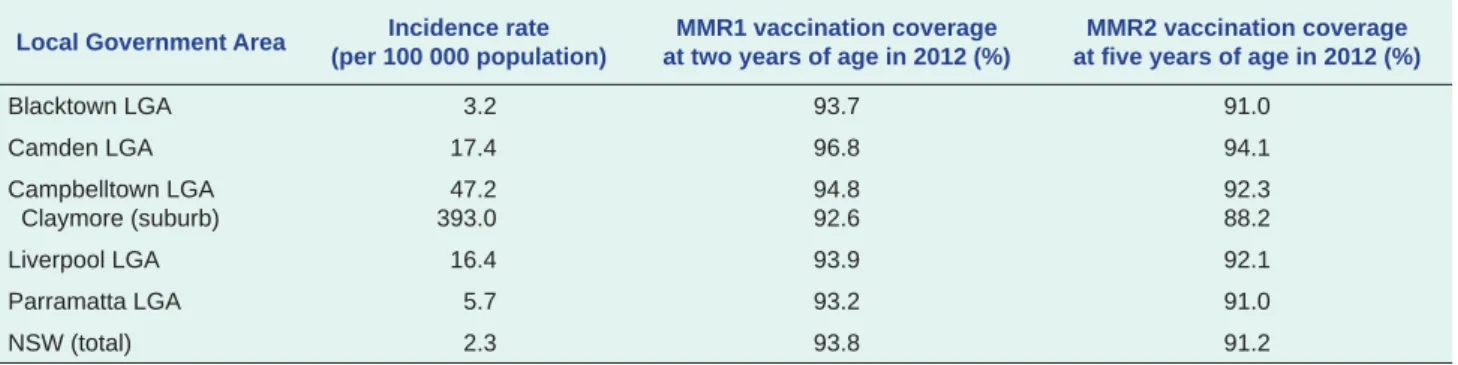
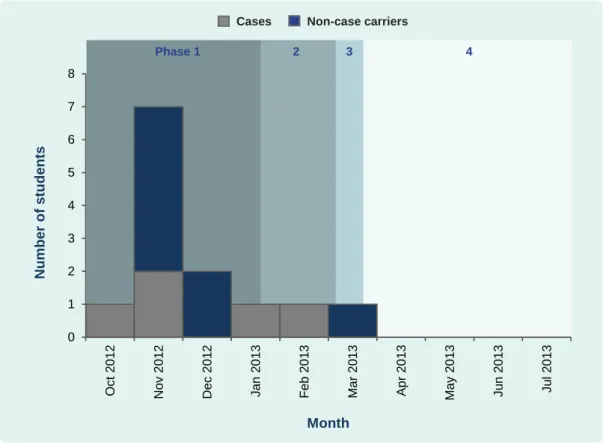
After intensified control measures, the number of students who screened positive for CA-MRSA dropped from nine to one with no more cases identified at the school. Conclusion: Identification of carriers, decolonization therapy, surveillance of cases and contacts, and strengthening of environmental and personal hygiene were control measures that helped contain this CA-MRSA outbreak in a boarding school in Hong Kong (China). Summary of CA-MRSA outbreaks in School X after screening phase, Hong Kong (China), November 2012 to July 2013.
In summary, the number of carriers for CA-MRSA decreased from nine to one (Table 1) during the screening phases; as of March 25, 2013, no further cases of CA-MRSA infection were identified (Figure 1). Identified deficiencies and recommended control measures at School X related to the CA-MRSA outbreak, Hong Kong (China), November 2012 to July 2013. CA-MRSA cases and non-carriers at School X by stage of outbreak and month of onset (for cases) or first identification (for non-case carriers), Hong Kong (China), October 2012 to July 2013.
CA-MRSA isolates in Hong Kong (China) were mainly of spa-type t019 and t437,6 other than the spa-type t441 identified in this outbreak. We reported a CA-MRSA outbreak affecting five students in a boarding school in Hong Kong (China). We reported a CA-MRSA outbreak affecting five students in a boarding school in which two (40%) were hospitalized and three (60%) required surgical treatment; this was the largest institutional CA-MRSA outbreak recorded in Hong Kong (China).
