Background: Although the prevalence of pneumonia in pregnancy is reported to be less than 1%, pregnancy status and risk factors associated with the development of pneumonia adversely affect pregnancy outcome. Methods: Pregnant women with clinical and radiological signs of pneumonia were selected from the maternity ward and delivery department of KEH. Pneumonia was significantly associated with adverse overall obstetric outcome in the presence of HIV-1 infection, antenatal treatment, anemia, and second-trimester reservation status.
Maternal pneumonia, maternal HIV infection, and the presence of medical and obstetric conditions were significantly associated with low birth weight and neonatal pneumonia. Conclusion: The presence of pneumonia in the antenatal period negatively affects maternal and neonatal morbidity and mortality.
LITERATURE REVIEW
Pneumonia in pregnancy
It is the third leading cause of indirect maternal mortality during pregnancy, childbirth, and the puerperium in the United States (Visscher and Visscher, 1971). In the cohort of mothers studied by Madinger et al (1989), preterm labor was precipitated by a number of maternal complications, including bacteremia (16%), empyema (8%), atrial fibrillation (4%), and respiratory failure requiring ventilation (20%). . However, Richey et al (1994) and Berkowitz and LaSala (1990) reported no higher complication rates of preterm birth in the presence of antenatal pneumonia.
In addition, premature birth and the development of chickenpox infection in the newborn may occur. Varicella pneumonia is more common in the pregnant population compared to the non-pregnant population.

Tuberculosis in pregnancy
Good et al (1981) conducted a retrospective study of activation and relapse of TB disease during pregnancy. In a recent retrospective review, EPTB accounted for 53% of TB in pregnancy with involvement of the abdomen, lymph nodes (cervical, intra thoracic, parasternal and axillary) and ischio rectal fossa (Kothari et al, 2006). There are few reports of concurrent TB and HIV infection during pregnancy, despite the greatest impact occurring in women of reproductive age.
Possible dynamics in cases of co-infection include pregnancy as a risk factor for the development of tuberculosis in HIV infection (Gilks et al, 1990), increased risk of postpartum tuberculosis in HIV-infected women (Leroy et al, 1995) and whether pregnancy represents any additional risk of developing TB (Espinal et al., 1996). Reports from Africa have shown an increased risk of developing tuberculosis in HIV-infected women after childbirth (Gilks et al, 1990; Leroy et al, 1995).
The global threat of multi drug resistant tuberculosis
This is a sign of poor control, resulting in the development of MDR TB (Dye et al, 1999). The median time to relapse when using first-line MDR TB treatment is 8 months (Migliori et al, 2002). The cost of treating multidrug-resistant tuberculosis is prohibitive for countries with limited resources.
Studies in the USA (Mahmoudi and Iseman, 1993), Cape Town (SA) (Dick and Henchie, 1998), the UK (White and Moore-Gillon, 2000) and the Netherlands (Geerligs et al, 2001) support these reported high costs of handling of MDR TB. Outcomes for MDR TB have improved with rapid investigation, availability of appropriate treatment and effective TB control programs (Turret et al, 1995; Tahaoglu et al, 2001).
HIV-1 and MDR TB in pregnancy
Overt teratogenicity was not observed in the 3 live births, and M tuberculosis was not cultured from their gastric aspirates, cerebrospinal fluid, or endometrial scraping (mother). M tuberculosis was not cultured from gastric washings and liver biopsy showed non-specific changes in histology. In the absence of culture evidence of an MDR pattern in the infant, it was elected not to start this infant on anti-tuberculosis therapy based on the mother's sputum profile as the mother was culture negative at birth and the infant responded to the regimen. selected.
Of the two HIV-1 exposed neonates, one was uninfected and liver and lung biopsies in the second case (the aborted fetus) confirmed prematurity with evidence of extramedullary hematopoiesis. In summary, successful treatment of MDR-TB during pregnancy is possible with appropriate and early interventions, as evidenced by the few reported cases.
