Some product names, patents and registered designs referred to in this book are in fact registered trademarks or proprietary names, although they are not always specifically referred to in the text. Therefore, the appearance of a name without a proprietary designation should not be interpreted as a representation by the publisher that it is in the public domain.
Tumors
Infection
Trauma
Arthritis
Prostheses
PREFACE
The encouragement of my wife and three daughters has been essential to my completion of this project. I cannot fail to mention also two of my colleagues at the Vancouver General Hospital, Mr.
CONTRIBUTORS
Klinisk instruktør Department of Radiology University of British Columbia Vancouver, British Columbia, Canada Alison Spouge, M.D., F.R.C.P.C. Lektor Department of Radiology University of Western Ontario Department of Diagnostic Imaging University Hospital.
Clinical Presentation
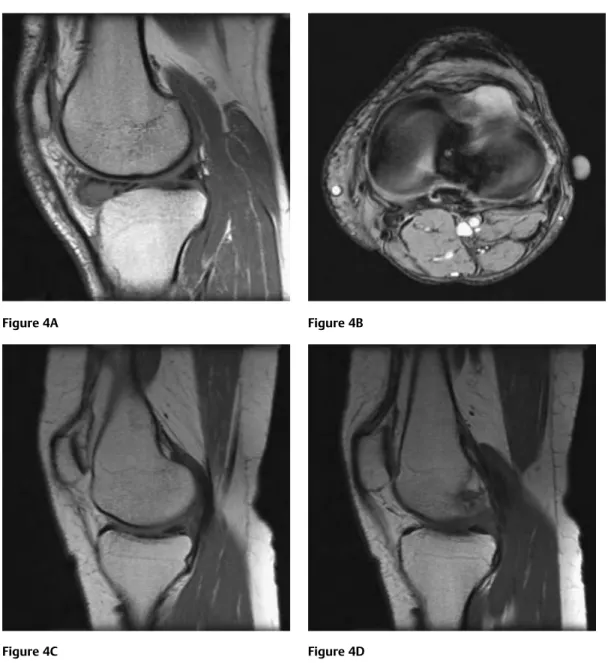
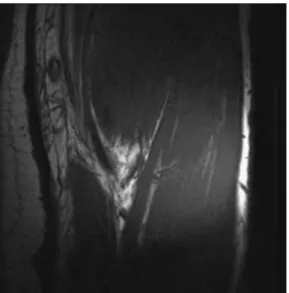
MRI (Figs. 1A-1C) revealed a focal disruption of the cranial third of the anterior cruciate ligament (ACL).
Internal Joint Derangement
Diagnosis
Discussion
Less commonly, avulsions may be observed at the semimembranosus and arcuate ligament insertions. Using MR imaging to diagnose partial tears of the anterior cruciate ligament: value of axial images.
Radiologic Findings
Differential Diagnosis
On coronal images, the PCL is seen in the medial aspect of the intercondylar level. There may be some irregular thickening associated with the surface of the ligament.
13Clinical Presentation
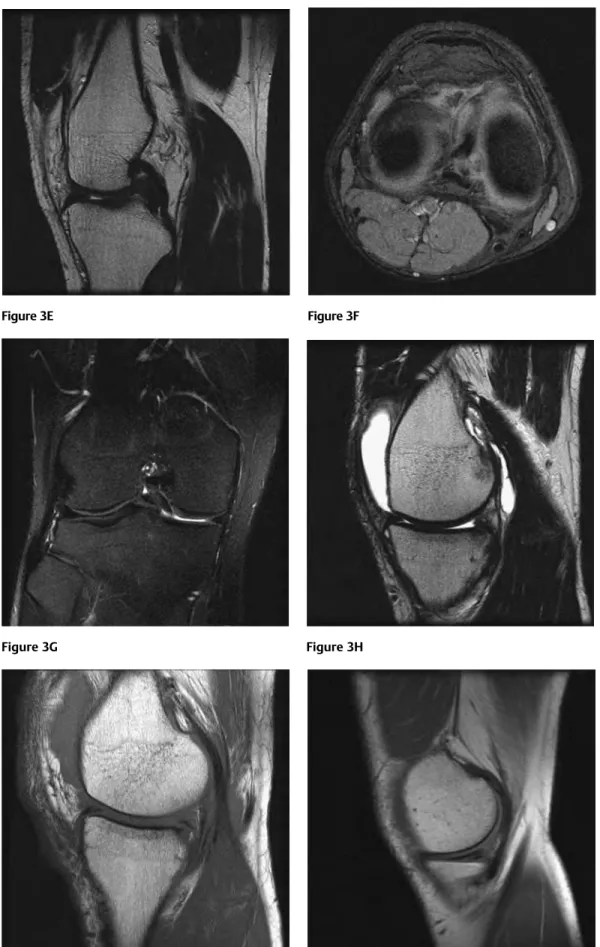
A T1-weighted sagittal image (Fig. 3A) shows a complex tear in the posterior horn of the medial meniscus. A similar lesion was noted extending from the posterior horn of the medial meniscus in the other.