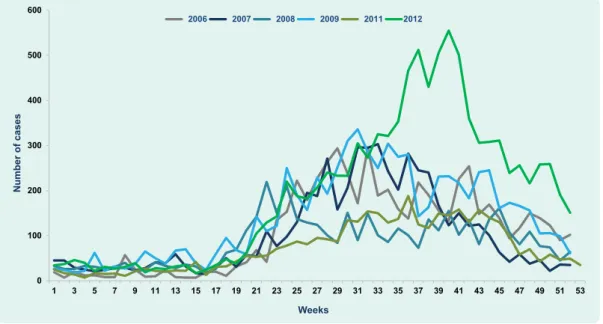
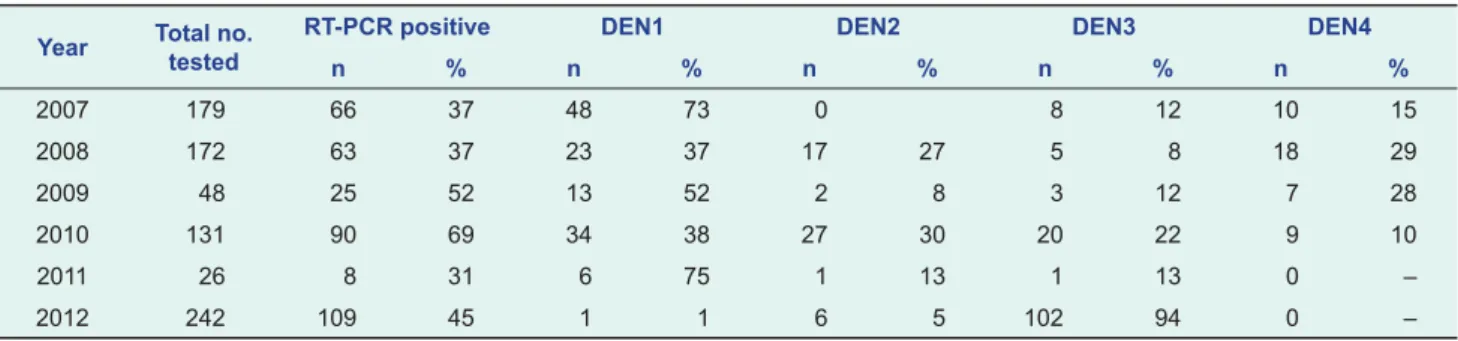
Although dengue has been a public health problem for several decades in the Lao Democratic Republic, the magnitude of the disease burden and epidemiological trends are still poorly understood.
