Investigating whether a meaningful geographic model of sociodemographic variables for schizophrenia can be constructed and whether it can determine areas of high schizophrenia susceptibility. The potential of the schizophrenia susceptibility model and the accessibility model, despite the crude and incomplete variables used, was evident.
LIST OF DIAGRAMS, TABLES AND MAPS
APPENDIX
QUESTIONAIRE FOR 'EXPERTS'
TABLES OF K\VAZULUNATAL CENSUS DATA Table 1: Local Councils within each District Council ofKZN
CHAPTER ONE: INTRODUCTION
Determining the geographical accessibility of public provincial hospitals offering psychiatric services to the population (particularly to persons with schizophrenia). Initially, the objectives and hypotheses are outlined, followed by the methodological protocol of the study.
CHAPTER TWO: LITERATURE REVIEW
THEORETICAL FRAMEWORKS UNDERLYING
THE STUDY
MEDICAL GEOGRAPHY
DEMOGRAPHY
EPIDEMIOLOGY
- Epidemiological Terms
In demography, we study various characteristics of the population, such as stable characteristics (gender, age, race or ethnicity) and economic characteristics (literacy and education, occupation and income). It is estimated that 0.025 to 0.05% of the total United States population is treated for schizophrenia annually.
SCHIZOPHRENIA
CONCEPT
SCHIZOPHRENIA COSTS
- Gender
- Marital status
- Location
- Population Density
- Seasonality of birth
- Culture
- Socio-economic status
- Occupation
- Migration
In the USA, the cost of treating schizophrenia, excluding indirect costs, has been estimated to be close to 0.5% of the gross national product (Warner and de Girolamo, 1995). This variable is appropriate for South Africa due to widespread poverty (White Paper on Social Welfare, 1997) and the expected migration of Africans from rural areas to informal settlements closer to the centers of metropolitan areas (Dor, 1994).
ACCESS TO MENTAL HEALTH CARE
The Bill of Rights does not guarantee individuals the right to health, but rather the right to access health services (Constitution, 1996). The Ministry of Health has stated that their aim is to ensure that all South Africans have access to health resources by adopting a District Primary Health Care (PHC) model.
GEOGRAPHICAL INFORMATION SYSTEMS
- INTRODUCTION
- DEFINITION
- APPLICATIONS
- HEALTH GIS UNIT, KZN, DEPARTMENT OF HEALTH
- POTENTIAL ERRORS IN USING THE GIS
The GTS database differs from other database applications because all information in the GIS is linked to a spatial reference. Shannon Rushworth (BSc Honors specializing in Geographic Information Systems, University of Natal-Pietermaritzburg) is the GIS Manager.

CHAPTER THREE: METHODOLOGY
INTRODUCTION
AIMS AND HYPOTHESES
Examining the geography of schizophrenia in terms of accessibility to mental health care for individuals diagnosed with schizophrenia. What number of certified patients diagnosed with schizophrenia would fall within the larger ranges of schizophrenia susceptibility.
Sample
- Instruments
- Validity and Reliability
- Ethical Considerations
- Describing the Database of Certified Patients with Schizophrenia
- GIS MODEL OF SCHIZOPHRENIA SENSITIVITY
- Demographic details of KZN province and population
- The model of schizophrenia sensitivity
- GEOGRAPHICAL ACCESSIBILITY
- Accessibility model
- Application of the Accessibility model
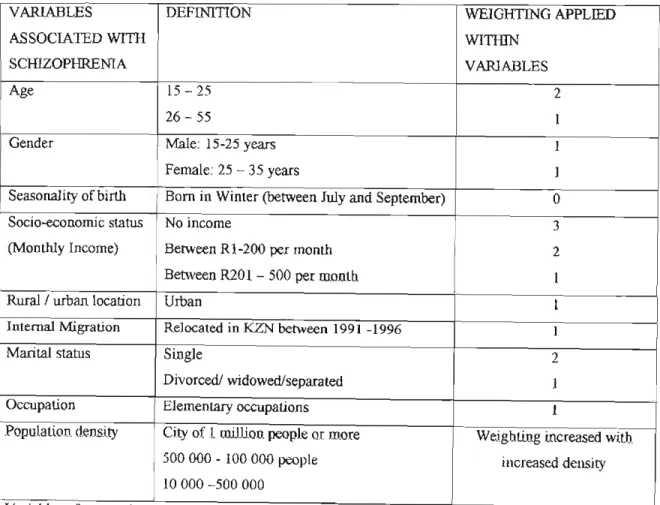
What percentage of the population in KZN is located within the areas of greater schizophrenic sensitivity. All the variables used were equally weighted and considered totally independent of the others. The percentage of the population in KZN that fell into each range of schizophrenic sensitivity was identified (See section 4.3.2).
