For this study, a non-probability convenience sample of 50 intensive care nurses and 50 family members from adult intensive care units (ICUs) in two tertiary care hospitals was used. Recommendations for future practice included incorporating education programs for critical care nurses regarding family needs in intensive care units and providing specific continuing education to improve communication skills.
INTRODUCTION AND BACKGROUND
The question of family needs in intensive care units as a research topic has therefore been investigated for. Furthermore, findings from these previous studies (Norris, 1986; Quinn, 1996; . Kleinpell, 1992) have revealed that nurses and families have different perspectives regarding family needs in an intensive care unit.
THE RESEARCH PROBLEM
Kleinpell, 1992) have revealed that nurses and families have different perspectives regarding family needs in an intensive care unit. It is important to understand perceptions of families' needs from nurses' perspectives as well. Otherwise, it can be very difficult to get a complete picture of the family's needs and to improve nursing care if only one side of the problem is considered.
PURPOSE OF THE STUDy
OBJECTIVES OF THE STUDY
SIGNIFICANCE OF THE STUDY
OPERATIONAL DEFINITION OF TERMS
In modern societies, the main family form is the nuclear family, although various extended family relationships are also often found (Giddens, 2006). This study was conducted in South Africa where the culture and most families adopt the extended family format.
CONCLUSiON
Before going to the ICU for the first time, the environment must be explained. Part Comparison of differences in perceived family needs as reported by family and groups of nurses.
FAMILY MEMBERS' NEEDS AND EXPERIENCES
- Feelings and experiences of family members towards
- Family members' needs from family members' perspectives
- Nurses' attitudes towards family needs
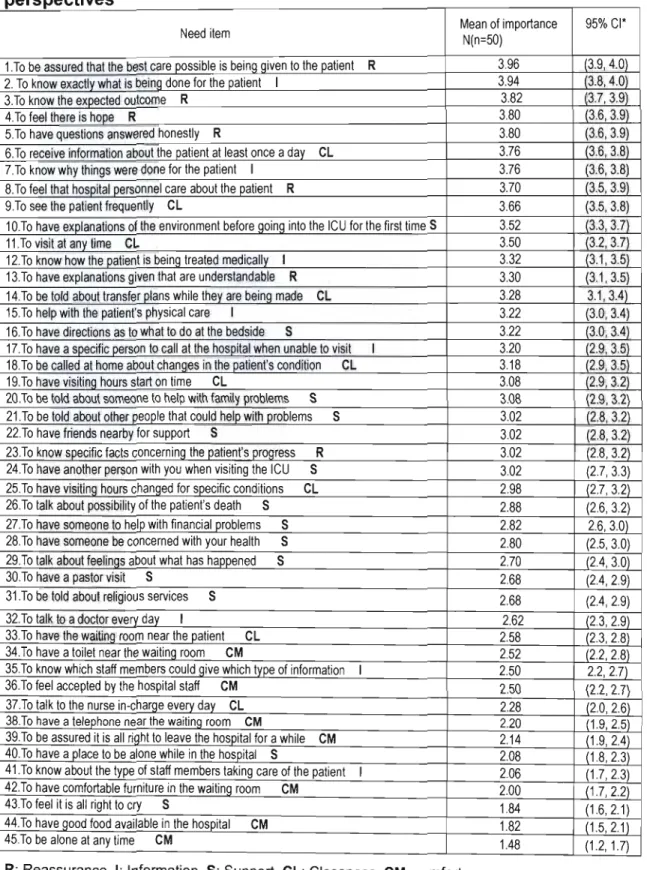
The five greatest needs from the perspective of family members were (1) to know the expected outcome (2) to have questions answered honestly (3) to be called home about changes in the patient's condition (4) to be sure that the best treatment possible is to be given to the patient, and (5) to know that the patient is being treated medically. Kirchhoff (1993) and Simon (1997) suggested that some nurses tend to limit family visits despite their understanding of the importance of visits for both the patient and family members.
FAMILY MEMBERS' NEEDS FROM NURSES' PERCEPTIONS
Even some nurses in this study who have a post-basic qualification did not reflect an accurate knowledge of the importance of relatives' needs. Maxwell (2007) also reported that nurses and family were in agreement with 5 of the 12 most important family needs.
REASONS CAUSING FAMILY NEEDS TO BE UNMET
Kosco and Warren (2000) reported that nurses agreed with families on only four of ten identified family needs. The most common differences in the perception of family needs between families and nurses concern visitation, involvement, role of the family and the role of the nurse in leu (Jacono, 1990; Williams, 2005; Fox, 2005).
