lesions, or global cerebral dysfunction. The definition of the levels of impaired consciousness has been a source of debate for many years.
Clouding of Consciousness (Lethargy)
A goal of this chapter is to outline an examination technique, outline the anatomic basis for the observed abnormal neurologic signs, review the relevant neurophysiology, and finally, discuss the differential diagnosis. The best approach is to simply describe what the patient is able to do spontaneously.
Delirium
Evaluation of the Poorly
Obtundation
Stupor
Coma
Unilateral loss indicates a focal lesion of the unilateral 9th and/or 10th cranial nerves or ipsilateral nucleus in the medulla. Spasticity is best manifested in the arms by rapid pronation and supination movements of the forearms.
Metabolic and Hypoxic-Ischemic Encephalopathies
Finally, an EEG may be necessary to rule out nonconvulsive status epilepticus and to assess the severity of the encephalopathy. These are located in the striatum (caudate nuclei and putamen), the cerebral cortex, the CA1 region of the hippocampus and the cerebellum, especially in the Purkinje cells.
Prognostic Factors in Comatose Survivors After CPR
These are located in the border zones between the MCA and the anterior cerebral artery (ACA), MCA and the posterior cerebral artery (PCA), and the border zone between the deep and superficial branches of the MCA. Clinical correlates of subcortical infarcts, involving the superficial and deep branches of the MCA, invariably include hemiparesis and often aphasias of various types in dominant hemisphere lesions.
Herniation Syndromes
An ipsilateral hemiparesis, due to Kernohan's notch, is caused by compression of the opposite cerebral peduncle. The early 3rd nerve stage is an ipsilateral enlargement of the pupil with a sluggish light response.
Chronic Disorders of Consciousness
In the vegetative state, the reticular formation is functioning and the eyes are open. Of these terms, akinetic mutism requires a separate discussion as it differs from the vegetative state.
Brain Death
If respiratory movements are observed, the apnea test result is negative (ie it does not support the clinical diagnosis of brain death) and the test should be repeated after a suitable interval. Therefore, the initial absence of Doppler signals cannot be interpreted as consistent with brain death.
Questions (True or False)
124 5 Evaluation of the poorly responsive patient. ii) Small systolic peaks in early systole without diastolic flow or reverberant flow indicate very high vascular resistance associated with greatly increased intracranial pressure and support the diagnosis of brain death.
There are six main and partial discussions; most are simple, but they must be committed to memory as they are the core of neuroanatomical localization. These are the corticospinal tract, the corticobulbar tract, the visual pathway, the oculomotor discussion with its associated pathways, the lateral spinothalamic tract and the medial lemniscus.
The Six Major Anatomic Decussations with Clinical
Initially, the most confusing elements of neuroanatomy for many medical students are probably the decussations of the neural pathways. Obtained with permission from Blumenfeld (2002). of rapid tapping of the feet, increased reflexes and Babinski's sign.
The ventral posteromedial nucleus (VPM) of the thalamus receives crossed fibers from the main sensory nucleus of the trigeminal nerve. Due to bilateral innervation of the nucleus ambiguus, dysphagia is rarely caused by an acute unilateral cerebral lesion. e) Corticolingual fibers to the tongue arise from neurons in the lower part of the precentral gyrus.
Despite paresis of the medial rectus muscle, convergence is often preserved. f) Lesions of the abducens nucleus cause ipsilateral lateral rectus weakness and, in rarely documented cases, an ipsilateral gaze paresis. There are rare cases of upgaze paresis due to lesions of the median raphe in the pons.
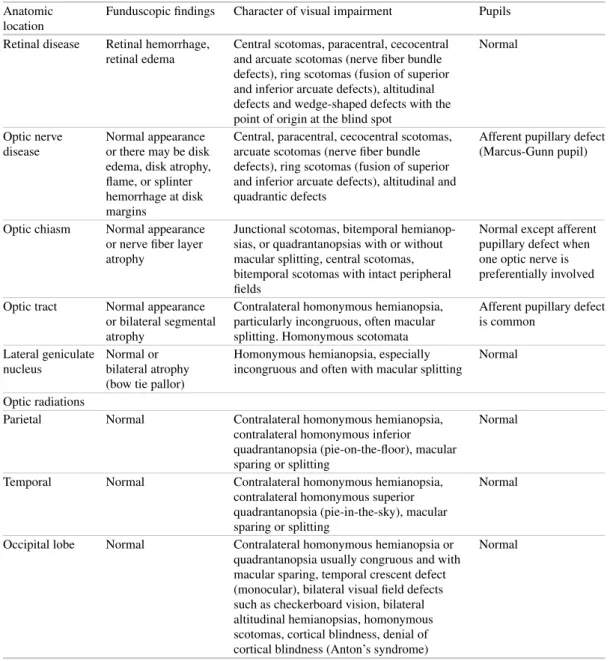
Yet they usually cause disabling symptoms. i) Medial occipital lobe lesions may cause a temporal crescentic visual field loss affecting only one eye contralateral to the lesion. Medial occipital lobe lesions can cause a temporal crescentic visual field loss affecting only one eye contralateral to the lesion. j) Bilateral occipital lobe lesions are usually due to vascular disease involving the basilar.
