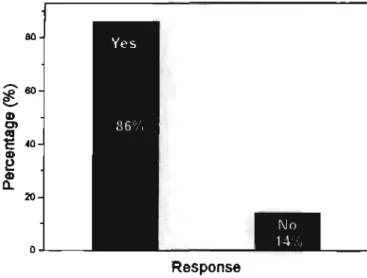
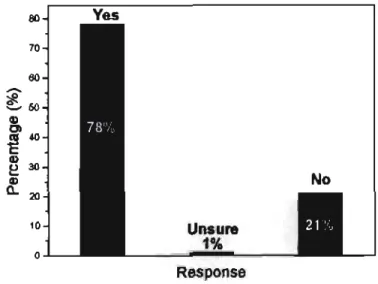
The aim of this study was to investigate the knowledge, attitudes and sexual practices of young people with mild intellectual disability (MMR) regarding HIV/AIDS. Knowledge of existence of HIV/AIDS 86 Knowledge of whether HIV causes AIDS 87 Percentage of misinformed per knowledge category 89.
LIST OF TABLES
LIST OF ABBREVIATIONS
MOTIVATION AND RATIONALE FOR THE STUDY
It is becoming increasingly clear that young women between the ages of 15 and 25 in South Africa are at particularly high risk of HIV infection (Wood & Jewkes, 1998). However, AIDS and HIV infection among persons with mental retardation remain virtually unexamined (Scotti, 1997), and although there has been an abundance of publications on adolescents and HIV/AIDS, there is little research on mentally retarded adolescents and HIV/AIDS.
AIM AND OBJECTIVES OF THE STUDY
The current study specifically involves outlining the knowledge, attitudes, and practices that individuals with mild mental retardation need to develop in order to practice healthy behaviors and reduce conditions that increase the risk of HIV infection. The findings will be useful not only to foster a better understanding of the psycho-educational dynamics of HIV infection in this particular group of adolescents, but also to tailor appropriate educational programs and promote further research in an effort to to increase our knowledge in addressing the problem of HIV/AIDS in this group of people.
DEFINITION OF TERMS
Intelligence can be defined as the general or global ability of an individual to act. Peer norms refer to the assessment of the likelihood of being desired by prominent others.
CONCLUSION
INTRODUCTION
DEFINITION AND PREVALENCE
One of the most widely accepted definitions of mental retardation was proposed by the AAMR. Prevalence figures on the composition of different categories of intellectual disability and the number of intellectually disabled adolescents could not be obtained.
DEVELOPMENTAL PROFILE
- Physical Factors
- Socio Emotional Factors
- Sex Behaviour
These factors thus further reinforce the turbulent period of adolescence among mildly mentally retarded adolescents. Mentally retarded persons pubertal growth does not differ from that of their non-retarded peers.
PERSONALITY DEVELOPMENT
While caregivers argue over ownership of responsibility for sex education, many mentally retarded youth continue to be sexually active and ignorant (Watson, 1980). In addition, mentally retarded youth appear to be more isolated, lonely, dysphoric, and angry than their counterparts.
INTRODUCTION
The chapter concludes with a discussion of barriers to the delivery of AIDS awareness messages to persons with mild mental retardation.
THE SOCIO-ECONOMIC CONTEXT OF HIV/AIDS
A South African National Youth Survey (2000) found that a significant minority of young South Africans are still unaware of the virus. Many men, aware of the risks of HIV infection, are now actively seeking younger girls in the belief that they are less likely to be HIV positive.
MENTALLY RETARDED PERSONS AND HIV/AIDS
Some students with disabilities are more likely than other students to believe in myths and misinformation because they cannot distinguish between reality and unreality. In an effort to be accepted by others or to gain attention (positive or negative), students with low self-esteem are more likely than others to engage in risky behavior.