CHAPTER FOUR: RESULTS
DESCRIPTION OF KWAZULU NATAL (KZN)
DESCRIPTION OF PATIENT SAMPLE
- Gender and cultural composition
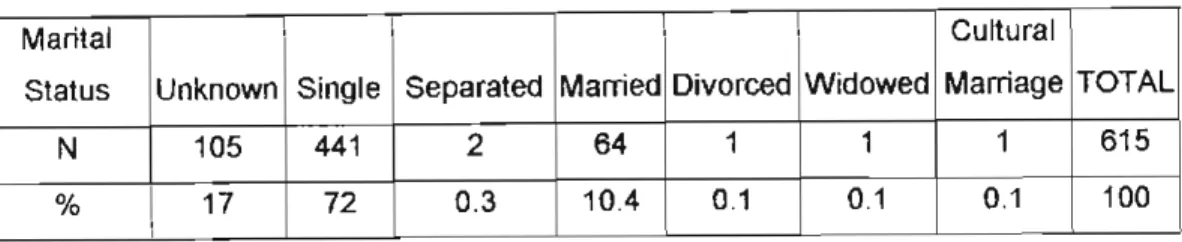
- Marital Status
- Seasonality of Birth
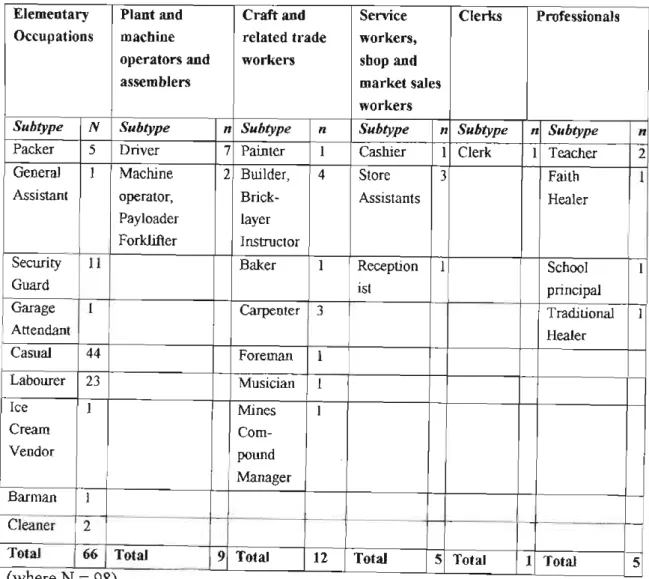
- Employment
- Occupation
- Religion
- Previous Admissions
- Length of Stay
- Diagnosis
- Location
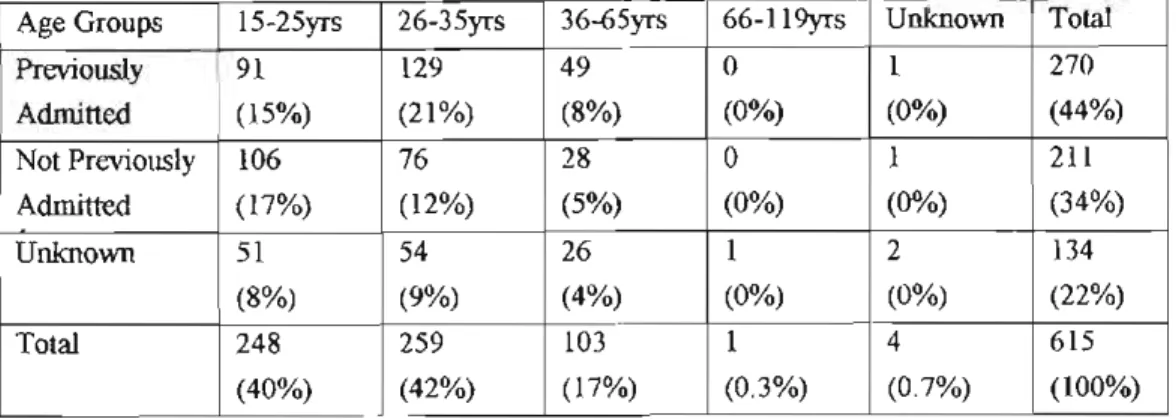
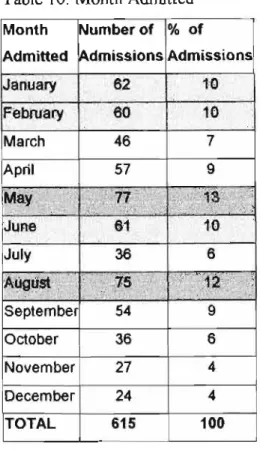
Fifty-three percent of the sample was not employed, and thirteen percent was employed (see Table 6). Forty-four percent of the patient sample had been previously admitted compared with just over a third (35%) who had not been previously admitted (see Table 9). The smallest sample of patients was admitted in the months of November and December (see IQ table).
Patients Originate
M!P 2: KwaZulu-Natal provincial hospitals providing psychiatric services and areas from which Psychiatric services and areas from which. Kwasimama Provincial Clinic (Durban DC) 1 Ntuzuma Morrisons Post Provincial Clinic (DC 21) 1 Umzumbe Mpumalanga Provincial Clinic (Durban DC) 1 Mpumalanga Provincial Clinic Mtubatuba (DC 27) 1 Mtubatuba NKweldCwd) ezana Provincial Hosoita/ (DC28) 1 Esikhawini. Note: Italics highlight provincial hospitals; the shaded areas indicate the transition of DCs between the place of reference and the place of residence; Chc stands for Community Health Center.

Ma~ 3: Referral Patterns for PS'lchiatric Patients