DISCUSSION
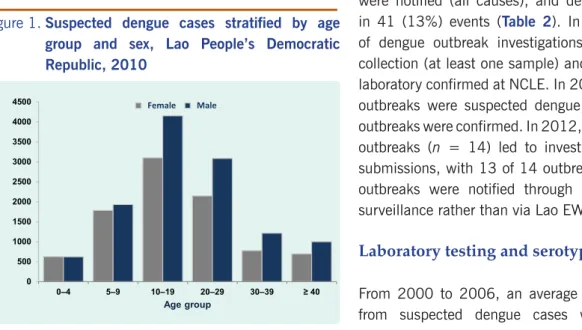
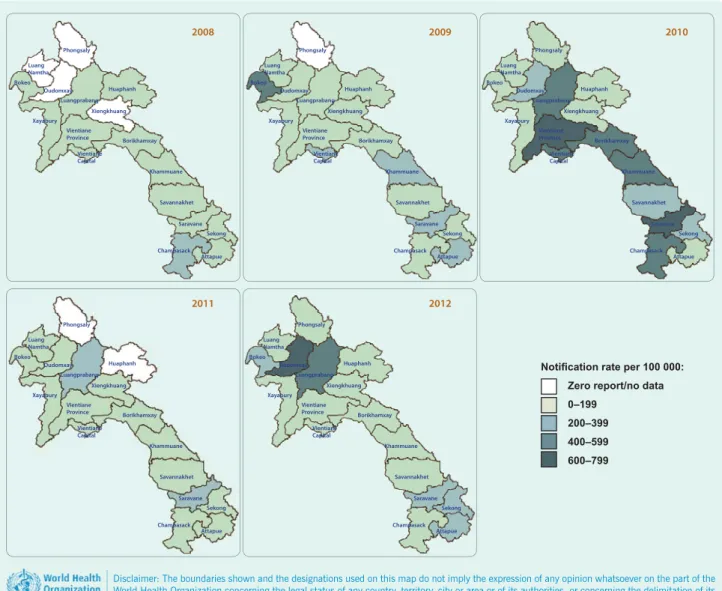
Additionally, internal evaluations of the surveillance system have found inconsistent use of clinical case definitions and weekly variability in the number of sites reported each week; there is still no system to link laboratory test results with case reporting, nor systematic reporting of RDT results during outbreak investigations. The dengue surveillance system in the Lao People's Democratic Republic has made remarkable progress and currently meets many of the key international recommendations for outbreak surveillance and response. Although our finding of an excess of suspected male dengue cases in 2010 is consistent with a recent estimate of the gender distribution in a province in the Lao People's Democratic Republic,9 we found no significant difference in laboratory-confirmed cases .
As seen in most dengue-endemic countries, disease transmission is highly seasonal in Laos and coincides with the wet season. To date, the national case data do not indicate a clear pattern of epidemic cycles as found elsewhere in the Region.11,12. Reporting of dengue cases in the Lao Democratic Republic has certainly been influenced by national awareness and community education campaigns, changing health-seeking behavior and improved access to telecommunications.
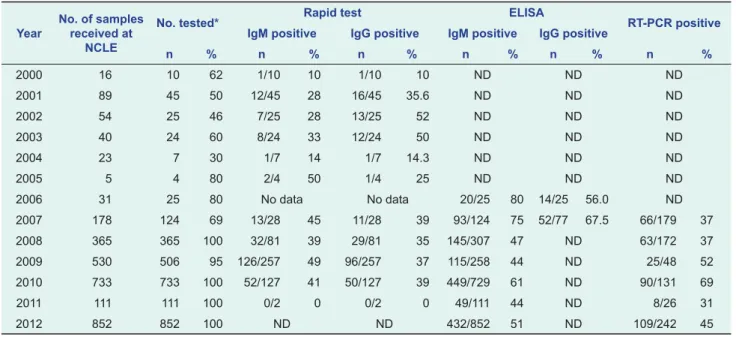
Rapid detection and typing of dengue viruses from clinical samples using reverse transcriptase polymerase chain reaction. Development and validation of real-time one-step reverse transcription PCR for the detection and typing of dengue viruses. The forthcoming analyzes will assist in the critical task of designing and implementing effective preparedness and intervention strategies, including contingency plans and risk assessment schemes, and will guide policymakers in making decisions about vaccine introductions when available.
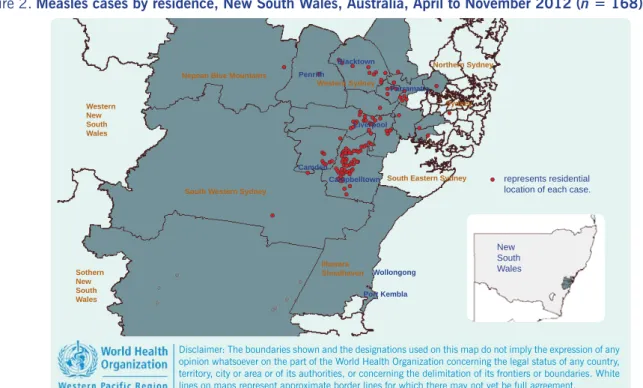
Spatial distribution and risk factors for dengue and Japanese encephalitis virus infection in urban settings: the case of Vientiane, Lao PDR. An outbreak of measles subsequently occurred in the state of New South Wales, prompting a sustained and coordinated response by public health authorities. Measles eradication has been debated since the development of an effective measles vaccine in the 1960s.