STRATEGIES TO MEET FAMILY NEEDS
- Family needs at different stages during the crisis
- Information providing
- Emotional support
- Involvement of the family member
It is crucial and essential for a nurse to understand the importance of the involvement of the family members in patient care, which will contribute to the patient's recovery and outcome, and also that this is one of the strategies to meet the family members' own needs. On the other hand, the involvement of family members in a patient's care is a way to meet the needs of the families.
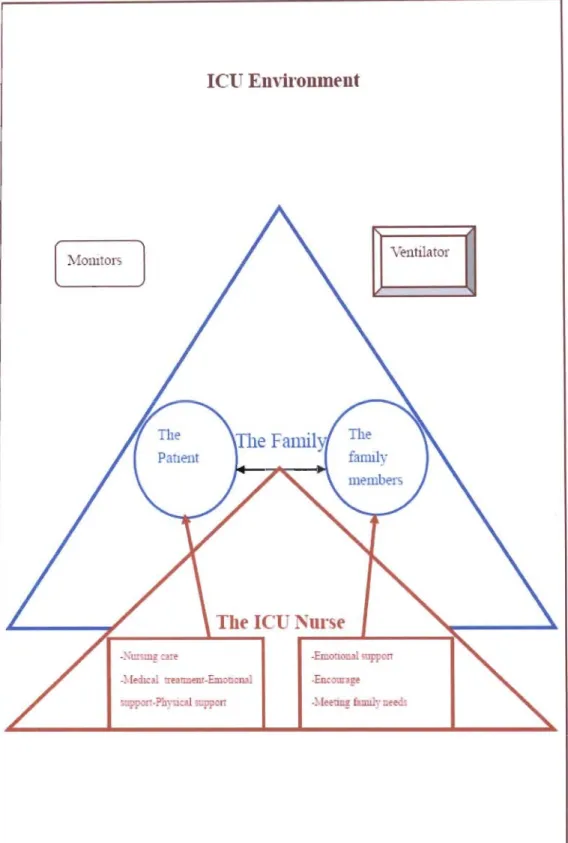
THEORETICAL FRAMEWORK
For example, if the patient is the only income earner for the entire family, it means that after he/she is admitted to the ICU, there will be no one to support the family financially and, therefore, the homeostasis of the family is broken. By supporting both family members and patients in the leu environment, the nurse would restore homeostasis between family members and the patient.
CONCLUSiON
INTRODUCTION
RESEARCH DESiGN
- Quantitative research
- Descriptive research
Family members were asked to select a family member to whom the researcher could give the questionnaire to complete. Part Data in the family group were analyzed by calculating the mean from each item out of the required 45 items. The mean scores of the 45 needs items from the two groups were also compared with a one-sample t-test, and comparing significance values.
The family group identified that of the 45 need items were rated as important or very important (mean > 3) and items were rated as somewhat important or not important (mean < 3) from the families' perspectives. Nurses were accurate in perceiving 21 (47%) of the 45 family need items compared to family members' perceived needs.

THE SETTING
POPULATION
SAMPLE AND SAMPLING PROCEDURES
In this study, the target population consists of all registered nurses working in the ICU and family members of ICU patients during the period October–November 2008 in eThekwini District Durban, South Africa. Convenience sampling, also called random sampling, is a selection of the most available people as participants in a study (Polit & Beck, 2003). For this study, the convenience sampling method was chosen, because it is convenient for the researcher to collect data, as well as because of the limited time.
SELECTION CRITERIA FOR PARTiCiPANTS
- ICU nurses
- ICU patient family members
DATA COLLECTION INSTRUMENTS
- Measures for ensuring reliability and validity
- Pilot Study
When considering the reliability of the instrument, the researcher chose to use the test-retest reliability technique. The researcher also gave the same questionnaire to three senior ICU nurse specialists and to the research supervisor to assess for content and face validity of the instrument. Consequently, the researcher believes that the validity and reliability of the CCFNI is sufficient, and that it was suitable for the researcher to use in the local hospitals to conduct this research.
DATA COLLECTION PROCESS
To protect the confidentiality of the participants, a box was provided where the participants could drop in completed questionnaires. The researcher kept a distance from the participants while they completed the questionnaire so that they could complete the questionnaire independently.
DATA MANAGEMENT
DATAANALySIS
First, the mean scores for the 45 need items obtained from the two groups in Parts 1 and 2 were compared using a one-sample t-test, which was used to compare the mean of each item between the family and nurse groups, to obtain the significance values ( p-value) for each of the 45 need items. The researcher was then able to compare the significance values obtained from the one sample t-test for each need item between the two groups and find the possible differences in perceived family needs from the perspective of nurses and families. If the p-value was greater than or equal to 0.05, it meant that there was no significant difference between the family and nurse groups in relation to this need item.