METHODOLOGY
- Justification for the study
- Aim
- Hypothesis
- Objectives
- Study design
- Study site and patients
- Consent
- Ethical approval
- Statistical analysis
- Case definitions
The study arm consisted of HIV-1 infected and uninfected pregnant women with pneumonia and the control arm consisted of HIV-1. This is a similar difference in low birth weight as observed in the study of mothers co-infected with tuberculosis and HIV. Women with pneumonia were informed about the study and written informed consent was obtained if they agreed.
All asymptomatic mothers with clinical signs were excluded from the study, but the clinical details were recorded. The clinical history, physical condition, gestational age, clinical and radiological extent of the pneumonia were recorded at entry into the study.
RESULTS
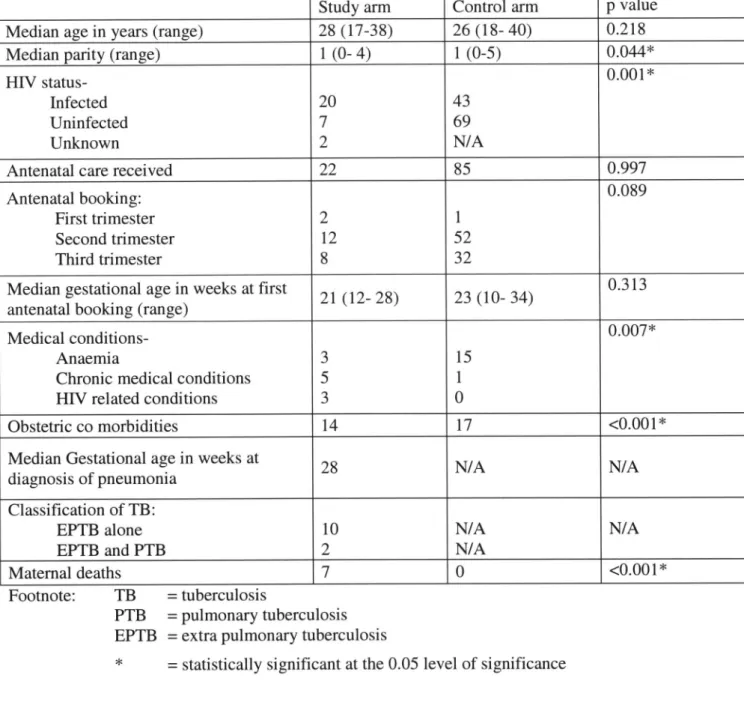
There were differences in age, parity, reservation status, HIV-1 infection, complete blood count, serum albumin levels in the presence of obstetric comorbidities. Of the 23 who received TB treatment, 16 were HIV-1 infected, five were uninfected, and the HIV status was unknown in the remaining two women. The mean gestational age at the first antenatal visit in the reserve population was 22 weeks (range 10–34).
There were no maternal deaths during labor and delivery in this group of women. The decision to initiate anti-TB treatment was made based on the mother's history and clinical signs in the newborn. Antenatal care did not statistically affect the mother's outcome in the presence of pregnancy pneumonia (p=0.169).
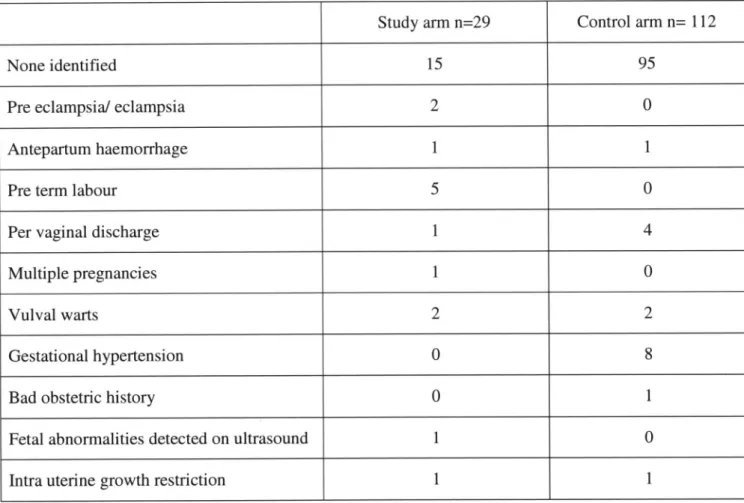
The diagnosis of pneumonia mainly occurred in the second trimester, but when pneumonia was present this variable had no influence on the maternal outcome (p=0.244). The difference in incidence of obstetric complications between the group of women with pneumonia and women without pneumonia reached statistical significance (p = 0.001), with complications occurring more frequently in women without pneumonia (64% vs. 28.8%). There was no association between pneumonia and obstetric outcome, either in the presence or absence of associated medical or obstetric conditions.