25Radiologic Findings
Between the deep and superficial parts of the MCL lies a bursa surrounded by a variable amount of fat. The superficial portion of the MCL can be further divided into vertical and posterior oblique components.
31Radiologic Findings
Rice bodies are usually noncalcified, whereas 70% of synovial osteochondromatosis nodules will eventually be calcified. Post-manipulation CT of the knee joint: aid in the diagnosis of intra-articular loose bodies.

37Clinical Presentation
Rupture of the quadriceps tendon is uncommon in the absence of conditions predisposing to tendinopathy. Cramped patellar tendon: an indicator of abnormalities in the extensor mechanism of the knee.
45Radiologic Findings
Increased signal intensity on T1- and T2-weighted images at the tibial insertion site of the patellar tendon, reflecting the presence of blood products and edema. Figures 9D Recovery of axial inversion at the level of the tibial tuberosity shows a central high signal in the so-called open-shell configuration. 9E Sagittal T2-weighted image shows a combined avulsion of the patellar tendon insertion and an intratendon tear at the tendon-bone border.
An ill-defined high signal is also demonstrated in the adjacent lower pole of the patella. On proton density-weighted images, abnormal signal intensity is seen in the proximal one-third of the patellar tendon.
62Radiologic Findings
Discoid meniscus is a relatively common variant of the menisci, present in 1 in 20 pediatric knees imaged. Rarely, plain film findings may include hypoplasia of the lateral femoral condyle and a higher than normal fibular head. Widening of the lateral joint space can be seen, and there is reportedly a decrease in height of the lateral intercondylar tibial spine.
Continuity of the anterior and posterior horns of the lateral meniscus is expected laterally on two consecutive 5-mm slices (so-called bow ties). The presence of a free-floating or unattached posterior horn of a discoid meniscus on MRI should raise the suspicion that it is the cause of the patient's pain, especially in the absence of a tear.

Clinical Presentation
Grade 3 Fissuring, fragmentation and fissuring of cartilage extending to the subchondral bone but affecting less than 50% of the patellar articular surface. Grade 4 More than 50% of the patellar articular surface is exposed, with sclerosis and erosions of the subchondral bone. Grade 4 Chondromalacic changes extend to the subchondral bone and involve more than half of the patella articular surface.
12H Grade 3: Cartilage thinning extends to the subchondral bone but involves less than 50% of the articular surface of the patella. 12I Grade 4: Chondromalacic changes extend to the subchondral bone and involve more than half of the patellar articular surface.
73Radiologic Findings
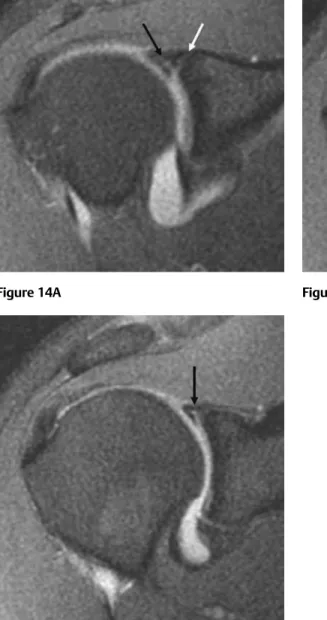
The rotator cuff consists of the supraspinatus, infraspinatus, subscapularis and teres minor tendons. Interruption of the supraspinatus tendon with a high signal equal to the fluid signal between the tendon fragments. Amount of retraction and degeneration of the torn supraspinatus tendon (if the tendon is retracted proximal to the glenoid rim, repair is unlikely to be successful.).