PRESENT STATUS OF SEXUALITY EDUCATION
Six studies showed that sex education leads to either a delay in the initiation of sexual activity or a decrease in overall sexual activity. Until recently, sexuality education was neglected in most South African schools due to community, religious and parental attitudes.
HIV/AIDS PREVENTION
Initial evaluations of the program have shown that there have been problems in its implementation (Macintyre et al, 2000). Behavioral messages and prevention efforts need to be combined and links with health services need to be developed.
SEXUALITY EDUCATION FOR THE MILDLY MENTALLY RETARDED ADOLESCENT
Essentially, there appear to be two main conceptual factors that influence sex education for mildly mentally disabled persons, viz. Another issue that requires attention is the content of sex education programs for the mildly mentally disabled.
DIFFICULTIES IN IMPLEMENTING HIV/AIDS EDUCATION
This means that to teach people with mental retardation how to avoid HIV infection, sex must be discussed. There is much to know about HIV infection and the information available is often confusing, especially for people with mental retardation.
INTRODUCTION
MODELS OF CHILD AND ADOLESCENT DEVELOPMENT
Inhelder (1958), a pioneering developmental theorist applied the Piagetian model of cognitive development to persons with mental retardation. Vygotsky's socio-cultural theory (1934) offers a different lens through which to view cognitive development by emphasizing the importance of specific social processes, which.
BEHAVIOURAL MODELS OF HEALTH BEHAVIOUR
Attitudes comprise beliefs about the behavior in question, while social norms comprise an assessment of the likelihood that significant others would want the individual to engage in the behavior in question and their motivation to meet those expectations. The assumption of the theory of reasoned action is that the individual has the means, skills and opportunities to engage in the desired action.
THE SCHOOL SETTING AS A HEALTH PROMOTING ENVIRONMENT
The foregoing describes some theoretical models that contribute to our understanding of HIV/AIDS and can guide changes in HIV risk behavior. There is a growing population of young people in South Africa, with 36.3% of the population under the age of 15 (Health Promoting Schools, 1997).
CONCLUSION
INTRODUCTION
RESEARCH DESIGN
AIM AND OBJECTIVES
THE POPULATION AND SAMPLE
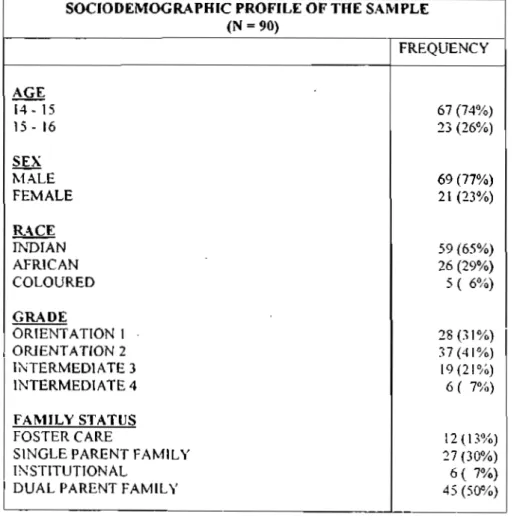
The school was established in 1986 by the Ministry of Education in recognition of the need to fill a gap in the continuum of services needed for young people with learning disabilities. This section describes the characteristics of the students, the curriculum and the length of stay at the school.
DATA COLLECTION INSTRUMENT
- Instrument Development Phase
- The Questionnaire
The content validity of the questionnaire was established by being evaluated by 2 researchers identified as experts in the field of HIV/AIDS research. The main purpose of the questionnaire was to elicit information about the sample's knowledge, attitude and sexual practices.
PROCEDURE
- Phase 2-Implementation
Because the subjects' literacy skills may have been limited, an interviewer-administered procedure was used, in which the questions were read aloud by the researcher. The researcher explained the purpose of the study, the inclusion of questions about sexual behavior, the confidentiality of the study, and the right to privacy and voluntary participation.
