I hereby certify that I have prepared this dissertation report entitled “Providing health services to refugee children from the Democratic Republic of the Congo living in Durban, South Africa: A caregiver's perspective” This dissertation is my own work and all primary and secondary sources have been acknowledged . To the classmates of Health Promotion, thank you for all the help and motivation in group work, good luck to everyone.
CONCLUSION AND RECOMMENDATIONS
Rationale of the study/Problem statement
It is therefore critical for refugee children to access the host country's local primary health care services (Beirens et al., 2007). Advice is often sought from friends, family and the community pharmacy before seeking help from healthcare services.
Aim and Objectives
Research Questions
Are caregivers satisfied with the health care services provided to their children by public clinics and private doctors in Durban, KwaZulu-Natal. What are caregivers' experiences of health care service provision for their children in Durban, KwaZulu-Natal.
Outline of the dissertation
- The vulnerability of refugee children
- Child immunisation as health promotion action
- Other health conditions
The fifth chapter presents the discussion of the findings, aligned with the research objectives. According to UNICEF (2010), infant mortality refers to “the probability of dying between birth and the age of five years, expressed per 1,000 live births, and the infant mortality rate as the probability of dying before the age of one year, expressed per 1,000 live births” .
Health care service utilisation
In the case of refugees, it can be argued that accessibility includes the use of interpreters to assist in the health care facilities that deal with refugees who do not speak English (WHO, 2012). Quality issues also refer to the requirement that healthcare workers be skilled and apply best practices in the management and treatment of clients and patients.
Barriers to Access health services by refugees
- Human and legal rights of refugees
- Socio-economic status of refugees
- Language Barriers
- Influence of cultural health beliefs in health care services
- Knowledge of the South African health care system
- Health worker attitudes towards refugees or migrants
- Medical Xenophobia
The importance of effective interpersonal communication in the healthcare delivery process is well established. A similar finding was reported by Apalata et al. 2007) in their study of refugee perceptions of the quality of health care in Durban.
Parents and caregivers perceptions of child health care services
A study conducted in Canada highlighted a collaborative and trusting partnership between parents and health professionals, further characterized by mutual respect, open information sharing and shared decision-making taking into account specific family circumstances and needs (LeBlanc, Naugler, Morrison, Parker & Chambers, 2014 ). In conclusion, perceptions of the quality of care received by health services are important for improving the quality of health services, as they provide better insight into their practice and a particular problem, which allows for improvements in patient care. From the point of view of human rights, quality healthcare can be considered the right of all patients and the responsibility of healthcare professionals.
Social networks and access to healthcare
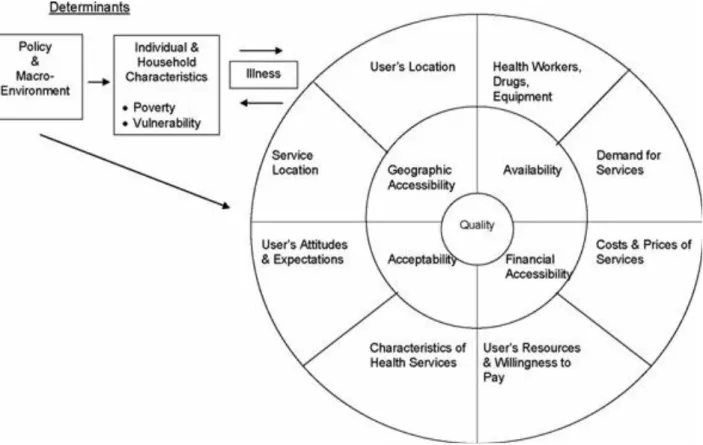
The components associated with healthcare quality as explained by the conceptual framework of Peters et al. Geographic accessibility refers to the distance from home to the healthcare facility or the travel time to the healthcare facility. Availability refers to the right type of care available to everyone who needs healthcare, including (refugees, migrants, vulnerable groups such as children and women).
Research Setting
- Quantitative survey
- Qualitative study
The aim of the study was to investigate the perceptions of refugee parents/or guardians regarding the provision of health services for their young children. These methods were chosen because they gave the researcher an opportunity to understand different aspects of the quantitative data in more detail (Creswell & Plano-Clark, 2011). The added value of the qualitative component was to gain a deeper understanding of caregivers' perceptions and experiences.
Sampling and Participants
Participants were included in the study if they met the inclusion criteria: being a DRC refugee living in Durban, aged 18 years or older, having a child or caring for other children, and being willing to participate in the study. Based on the inclusion criteria, 120 parents/or caregivers of young children (up to ten years old) were recruited for the quantitative phase of the study. Ten of the participants in the quantitative study were randomly selected for the qualitative study to provide more information about the different aspects explored in the quantitative study.