A type II SLAP tear represents minimally displaced stripping of the superior labrum of the bony glenoid. Extension of the curvilinear defect posterior to the biceps anchor also indicates a labral tear.
79Radiologic Findings
The long head of the biceps tendon contributes to the stability of the glenohumeral joint. A dislocated long head of the biceps tendon (Fig. 16E) may appear on axial MRI as a GLOM (arrow). The long head of the biceps tendon should be systematically assessed in all cases of suspected rotator cuff tear.
Abnormalities of the long head of the biceps tendon of the shoulder: MR imaging findings. The hyaline cartilage of the hip joint can extend below the labrum and thus "undercut".

97Clinical Presentation
The most common appearance of lateral epicondylitis is a focal hypoechoic area in the deep part of the tendon (Fig. 19F,19. On ultrasound, the most common appearance of lateral epicondylitis is a focal hypoechoic area in the deep part of the tendon. Chronic Inflammation of the adjacent radiobicipital bursa (separating the tendon from the proximal lower radius) may be visible.
Transaxial 20LA T2-weighted image shows distal tendon thickening, heterogeneous intrasubstance high signal, and fluid in the tendon sheath. Loss of definition and loss of anterior concavity of the tendon in cross section.
121Radiologic Findings
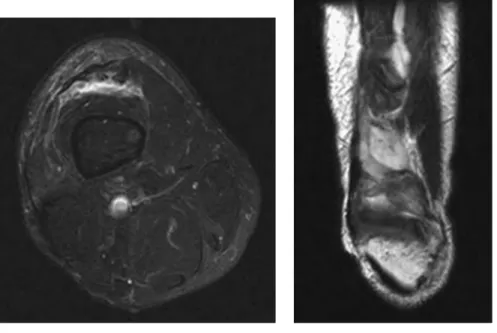
The tibialis posterior tendon runs in a groove behind the medial malleolus deep to the flexor retinaculum and anterior to the tendon of the flexor digitorum longus. Partial tears can be seen as clefts that extend into the synovial surface of the tendon. There is marked swelling and internal signal heterogeneity of the tibialis posterior tendon, which cannot be clearly defined as a distinct structure.
On MRI, the tibialis posterior tendon usually measures twice the diameter of the flexor digitorum at the level of the ankle joint. The finding of abnormal signal intensity in the sinus tarsi on MRI should alert the radiologist to potential abnormalities of the tibialis posterior tendon.
129Clinical Presentation
The remaining fibers are visible on the cephalad extent of the tendon (on the diagrammatic left side of the figure). To show the entire peroneus longus tendon, the covered region should be extended to the first metatarsal bone. The peroneus longus tendon is visible as a single hyperdensified oval structure at 9 o'clock within the common sheath.
The medial part of the peroneus brevis shows intrasubstance disturbances beyond the central split. If the full length of the peroneus longus tendon is not visualized, the tears may be missed.
137Radiologic Findings
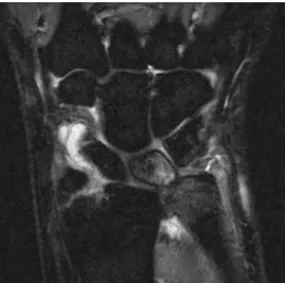
The scaphoid and lunate are palmarly flexed with a reduced SL angle (30 degrees), a normal or increased capitolunate angle (30 degrees), and palmar subluxation of the head. Indirect MR arthrography significantly improves sensitivity in evaluating the SL ligament compared with unenhanced MRI of the wrist. A bony fragment is projected distal to the distal radius in the expected position of the radial styloid.
Focal tenderness on the medial aspect of the wrist, especially distal to the ulnar styloid. For example, avascular necrosis is more likely to affect the radial side of the lunate than the ulna.