DATA ANALYSIS
RESULTS
INTRODUCTION
RELIABILITY OF PRIMARY SCALES USED IN THE SURVEY TABLE 2: Cronbach's Alpha Coefficient for KAP Scales (n=90)
Internal consistency was slightly poor on the remaining 3 scales (0.4166 to 0.4841), with item analysis not producing any significant improvement in the reliability of these scales. Cronbach's alpha coefficients could not be performed on the remaining scales because in some cases the items were not suitable for scaling and in others too few items comprised the scale.
KNOWLEDGE ABOUT HIV/AIDS
- Existence and Cause of HIV/AIDS and STDS
- Transmission of HIV/AIDS .1 Descriptive Analyses
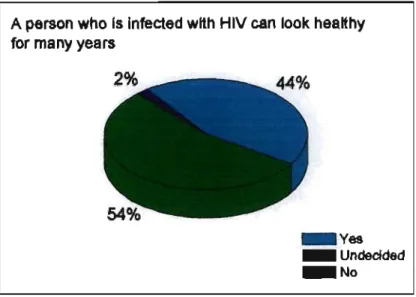
- Perceived Knowledge of HIV/AIDS
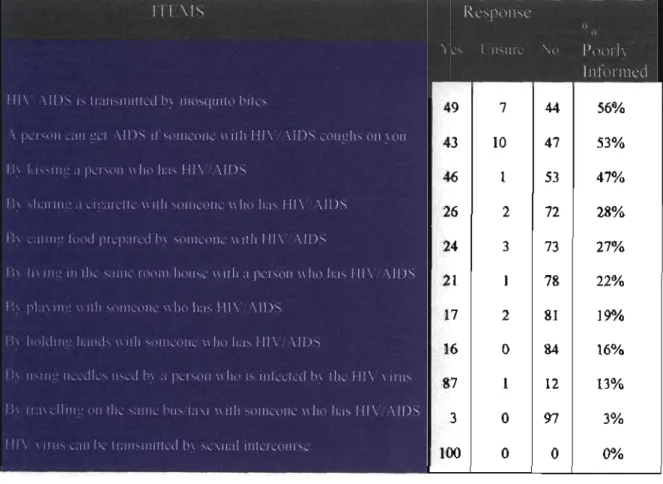
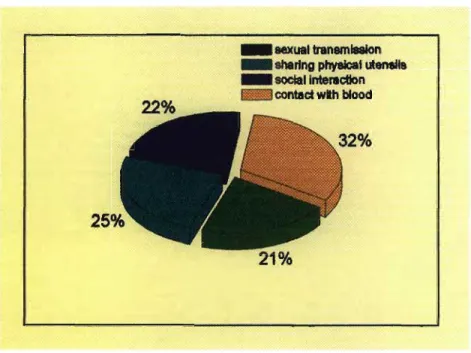
Despite good knowledge that HIV/AIDS can be transmitted through sexual contact (100%), almost half (47%) of respondents believed that HTV7AIDS can be transmitted by kissing an infected person and almost 1 in 4 respondents believed that HTV7AIDS can be transmitted through social interaction (22%). Similarly, significantly more women than men believed that HIV/AIDS can be transmitted by playing with an infected person (cf** 6.38, df.=l, p<0.05).
PERSONAL EXPOSURE TO HTV/AIDS
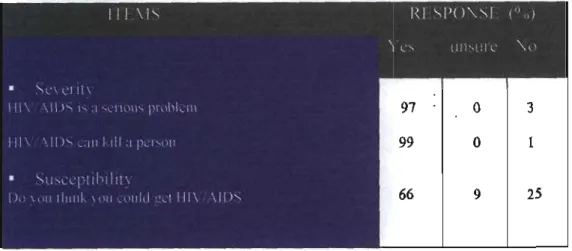
THREAT
- Fear
There was a statistically significant racial difference in identifying HIV/AIDS as a serious problem (^=7.64, df.=2, p<0.05), with fewer Africans than Indians and Coloreds reporting AIDS as a serious problem . Similarly, there was a statistically significant racial difference in susceptibility (df.=2, p<0.05), with fewer Africans compared to Indians and Coloreds indicating susceptibility to HIV/AIDS.