Research instruments
Some of the questions asked were: Have you received any help from your refugee community? Items were adapted from the National Survey of Early Childhood Health (NSECH) used in the study by Halfon & Hochstein, 2004) regarding satisfaction with health care for young children. The questions assessed parents' overall satisfaction with health care services, but also the health service consultation process.
Data Collection Procedures
For the qualitative research, an interview schedule was developed in English and translated into French, based on the main research areas of the quantitative research instrument. Some of the questions asked were: What diseases do your children suffer from that you sought medical treatment for? How did the healthcare providers make you feel when you visited the clinics? Informed consent was sought by explaining the objectives of the study, the voluntary nature of participation in the study, the confidentiality and anonymity of the information provided, and the right to withdraw from participation at any time during the interview the examination without the doctor's permission. any negative consequences.
Data Analysis
- Quantitative data analysis
- Qualitative data analysis
Quality control of the data was performed to ensure that it was correctly coded and imported into SPSS. The final step in the process involved interpreting the data and cross-checking it with the data (Terre Blanche et al., 2006). Particular attention was also paid to supporting the validity and reliability of the quantitative and qualitative studies.
Socio-demographic characteristics of the participants
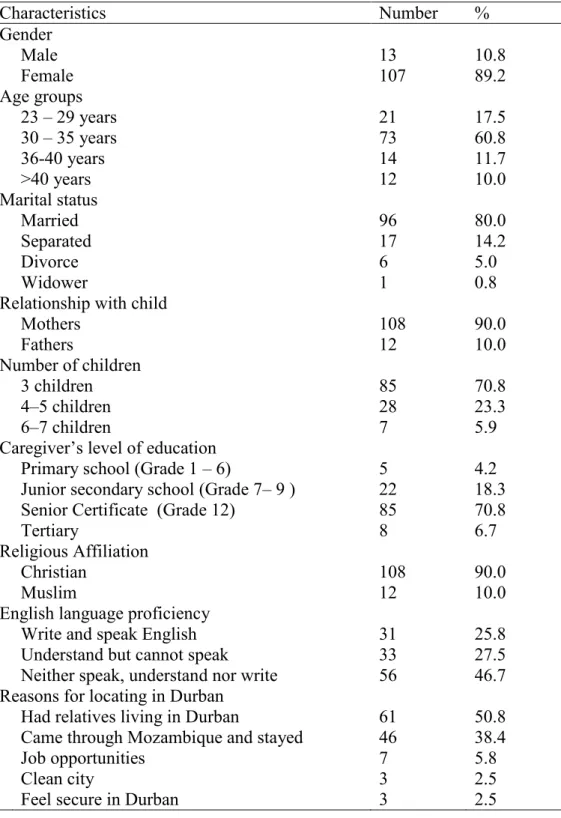
Nearly all (98.2%) participants who could not speak, understand, or write English were women. Regarding their documentation, the majority of participants (86.7%) were asylum seekers (i.e. not classified as refugees by the UNHCR), while 13.3% were officially refugees. About half of the refugee caregivers decided to settle in Durban because they already had relatives living in Durban.
Socio-economic and social-support of participants
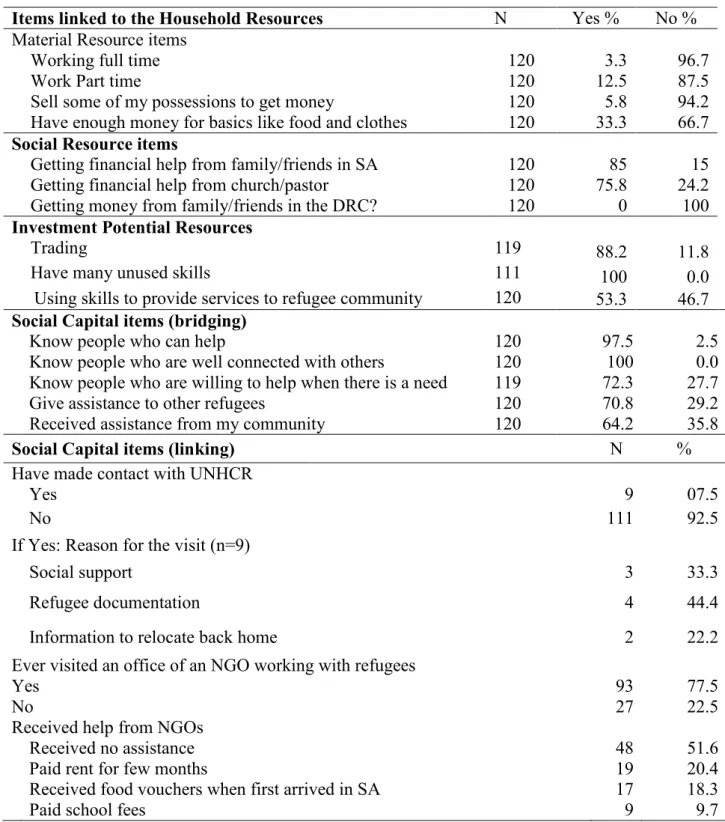
- Household resources
- Social networks
When participants were asked about their source of income, the majority of respondents (96.7%) said they were not employed full-time. The results in Table 2 also revealed that most respondents also rely on social networks for help. Regarding social networks outside the refugee community, very few participants (7.5%, N=9) indicated that they had visited the United Nations High Commissioner for Refugees (UNHCR) for support.