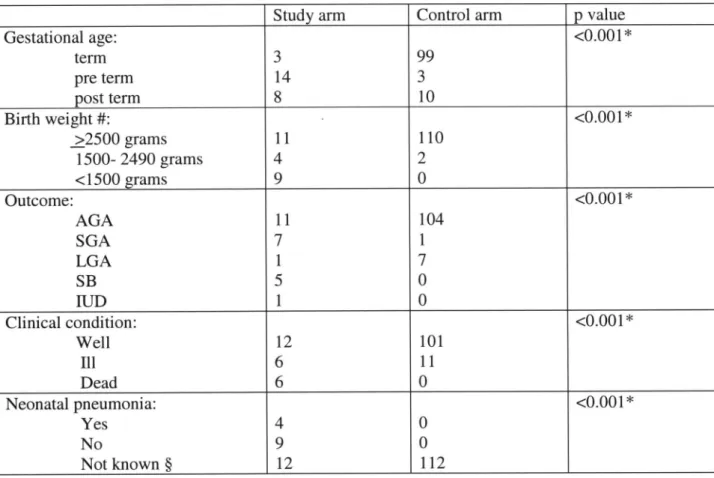
The presence of pneumonia and pneumonia in the presence of HIV-1 infection had a statistically significant effect on obstetric outcome (p=0.001 and p=0.000). In addition, maternal pneumonia and HIV infection in the presence of maternal pneumonia were significantly associated with neonatal death (p value <0.001 and =0.002, respectively). However, neonatal deaths were significantly associated with pneumonia diagnosed in the second trimester (p = 0.025), the presence of (maternal) health problems (p = 0.002), (maternal) pneumonia (p < 0.001), HIV-1 infection in the presence of pneumonia (p < 0.001) and absence of obstetric complications (p value = 0.003).
DISCUSSION
Twenty-two women with pneumonia sought antenatal care at mid-gestational age at their first antenatal visit late in the second trimester. Although our study population was too small to comment on the impact in the prenatal community, pneumonia in pregnancy was significantly associated with maternal and neonatal death. The contribution of pneumonia to maternal mortality in the KEH population has not yet been described.
Despite the prevalence of tuberculosis and HIV epidemics in women in the reproductive age group, documentation of the contribution of co-infection to MMRs has been limited to Zambia, India and Mexico, reporting MMRs of 6.3% to 25% (Ahmed et al., 1999; Juneja et al, 1994; Figueroa-Damiaan and Arredondo-Garcia, 1998). In the study arm, probable or suspected tuberculosis was present in 71% of deaths and HIV-1 co-infection in 86% of deaths, again highlighting the contribution of the twin epidemics. The impact of co-infection with tuberculosis and HIV-1 on CD4 count during pregnancy has been previously documented in the research setting, reporting a mean CD4 count of 348 cells/mm3 (Pillay et al, 2004b).
All neonates in the control arm were born alive and 18 live births occurred in the study arm. It was 280 times higher than pregnancies complicated by HIV-1 infection alone in the control arm and 2.8 times higher than in neonates exposed to co-TB–HIV-1 infection studied at the same center ( Pillay et al, 2004b). The detection of 4 cases of congenital pneumonia was limited to neonates in the study arm.
The protective efficacy of BCG vaccine in preventing pulmonary TB in adults and adolescents is controversial (Anonymous, 1972; Anonymous, 1980). The impact of pneumonia on obstetric outcome was significant in the presence of HIV-1 infection. In the few reported cases, one mother chose to terminate the pregnancy for social reasons rather than further management of the infection (Nitta et al, 1999) and one experienced preterm birth (Lessnau and Qarah, 2003).