ETHICAL CONSiDERATIONS
- Permission of the study
- Informed consent
- Potential risks and benefits
- Confidentiality
- Anonymity
- Withdrawal
- Self-determination
The significance level was set at 0.05, and the researcher considered only items whose p-value was less than 0.05 as significantly different. Permission was further sought from the KwaZulu-Natal Department of Health (Appendix 10) and from the relevant target hospitals (Appendixes 11 and 12) to carry out the study. Refusal of participation by the family will not affect any patient's care and treatment in the ICU.
CONCLUSION
Participants had the right to voluntarily decide whether they wanted to participate in the study, without risking any punishment or adverse treatment. It also meant that people had the right to ask questions, to refuse to give information, to ask for clarification or to end their participation (Polit & Beck 2003: 147).
INTRODUCTION
SECTION A: PARTICIPANTS' DEMOGRAPHIC INFORMATION
- The demographics for the families
- Gender of family member participants
- Cultural groups of family member participants
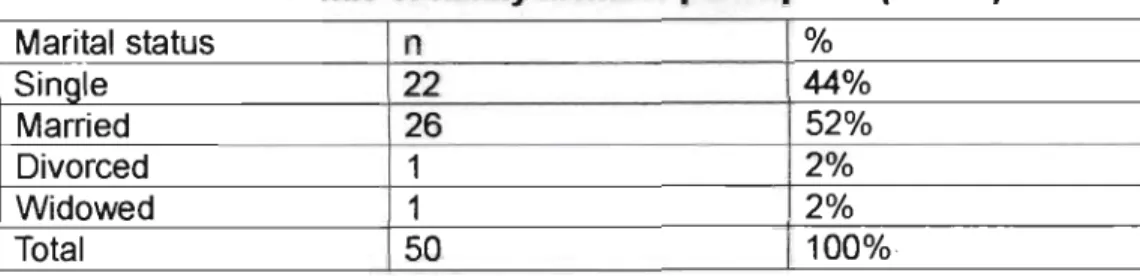
- Marital status of family member participants
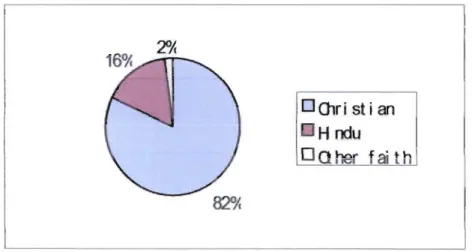
- Religion of family member participants
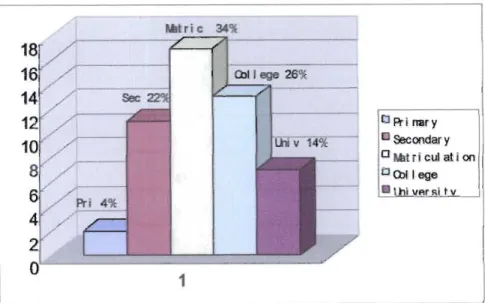
- Education of family member participants
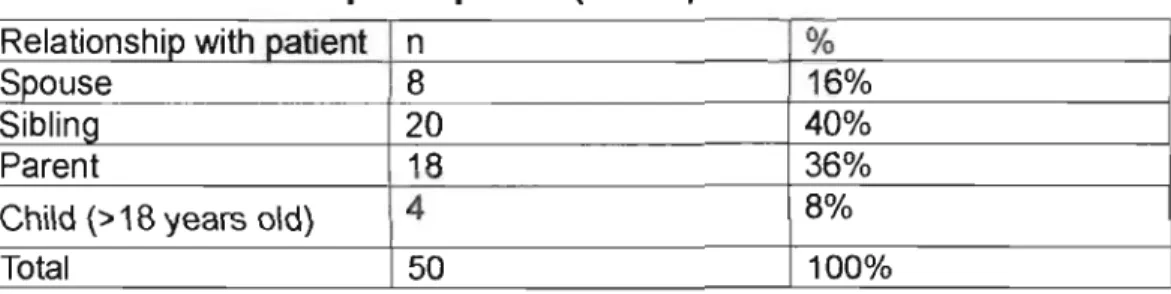
- Relationship with patient
- Previous ICU visiting experiences
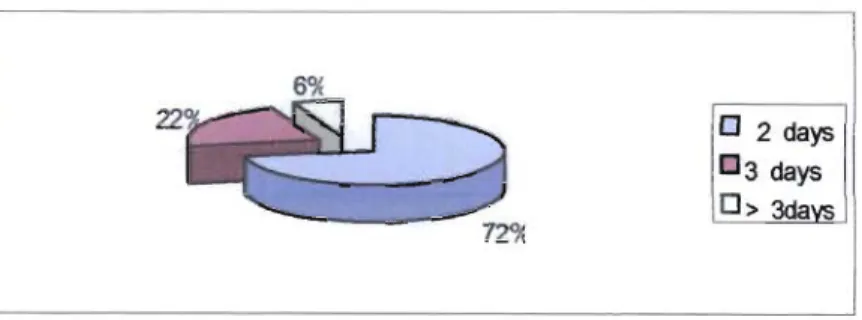
- Days the patient has been in ICU
- The demographics for the nurses
- Gender of nurse participants
- Age of nurse participants
- Cultural groups of nurse participants
- Marital status of nurse participants
- Religion of nurse participants
- Nursing educational level
- Work title of nurse participants
- Type of ICU training of nurse participants
- ICU training experience of nurse participants
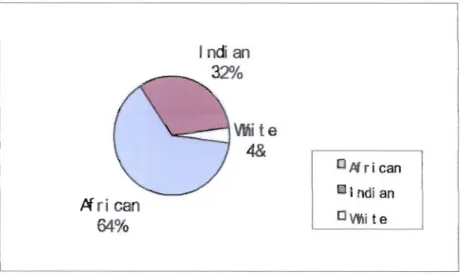
According to figure 4.2, three cultural groups were observed among the entire family members in this study. Forty percent of the participants (n=20) went to the ICU to visit their siblings, 36%. The majority of the participants, 88% (n=44) had a diploma in Nursing while 12% (n=6) had a degree in Nursing.
SECTION B: DESCRIBES AND COMPARES THE DATA REGARDING
- Family needs from family members' perspectives
- Family needs from nurses' perspectives
Seventy percent (n=35) of participants chose the need 'to have questions answered honestly' as their most important need (mean=3.70). 9. See the patient regularly. 9. Tell about someone who can help with family problems. 10. Get explanations about the environment. The remaining of the three need categories, namely the need for 'proximity', 'information' and 'support', were ranked differently by the two groups.
CONCLUSiON