The Sensory Systems
Axons from these neurons decussate in the anterior commissure and ascend to the ventrolateral part of the spinal cord. Neurons of the VPL nucleus of the thalamus receive input from the lateral spinothalamic tract and the medial lemniscus.
Ischemic Stroke (Cerebral Infarction) and Transient Ischemic Attack
Cerebrovascular disease usually accounts for approximately 5-15% of a general neurologist's outpatient practice, but it is the most common condition seen in the hospital setting. Case reports will be included to illustrate the importance of the history and neurological examination to determine both the anatomic and pathological diagnosis, the indicated evaluation, and some current treatment methods.
Cerebrovascular Anatomy
The lowest portion of the internal carotid artery is the usual site of atherosclerotic plaques. The first major branch of the supraclinoid portion of the internal carotid artery is the ophthalmic artery.
Venous Sinus Disease
Horner's syndrome can occur if the sympathetic fibers pass through the sheath of the internal carotid artery. Cranial nerves 3rd, 4th, 5th-1 and 2, 6th, and sympathetic fibers pass through the sinus of the cavity.
Intracerebral Hemorrhage
During this time, two additional CAT scans of the brain show incipient resolution of the hematoma. Cerebellum (8%) Ipsilateral gaze preference with paretic gaze nystagmus, ipsilateral ataxia and truncal ataxia are uncommon, as cerebellar vermis bleeding is rare.
Subarachnoid Hemorrhage
The first branch of the internal carotid artery is the ophthalmic artery which leaves from the supraclinoid portion. Embolism associated with atherosclerotic disease at the origin of the common carotid artery is a common source of cerebral infarction.
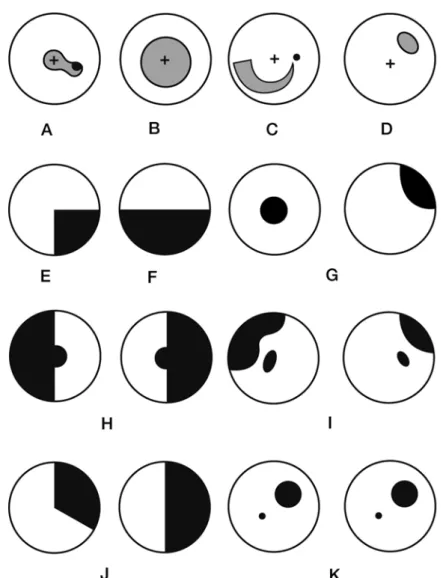
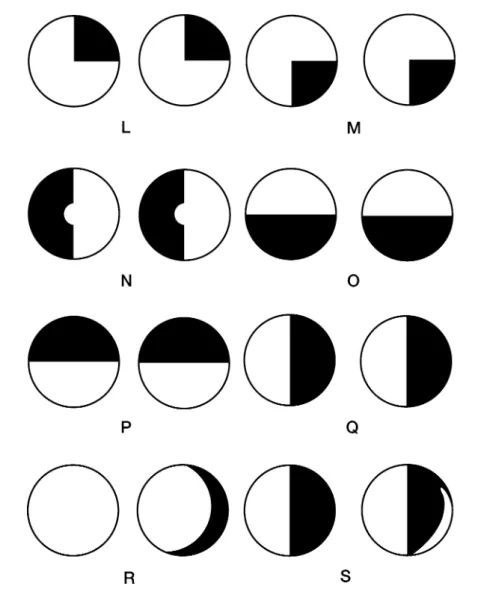
Pupil
Familiarity with the anatomy of the autonomic nervous system is critically important to the diagnosis of many neurological diseases. The most clinically useful elements of the autonomic nervous system will be reviewed in this chapter.
Autonomic Nervous System Anatomy with Clinical
This is due to the delay in pupil dilation for several seconds in the presence of a sympathetic lesion. A suspicion of light-near dissociation begins with an assessment of the pupillary response to light.
Case Reports
Left-sided Horner syndrome fits nicely with a left corticospinal tract lesion, suggesting pathology on the left side of the cervical spinal cord. The left hemiparesis is unchanged, but there is paresis of the right leg with a right Babinski sign.
Blood Pressure
The patient complains of feeling slightly dizzy, but after 2 minutes the blood pressure rises to 120/80 with a heart rate of 84 and she feels well. Blood pressure should be taken after 3 minutes if previous blood pressures are not diagnostic.
Genitourinary System
The external sphincter receives somatic innervation originating from Onuf's nucleus, S2-S4, located in the ventrolateral gray matter of the spinal cord. The external sphincter receives somatic innervation originating from Onuf's nucleus, S2-S4, located in the ventrolateral gray matter of the spinal cord.
Neuromuscular Diseases
There is an overlap with AHC, but pathology affecting these lower motor neurons will be included. The anatomical distribution of weakness usually provides the diagnostic clue and this element will be highlighted.
Neuroanatomic and Differential Diagnoses
The approach to patients with these disorders will be outlined with a strong emphasis on history and neurological examination. Case numbers of each anatomic site will be listed at the end of the chapter to facilitate review of all reports pertaining to that disease location.
Cases
Past Medical History: The patient has a 50-pack-year history of smoking, hypertension, and type II diabetes. She has had paresthesia of the toes for several years and this is attributed to her diabetic neuropathy.