The development of this guidance was designed within the principles of health equity and social capital. When we talk about the approach to social capital in this guide, we therefore mean the following:
Case Studies
Introduction to case studies
The goals of the projects were in line with the social capital approach, and the funding was aimed at building strong and lasting connections and networks between residents and local service providers. Although each project took place in a different area, the communities and projects shared many similarities.
Case Study One: Yangara (DJ Lane) Reserve Project
The regular events were organized by council staff with the active involvement of Friends of Sullies. Most of the residents who were involved in the redevelopment of the reserve lived in the immediate vicinity of the reserve.
Case Study Two: The Parks Helix Project
The agencies built closer ties with each other and worked together on the final activity of the project 'The Walking Trail'. One of the remarkable results of the project has emerged almost in the face of adversity.
Case Study Three: Kilburn Blair Athol Community Capacity Building
The Kilburn Blair Athol Community Capacity Building Project brought together several teams to manage specific areas of the project, its directions and joint activities. We discuss below four existing initiatives that were the focus of our research, as recommended by local community health and mental health service staff; CaFE Enfield, Youth Link, Community Garden and INCCA.
Once the connections are made, parents and children slowly become involved in activities in the center (usually starting with the most informal ones such as playgroup or crafts). They become active in decision-making and the management of the center and networks with other parents in the community.
Strengths of the CaFE Enfield Project
In this way, the parents involved in the center made all the important decisions related to the day-to-day operation of the center. The second, an advisory group of service organizations, consisted of members of the service providers involved in the center.
Many parents involved in the center consider their involvement 'life-changing' to say the least. In addition, the close participation of the volunteers in the day-to-day running of the center and in the management of its activities ensures the sensitivity of the center to the real needs of the community.
Challenges
The group developed questions for a survey and each person had to give the questionnaire to six friends and invite them to the next meeting. The group is open to all young people in the area and at times there were 30 people who came to the meetings. Currently the primary agency involved with the Garden is the Enfield Community Mental Health Services.
The plot of land next to the house was cultivated and maintained by the group as a communal garden for a number of years. After that time the house and land were sold and after a short search in the local community the garden was moved to a local church.
The group grew out of it and new participants were recruited directly by young people from their circles of friends and peers. The Community Garden was established as a response to a 'community garden' which was identified as important to the local community during the consultation.
The government is sending more and more people into the community from different places and let's face it, the attitude of the community towards some people is not very good and it makes them feel much more isolated, whereas if they could come here , everyone understands that they all have a good day or a bad day and they can discuss their problems with other people and sometimes that just makes the difference (participant). This initiative was set up in response to the theme that the residents repeatedly raised during the consultation; one of the things they wanted to happen in the area was accessible and affordable art workshops. One of the ambitions of the project was to achieve independence from funding and teachers through self-study (where workshop participants would take responsibility for guidance).
Challenges
However, despite the difficulties, some workshops continued and saw regular high-level participation. Discussions with these groups revealed a strong sense of ownership of the group and a positive supportive dynamic of the workshops. Due to the wide range of these needs, the program broke up into smaller projects that later became independent of each other.
Building community networks and engaging isolated community members, as well as creating links with service providers were the main objectives of the projects. One of the projects experienced sustainability difficulties due to an over-reliance on volunteers.
Factors important for success of the programs
As has been emphasized by the staff involved in the case studies, the best way to ensure participation was to provide a 'vehicle' that would interest and engage the residents and that could provide fun. Often the activities led to the creation of community art, which was later displayed in the area. It is important that all stakeholders were represented in the management committees, including residents' reference groups, service agencies and funding bodies.
The agencies involved in the case studies made the building of trusting cooperation with the communities the basis for a sustainable relationship. The programs in the case studies worked to develop strong links between residents and local service providers, to ensure long-term, sustainable cooperation between the relevant stakeholders.
Participation in community development programs
Due to the high demand on time and resources for such activities, some of the case study projects reported significant difficulties in involving local communities. In response, some programs have developed ways to help participants with transportation, providing buses or carpools. And one of the reasons for that is that men don't have access to groups unless it's a club.
Another problematic aspect of the projects was a minimal involvement of indigenous, migrant and refugee residents. It is clear that the complexity of the factors cannot be fully covered in this short section.
Your Program
Getting ready - an audit of organisational capacity
This part identifies 4 main areas where capacity has been shown to be influential in the effective application of social capital theory in practice. CAPACITY INDICATOR 1 Commitment to underpinning values CAPACITY INDICATOR 2 Knowledge of terms and concepts CAPACITY INDICATOR 3 Experience in community development CAPACITY INDICATOR 4 Quality of collaborative relationships. You will need to decide who in the organization(s) is best placed to undertake this audit.
We suggest that you review each of the four indicators of organizational capacity in turn, treating each as follows: Social capital, as described in this guide, summarizes some of the values that address the question of what makes a "good" society, and the role of government and civil society in helping to achieve social goals.