Child Health Status and Immunization
Regarding the social services for refugees, I can say that it does not help, because they [the provision of services] are based on discrimination, just like the nurses do in the clinics. However, it should be noted that the majority of children (82%) in the study were under the age of 12 and are likely to develop this later. The results further showed that the majority of children (70%) had been vaccinated in the Democratic Republic of Congo, while the remaining 30% had been vaccinated in South Africa.
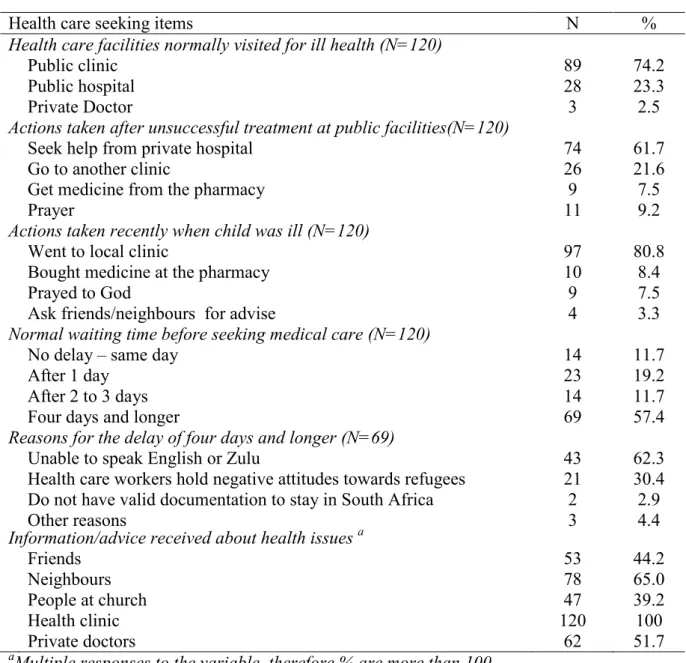
Health care seeking for children
Name of child vaccinated and age when vaccinated N% BCG/TOPV at birth (Bacillus Calmette Guerin (Anti-tuberculosis vac 120 100 TOPV RV DTP-IPV/Hib Hepatitis B PCV7 at 6 weeks, 120 100
Action taken when children are ill
Health personnel have negative attitudes towards refugees 21 30.4 Do not have valid documentation to stay in South Africa 2 2.9. The main reasons given by nursing staff for the four days and longer delays were their inability to communicate in English and isiZulu (62.3%) and the negative attitudes of healthcare. When participants were asked about their means of transportation to health centers, 65.0% indicated that they use public transportation, while the remaining 35% walked.
Satisfaction with health care service delivery
For participants using public transport, the average transport varies from 10ZAR to 20ZAR ($0.73 to $1.47; US dollars) which is considered expensive by most when they do not have enough money for food. The frequency distributions for satisfaction of different service aspects of the last child health care consultation are depicted in table 7 below.