Summary
Forty-four percent of patients had been previously admitted compared with just over a third (35%) who had not been previously admitted. Most patients stayed in hospital between 15 and 99 days, the most common length of stay being between 4-6 weeks. Three quarters of the referring institutions referred patients who lived in the same CK as him.
SCHIZOPHRENIA SENSITIVITY MODEL
- Is there evidence of a geographical pattern?
Map4:. Schizophrenia Sensitivity
LEGEND
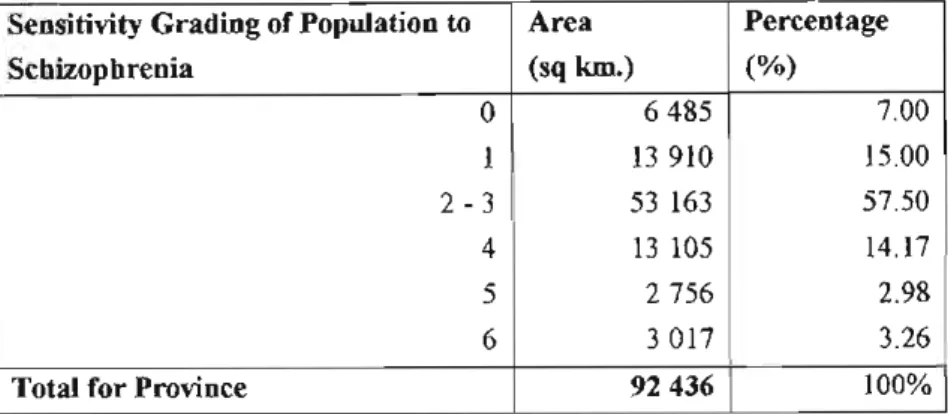
- Percentage ofKZN population falling into the varying ranges of schizophrenia risk
- Description of the relationship between the schizophrenia sensitivity ranges and certified patients
- DESCRIPTION OF ACCESSIBILITY MODEL
- Access and the KZN population
- Accessibility to Psychiatric Health Services
- Access and the certified patient population with schizophrenia seen at Fort Napier Hospital
- Relationship between the accessibility rating and schizophrenia sensitivity ratings
- Summary
Umlazi, Kwamashu and Inanda had 76% of the total number of patients within the SSR level 6. The largest concentration of the KZN population was found within the 6 sensitivity range (34%), and then the 2-3. The greatest concentration of the KZN population was found in the area representing accessibility range 1 (58%), followed by a progressively decreasing population density through accessibility ranges and 4 (6%) (see Table 20).