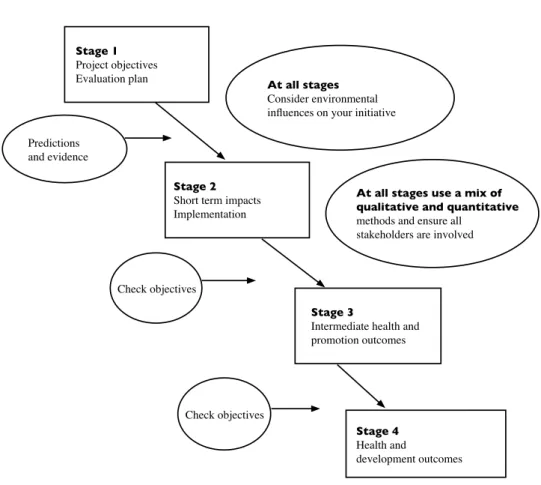
- Program Planning and Evaluation
- Measuring Change
First, reading about social capital and health equity is the first step toward embedding these values into the organization's structures and systems. In order to apply social capital to practice, it is not necessary to have a comprehensive knowledge of its theoretical foundations or a detailed understanding of the competing definitions. Recognition of the value of these skills is an indication of an organization's readiness to embark on social capital approaches.
Two of the projects (Helix and Kilburn Blair Athol) involved relatively complex programs spanning three years. For this reason, it is a good idea to take stock of the level of skills present in the organization and identify the employees and community members with this kind of expertise.
Explaining Concepts
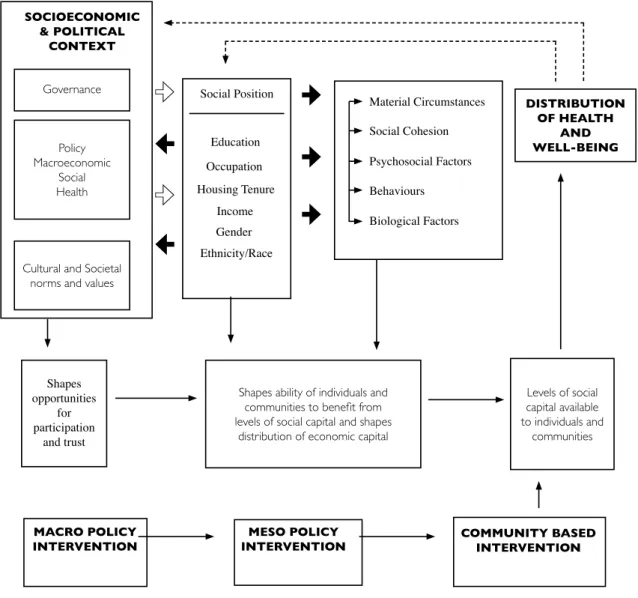
Health Equity and its determinants
The discipline that explores the reasons for the existence of health inequalities is called social epidemiology. Its latest initiative to tackle the problem of health inequalities is the Commission on the Social Determinants of Health, established in 2005. The conceptual framework underpinning the Commission's work takes social and economic factors as primary influences in shaping output of health inequalities.
They are unlikely to be able to address the upstream contextual and structural determinants of health inequalities. CSDH (2008) Closing the gap of a generation: Health equity through action on the social determinants of health.
Social Capital and Health
The literature suggests that at least some aspects of social capital are associated with health outcomes. However, there is also evidence that some aspects of social capital can have negative effects on health. Why is it important to consider the theory of social capital and how it may relate to health.
The daily activities of on-site interventions reflect the underlying theories of social capital and how it can influence health. Consistent evidence of links between aspects of social capital and health

Understanding Related Social and Community Concepts
The research uses quantitative and qualitative measures of social capital to advise policy makers in facilitating social inclusion. Thus social inclusion/exclusion, community capacity building and community development all overlap with our central concept of social capital. Aware of the imprecise understanding and inconsistencies in the use of social capital, the team developed a comprehensive review of the social capital literature.
The brief aims to inform policy makers of the value of the social capital approach. It provides definitions of social inclusion and social capital, and summarizes research findings showing the links between social determinants of health and social inclusion.
COMMUNITY BUILDING AND COMMUNITY INVOLVEMENT
- truSt 1
- rECiProCity
- SoCial lifE
- HElP and aSSiStanCE
- CiviC and Community grouP involvEmEnt
- Community/nEigHBourHood lifE
Research evidence suggests that there are important pathways linking social capital to health and well-being. Individuals and their networks: At the individual level, social capital (including strong social networks and social support, involvement in voluntary organizations, and levels of trust, reciprocity, and belonging) has been associated with improved health and well-being. Neighborhoods: There is evidence that neighborhoods with higher levels of social capital have better health outcomes.
Low social capital (mainly in terms of trust, social networks and feelings of social connectedness) also contributes to social exclusion. These case studies offer insight into how community projects can contribute to the development of social capital.