Distribution of health care service experiences during the last child health care visit Participants were asked to evaluate their level of satisfaction with the last health service
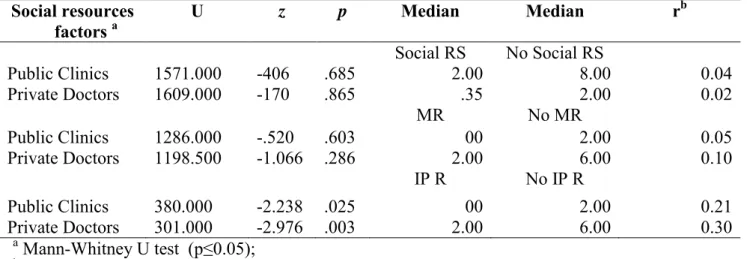
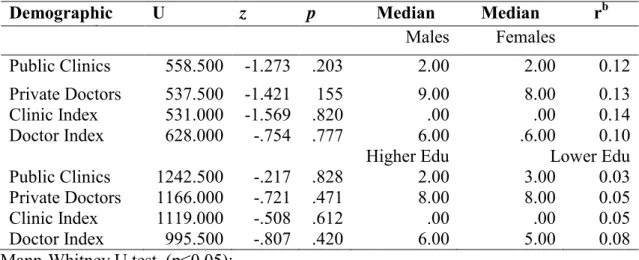
Indices of satisfaction with health appointments for both private doctors and public clinic visits were constructed by summing the items related to the various aspects of the consultation process as described in the frequency table above. The Mann-Whitney U test (table 8 below) performed on both satisfaction rating scales did not show any significant difference between gender and level of education (lower and higher levels. While not shown in table 8, it should be noted that the caregiver's level of education (No school vs. school) and SES (Not enough for the basics vs. enough for the basics) did not show significant differences in satisfaction with health care services.
Satisfaction with health care services in terms of household resources
No, I never feel happy, at the local clinic there are many things that can make you not feel happy. I spent more than 6 hours in the clinic and no nurse cared to talk to me. I myself have been to the private clinics before, so I know how expensive it is – but the services are well organized and of good quality (Female, participant 5).
Conclusion
The individual and household characteristics including the socio-demographic information, the socio-economic status, i.e. this will be followed by the views on the geographical accessibility of healthcare services, the availability of services related to their perceived child healthcare needs, and at finally, views on acceptability of health care, including their views on health care and the level of satisfaction with health care provided to their children.
Individual and Household characteristics of caregivers
- Individual Demographical Characteristics of caregivers
Furthermore, the ability to speak the language of the host country has been argued to reduce anxiety and thereby increase greater psychological well-being among refugees (Krumm, 2012). The barriers of language play out in different ways as the study results suggest and have a negative impact on healthcare accessibility and levels of satisfaction with healthcare services which will be discussed in more detail in the sections below. The refugees in the study reported that unless they can present their documentation, they do not receive health care. However, in emergencies no health care can be denied to foreign nationals (DoH, 2012).
Availability of health care services
However, long queues are a common complaint of the South African public healthcare system (Coovadia et al., 2009). The overall dissatisfaction with public healthcare is worrying as this appears to be an ongoing problem. The language barrier in public health clinics likely contributed to some of the dissatisfaction experienced by providers.
Introduction
Conclusions
The geographic accessibility of public health facilities improves access for refugees who do not have adequate financial means to travel to health facilities. Caregivers reported that they were very dissatisfied with the health services for their children, especially with the provision of health services in public health facilities. The negative attitude and discriminatory behavior of healthcare workers, in addition to long waiting times, contributes to caregivers' opinion of the poor quality of healthcare services.
Limitations of the study
Refugees' perceptions of their health status and quality of health care services in Durban, South Africa: A community-based survey. What does 'access to healthcare' mean? 2014).Family members' experiences of using interpreters in health care. Patients' satisfaction with health care services provided in the clinics of the city of Johannesburg municipality ((Doctoral dissertation, University of South Africa).
ETHICAL CLEARNCE TO CONDUCT THE STUDY
CONSENT FORM FOR INDIVIDUAL PARTICPANTS (CAREGVIVERS)
I also give permission for interviews to be audio-recorded, and for the transcribed interview material to be used for research purposes only. I understand that my participation is voluntary and that I have the freedom to withdraw from the study at any time should I wish to do so.
QUALITATIVE INTERVIEW SCHEDULE FOR CAREGVIVERS
QUANTITATIVE RESEARCH QUESTIONNAIRE SECTION A: DEMOGRAPIC INFORMATION
- The private doctor(s): (Not applicable – did not seek the help of a private doctor)
- The local clinic: (Not applicable – did not seek the help of the local clinic)
- A faith healer: (Not applicable – did not seek the help of a faith healer)
- The local herbalist (Not applicable – did not seek the help of a herbalist)
- The traditional healer (Not applicable – did not seek the help of a traditional healer)
- Satisfaction with clinic and private doctor A. Local clinic
When you arrived in South Africa, you and your family received a full health assessment. When your child is sick, how long do you usually wait before taking him/her to the clinic or doctor. 6. Did you feel that the nurse respected your opinions about your child's health needs.