CHAPTER FIVE: DISCUSSION
Gender and cultural composition
These findings also correlate with the literature in that at least half of patients with schizophrenia present before the age of 25, suggesting that the other half present after the age of 25 (American Psychiatric Association, 1994). It must be taken into account that the admission criteria for FNH are more likely to have contributed to the fact that no patients under the age of 16 were admitted, rather than to the fact that there were no such cases. Furthermore, patients who may have been readmitted were included in the data; therefore, assumptions about age of onset may not be accurate.
Marital Status
Seasonality of Birth
For the 1994 elections in South Africa, all South African citizens were required to obtain an identity document in order to vote, ensuring that most people had their dates of birth. Another explanation for the poor number of dates of birth could be that patients were too psychotic on admission to provide reliable or consistent personal information.
Employment
Occupation
Certainly, some individuals with higher incomes and occupational status would receive private mental health care. Wiggers & Sanson-Fisher (1997) identified a problematic issue where patients experience possible discrimination in the treatment offered, based on their occupational status. Wiggers & Sanson-Fisher (1997) conducted a study in Great Britain, which found a difference in occupational status in the duration of GP consultations.
Religion
Care must be taken in interpreting these results, as the fact that the sample was obtained from a public hospital must be taken into account. This is a major concern regarding patients with schizophrenia, as many tend to be socioeconomically disadvantaged. In addition, this mental illness often manifests in the patient's social disability and may expose the patient to further discrimination in the provision of services.
Previous Admissions
It may also be a reflection of earlier ethnocentric, primarily Christian value systems that may have overshadowed other possible belief systems. With increasing advances made in the understanding of brain neurochemical transmitters and receptor sites, new antipsychotic drugs are being developed, providing more effective and cost-effective antipsychotic treatment. In an effort to save costs, mostly cheaper drugs (which often tend to have greater side effects) are being made.
Month Admitted
Length of Stay
Knapp (1997) suggests that cost-effectiveness in relation to chronic mental illness should be interpreted carefully, arguing that patients with chronic mental illness tend to have unique needs compared to those with acute illness. In addition to the obvious costs of hospitalization, there are also many indirect and intangible costs (Suleman et al, 1997; Torrey, 1998). This highlights the need for multifaceted funding, management and treatment of schizophrenia where the overlapping.