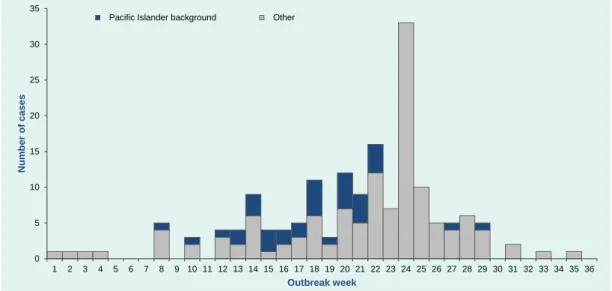
In 2005, the World Health Organization's Regional Committee for the Western Pacific, of which Australia is a member, formally declared a goal to eliminate measles in the region by 2012.5 It was suggested that this had already been achieved in Australia in 1999,4 due to high population immunity achieved by the 1998 measles control campaign and continued high two-dose vaccination rates among children since then,4,6 as well as a low incidence rate of measles in Australia with no endemic genotypes of the virus found in Australia since then. the early 1990s.4,7. During the next eight months, a further 167 cases were identified in the Australian state of New South Wales (NSW). Crude notification rates for Aboriginal and/or Torres Strait Islander people and people of Samoan descent were calculated using NSW population data obtained in the 2011 national census.
RESULTS
In particular, Pacific Islander cases were overrepresented in the first half of the outbreak, with all but two before week 23 (Figure 1). This suggests that these tick species may play a role in the transmission of both Anaplasma phagocytophilum and Anaplasma platys from ticks to humans in nature. The fight against tuberculosis (TB) in the Western Pacific region of the World Health Organization (WHO) has made significant progress over the past decade, with a 33% reduction in prevalent TB cases since 2000.
The case notification rate increased in the early 2000s, appears to have stabilized in recent years, and is decreasing for all forms and new positive staining cases. HIV testing in tuberculosis patients has gradually increased along with a slow decline in the number of HIV positive patients found. Tuberculosis epidemiology and control in the Western Pacific Region: analysis of 2012 case notification data.
Significant progress has been made in tuberculosis (TB) control in the Western Pacific Region of the World Health Organization (WHO) especially in the last decade. Each year, the region's 36 countries and territories are required to report TB surveillance data to WHO using a standardized data collection form. Case definitions for TB can be found in the 4th edition of TB treatment guidelines.4 In 2013, 30 countries and areas of the Western Pacific Region reported data representing more than 99.9% of total population.
The other three countries – the Laos People's Democratic Republic, Mongolia and Papua New Guinea – are considered priority countries with a high TB burden in the Western Pacific). Percentage of reported TB cases (all forms and new smears positive) per 100,000 population in the Western Pacific, 2000–2012. Map showing the number of reported TB cases (new and recurrent) per 100,000 population in Western Pacific countries and territories, 2012.
Treatment outcome trend expressed as a percentage of new lung smear-positive cases in the Western Pacific, 2000–2011. Progress in TB/HIV activity in seven Western Pacific countries with a high TB burden, 2005-2012. The overall percentage of TB patients tested for HIV in the Region remains low.
However, the figure has increased significantly over the past few years, particularly in Cambodia, Vietnam and the Lao People's Democratic Republic. This report provides an overview of the epidemiological and programmatic situation of TB in the Western Pacific Region, based on case notification data in 2012. TB case notification rate, estimated incidence, prevalence and mortality per 100 000 population in the Western Pacific Region, 1990–2012.
Caution should be used when referencing websites; this should only be done when its content has been substantially described in the article.