147Radiologic Findings
Congenital and Pediatric Conditions
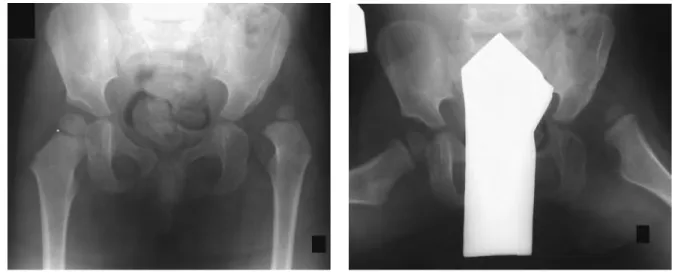
Later still, increased uptake in both the femoral head and acetabulum may be demonstrated if the disorder is complicated by secondary degenerative disease. 26C and 26D Lateral anteroposterior images of the frog's leg show flattening and fragmentation of the femoral head with associated cystic changes in the subjacent femoral metaphysis (the latter associated with a poor prognosis). Prognosis depends on the amount of femoral head involved; if more than 20% of the head is extruded laterally, the prognosis is poor.
On MRI, the coronal and sagittal planes are most useful in assessing joint congruity and coverage of the femoral head (with prognostic significance). Thus, the femoral head is predisposed to drop out of the acetabulum, putting the hip at risk for subluxation/dislocation when exposed to mechanical stress, for example, breech delivery.
156Radiologic Findings
This results in the shortening of the long bones and a decrease in the diameter of the vertebral body and posterior arch. A lateral skull may show midfacial hypoplasia, enlarged calvaria, frontal prominence, and shortening of the skull base. Lateral view of the lumbar spine shows shortening of the pedicles and vertebral bodies with prominent posterior scalloping.
The pelvis will be wide and short, with square-shaped ilia and a narrow pelvic opening. The lateral view of the lumbar spine shows shortening of the pedicles and vertebral bodies with pronounced posterior serration.
160Radiologic Findings
Depending on the subtype, deformities from previous fractures may be dominant at presentation, or the bones may be bent secondary to microfractures. The first fracture typically occurs in the second or third year of life, although presentation can be as early as birth (intrapartum fractures in 20%) or as late as 6 years of age. On prenatal ultrasound, bending of the long bones can be seen; however, no intrauterine growth retardation is demonstrated.
It can be enlarged due to transfer of the skull due to lack of ossification with improved visualization of intracranial contents. Although osteogenesis imperfecta may be involved, nonaccidental injuries should be considered in all cases of pediatric rib fracture, especially first rib fracture.
167Radiologic Findings
In addition, the marrow cavity becomes extremely narrowed, leading to deficient bone marrow and secondary bone marrow failure. The most severe form is seen in infants and significantly reduces life expectancy, usually due to bone marrow failure and infection. In older children, the typical triad of fractures, visual impairment and bone marrow failure is common.
Neural foraminal narrowing may be evident, for example, of the optic foramina or internal acoustic meatus. In the infantile form, there is a high mortality rate in the first 2 years of life (those with severe disease dying before the age of 3 months), secondary to bone marrow failure and overwhelming infection.
171Radiologic Findings
Lesions cluster at the end of the tubular bones, concentrated near the articular surfaces, around the acetabula, glenoid, and on the carpus and tarsus of the hands and feet. Although the condition may be recognized in infancy, the onset is usually insidious, with deformity of the extremities, pain, stiffness of the limbs, and limitation of movement in the joints first manifesting in late childhood or early adolescence, which then progresses as the patient reaches skeletal maturity. . It can affect the entire cortex or it can be limited to one side of the cortex; it may also extend into the cancellous bone (Fig. 32C).
In individual cases, MRI is invaluable in evaluating soft tissue abnormalities, such as thickening of the iliotibial band and fibrosis in the subcutaneous tissue (low signal), which may need to be treated as part of reconstructive bone surgery. and joints. Early reports of the use of bisphosphonates (eg, pamidronate infusion) show promise in treating pain and swelling of the affected limb.

179Radiologic Findings