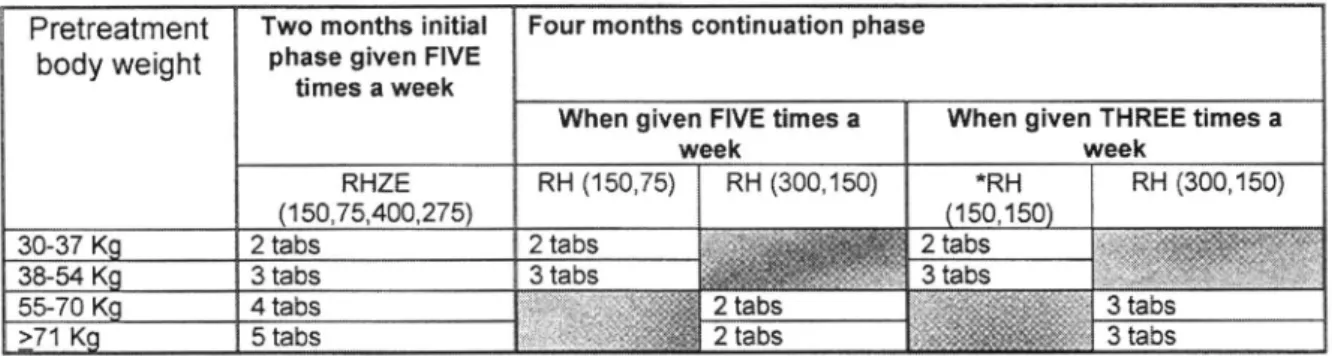
It is not within the scope of the study to comment on the development of tuberculosis in early infancy in neonates exposed to this disease during pregnancy. Appendix E.2: The use of fixed dose combination drugs in the treatment of tuberculosis in South Africa (Department of Health, SA, 2000a).
Directly observed therapy
Retrospective study of human immunodeficiency virus infection and drug-resistant tuberculosis in Durban, South Africa. BCG and mouse bacillus vaccines for prevention of tuberculosis in adolescence and early adulthood. Drug-resistant tuberculosis: review of the worldwide situation and the WHO/IUATLD global surveillance project.
Coninx R, Mathieu C, Debacker M, Mirzoev F, Ismaelov A, de Haller R, Meddings DR. First-line tuberculosis therapy and drug-resistant Mycobacterium tuberculosis in prisons. Impact of the human immunodeficiency virus epidemic on mortality among adults with tuberculosis in rural South Africa. Davies GR, Pillay M, Sturm AW, Wilkinson D. Emergence of multidrug-resistant tuberculosis in a. de Cock KM, Soro B, Coulibaly IM, Lucas SB.
Extrapulmonary and disseminated tuberculosis in HIV-1 seropostive patients presenting to the acute medical service in Nairobi. Impact of human immunodeficiency virus type 1 infection on the initial bacteriological and radiographic manifestations of pulmonary tuberculosis in Uganda. Risk factors and outcome of human immunodeficiency virus-infected patients with sporadic multidrug-resistant tuberculosis in New York City.
Murray J, Sonnenberg P, Shearer SC, Godfrey-Fausset P. Human immunodeficiency virus and the outcome of treatment for new and recurrent pulmonary tuberculosis in African patients. Impact of DOTS compared with DOTS-plus on multidrug-resistant tuberculosis and tuberculosis deaths: decision analysis. Tahaoglu K, TOrtin T, Sevim T, Atac G, Kir A, Karasulu L, Ozmen I, Kapakli N. The treatment of multidrug-resistant tuberculosis in Turkey.
Telzak EE, Sepkowitz K, Alpert P, Mannheimer S, Medard F, el Sadr W, Blum S, Gagliardi A, Salomon N, Turett G. Multidrug-resistant tuberculosis in patients without HIV infection. Primary and acquired drug resistance in black adult patients with tuberculosis in South Africa: results of an ongoing national surveillance programme.