This chapter presents the summary and discussion of the study findings. These figures showed that nurses were less accurate on half of their family's perceived needs compared to family members' perceptions, despite both groups agreeing on 5 of the top 10 most important needs. A description of healthcare providers' perceptions of the needs of significant others in intensive care units in Norway and Sweden.
FINDINGS
- Participants' demographic information
- Family members' needs from families' perspectives
- Family members' needs from nurses' point of view
- Comparison of the differences in perceived family
The need for reassurance (mean = 3.63), such as assurance of the best possible care for the patient, knowing what and why things have been done for the patient, knowing what the expected outcome is, feeling hopeful, etc., is considered assessed as the first priority. by family members. Findings from relative studies (Leske, 1986; Hupcey, 1998; AI-Hassan & Hweidi, 2004; Fox-Wasylyshyn, 2006) show little difference compared to this study in terms of the need for comfort, which is always considered an important need was assessed. category by the nurses. In addition to visits, families were desperately concerned about their loved ones in the ICU, but nurses tended to focus on families' needs for support, such as family members' health, and someone who could help with family issues.
RECOMMENDATIONS
Journal of Intensive and Critical Care Nursing Perceived needs of Jordanian families of critically ill hospitalized patients. Experiences of partners of seriously ill persons in an intensive care unit. 1990) Critical care family needs: confederate nurse-family member pairs. An analysis of information available to relatives in intensive care. 2005) Relatives' experiences of critical care.
1986) Investigation of selected psychosocial needs of family members of critically ill adult patients. 1991) Critical care nurse's perceptions of family needs. 1998). A qualitative study to determine the self-perceived needs of family members of patients in a general intensive care unit. 2005).
L1MITATIOONS OF THE STUDy
CONCLUSiON
2000) Needs of families with a relative in an intensive care unit in Hong Kong. 2003) Immediate needs of adult relatives of adult intensive care patients in Hong Kong. 1986) Needs of relatives of seriously ill patients: a follow-up. Critical care and critical care nursing a) The needs of family members visiting adult intensive care units, as perceived by family members and nurses. 1996b) The needs of relatives visiting adult intensive care units, as perceived by relatives and nurses.
Stricker, K.H.; Niemann, S; Bugnon, S; Würz, J; Rohrer, 0 and Rothen, HU (2007) Family satisfaction in intensive care: cross-cultural adaptation of a questionnaire, Journal of Critical Care 22 p204-211. You are invited to participate in a study on the needs of relatives in the intensive care unit (ICU).