PREJUDICE
Regarding perceived methods of protecting oneself from HTV infection, the highest number of responses included condom use (51%), followed by abstinence (35%). A negligible number of respondents indicated staying away from infected individuals (7%) and not coming into contact with blood (7%) as viable means of protection.
BEHAVIOURAL PRACTICES
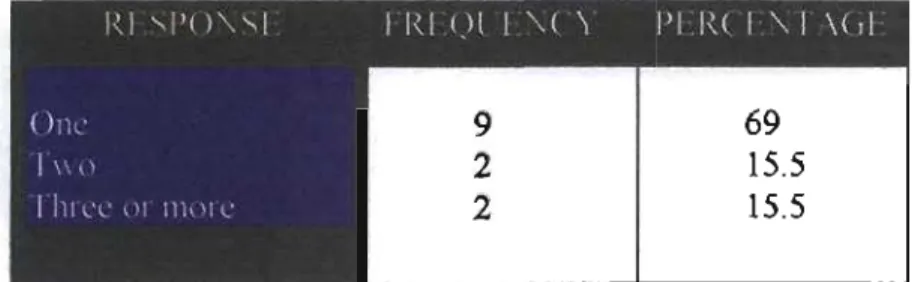
- Number of sexual partners in the last six months
- Condom usa2e
Of those who were sexually active, 69% indicated that they had 1 partner, 15.5% indicated that they had 2 partners and 15.5% indicated that they had 3 or more partners. In response to the question, "Do you carry a condom with you", it is alarming to note that only 1% of respondents always indicated, 2% sometimes indicated and 97% never indicated (Figure 11) .
PEER NORMS
Item analyzes revealed a statistically significant race difference regarding girls engaging in premarital sex (tf2 =6.172, d.f.=2, p<0.05), with more Indians than blacks and Africans indicating that girls should not engage in premarital sex.
SELF EFFICACY
Significantly more Africans than Indians and Coloreds indicated that their sexual partners would refuse to use condoms (jf=11,799, df.=2, p<0.05). Similar findings were observed across genders (df.=2, p<0.01), with significantly more women than men reporting that their sexual partners will refuse to use condoms.
HEALTH SEEKING BEHAVIOURS
- Care
- Support
EDUCATION
- Sexuality Education at School
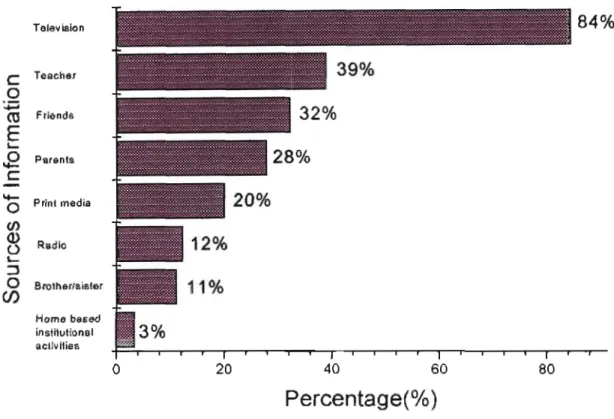
HIV/AIDS exposure occurs within the family, with 28% of respondents indicating that parents and 11% of respondents indicating that siblings are a source of information regarding HIV/AIDS. In the above analysis, subjects were asked for their opinions regarding appropriate and suitable HIV/AIDS initiatives at school.