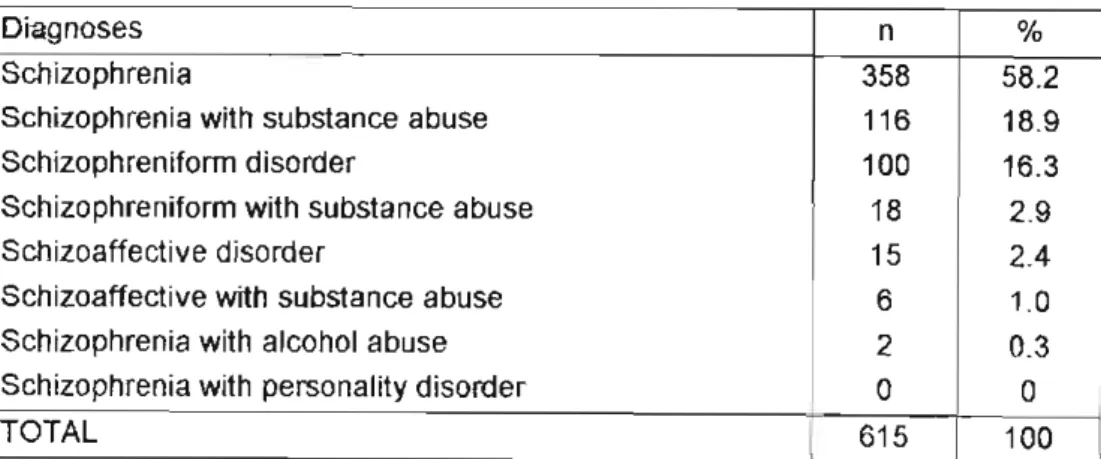
Diagnosis
Health professionals currently rely on a mental status examination, which usually involves a clinical interview and observation of the patient's behavior (Sue et al, 1994). It is difficult to diagnose a person as having schizophrenia on first admission because of the chronological criterion of DSM-IV, where the disorder must have lasted for at least 6 months previously and been evident for 1 month at the time of diagnosis (May 1998; Sue et al ., 1994). The changes in the criteria for schizophrenia may increase the reliability and validity of the diagnosis, but make the comparison of different studies over a period of time the same.
Location
Health Care Quality Policy for South Africa (September 2000); Mental Health Care Act (2000); White Paper on Transforming Public Service Delivery (October 1997); Health Care Quality Policy (April 1997); White Paper on Health System Transformation. Fifty-nine percent of the population is now urbanized and approximately 7 million urban residents are squatters (Dawes & Donald, 1994). Fifty-eight percent of patients, who were referred outside the central center of their residence, had come from cities from which other patients were referred by institutions within the same CK.
DISCUSSION OF SCHIZOPHRENIA SENSITIVITY MODEL
- Is there evidence ofa geographical pattern?
- Percentage ofKZN population falling into the varying ranges of schizophrenia risk
- Description of the relationship between the schizophrenia sensitivity ranges and certified patients
- Summary
- Access and the certified patient population with schizophrenia seen at Fort Napier Hospital
- Relationship between the accessibility rating and schizophrenia sensitivity ratings
Again, this seems to indicate the role that population distribution may play in the model's patterns. The majority of sites (7 of 9) assigned 10 or more patients fell into the high sensitivity ranges for schizophrenia and into the easy access ranges. Seventy-three percent of cities fell into the range of easy accessibility, while only 55% of cities (6) fell into ranges of high susceptibility to schizophrenia.
CONCLUSION
The limitations of this study included the use of crude variables in the models which resulted in the loss of some sensitivity and comprehensiveness of the purpose of the model. To make a difference in these patients' lives, the quality of life of the majority of the population in KZN must be improved. This will include ensuring a basic education, increased employment opportunities, and raising the standard of living of the majority of South Africans to above the international poverty line.
QUESTIONAIRE GIVEN TO THE 'EXPERTS'
Feel free to discuss and debate this section with others. age - gender - education - marital status - seasonality of birth - occupation. Feel free to add further definitions and comment. The terms used are subjective and need to be defined to make them better. The variables included are aimed at the general public. Can you think of any others more specifically related to psychiatry?
TABLES OF KZN CENSUS DATA
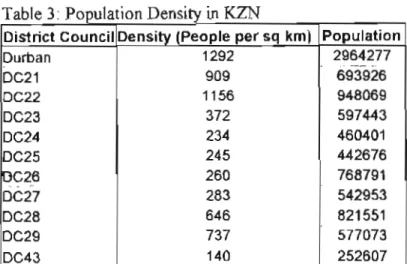
The others showed a density of less than 400 people per square kilometer, with DC43 less than 150 people per square kilometer. In the age distribution of women and men, the age category 0–14 dominated overall and within each DC (see Tables 5 and 6, respectively). Just under 30% of KZN's workforce is employed. In Des outside Durban, the employment percentage ranges from 7 to 23.