INFERENTIAL ANALYSIS OF KAP SCALES
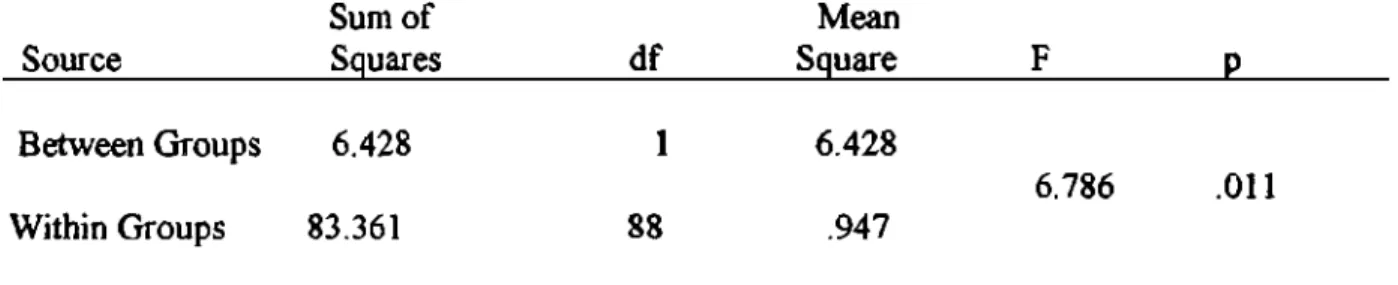
A one-way analysis of variance (ANOVA) was performed with sexual activity as the independent variable and personal exposure to HIV/AIDS as the dependent variable. A one-way analysis of variance (ANOVA), using knowledge of condom use as an independent variable and use of a condom by sexually active respondents as the dependent variable was performed (Table 17).
SUMMARY OF RESULTS
43% of respondents believed that HIV/AIDS can be transmitted when an infected person coughs on you. Similarly, significantly more women than men believed that HIV/AIDS could be transmitted by playing with an infected person.
INTRODUCTION
KNOWLEDGE ABOUT HIV/AIDS
Similarly, significantly more women than men believed that HIV/AIDS can be transmitted by playing with an infected person. Over half (56%) of those questioned believed that HIV/AIDS can be transmitted by mosquito bites.
PERSONAL EXPOSURE TO HIV/AIDS
Therefore, in an effort to increase condom use, HIV/AIDS awareness programs should emphasize both severity and personal susceptibility to the disease. Just over 1 in 3 respondents indicated that they knew someone who had died of HIV/AIDS.
THREAT
- Fear
In terms of personal susceptibility, just over two-thirds of respondents reported that they were susceptible to HIV/AIDS. Similarly, a significant racial difference in susceptibility was found, with fewer Africans than Indians and Coloreds reporting susceptibility to HIV/AIDS.
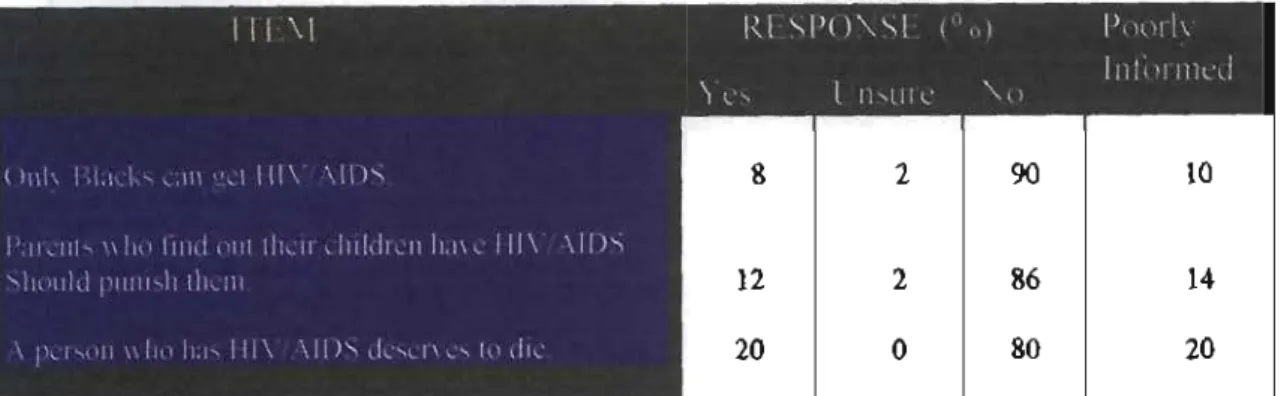
PREJUDICE
The 20% of respondents who stated that an infected person deserves to die may just be a reflection of the underlying attitudes and prejudices in society, stemming from fear and ignorance. This highlights the urgent need to improve negative attitudes and prejudices among MMR adolescents in order to increase threat perceptions and thereby reduce sexual risk behaviors.
PREVENTION OF HIV/AIDS
This is not surprising given that respondents who hold a prejudiced attitude do not want to be associated with the disease, possibly because of the negative connotations and stigma attached to HIV/AIDS. This may be because respondents are not involved in serious relationships or do not understand the risk of multiple partners in the transmission of HIV/AIDS.
BEHAVIOURAL PRACTICES .1 Sexual Activity and Frequency
Statistical analysis showed no significant age and class differences in the number of sexual partners in the last 6 months. Statistical analysis showed that respondents with a high level of personal exposure to HIV/AIDS reported having fewer sexual partners in the past 6 months.
PEER NORMS
In determining views on "premarital sex," respondents were asked whether it was okay for boys and girls to have sex before marriage. Respondents showed moralizing attitudes, with 69% indicating that boys should not have sex before marriage and 71%.
SELF EFFICACY
Respondents were also asked whether their sexual partners would agree to use condoms if asked. 80 percent of respondents reported that they would not find it embarrassing to use a condom.
HEALTH SEEKING BEHAVIOURS
Siblings fared poorly in the above rating, with only 7% of respondents indicating that they would turn to a sibling with a question about HIV/AIDS. However, in the above analysis, only 10% of the respondents indicated that they prefer to talk to their peers about HIV/AIDS-related issues.
EDUCATION
- Sources of Information
- Sexuality Education at School
The analysis indicated that the home was hardly a source of information about HIV/AIDS, with 28% of subjects hearing about HIV/AIDS from parents and 11%. This is in line with Zazayokwe's (1990) analysis of the reactions of South African communities which showed that parents and siblings do not condone the open discussion of HIV/AIDS as it involves the discussion of sex.
CONCLUSIONS
Respondents who had more knowledge about transmission methods were more likely to view HIV/AIDS as a personal threat. Although the vast majority of respondents expressed a tolerant attitude, more than half indicated that they would keep their HIV status secret, indicating that they are aware of the rampant social stigma and discrimination faced by people suffer with HIV/AIDS.
LIMITATIONS
Nevertheless, the survey provides comparative data between racial and gender subgroups of the sample. This study did not examine the effects of these variables and their impact on respondents' HIV/AIDS knowledge, attitudes and practices.
THEMES AND DIRECTIONS FOR FUTURE RESEARCH
Therefore, it is strongly recommended that future research include triangulated designs involving large random samples to foster a better understanding of the contextual factors that inform adolescent MMR knowledge, attitudes, and practices related to HIV/AIDS. We hope that this small-scale study represents the beginning of a systemic research effort to address the challenges of the MMR adolescent AIDS epidemic.
RECOMMENDATIONS
- Policies and Procedures
- Behaviour Change Programmes
- Systemic Whole-School Interventions
- Monitoring and Evaluation
Highlighting the severity of the disease and the personal susceptibility of MMR adolescents to contracting HIV/AIDS. Increasing students' exposure to people with HIV/AIDS to increase knowledge and improve attitudes.
Fifth National HIV Survey among Women Attending Public Health Service Clinics in South Africa. A study of the prevalence of severe mental retardation among colored children in an urban community.