The fetal phase begins at a gestational age of 10 weeks and lasts until birth (Gomella, et al., 2020). A pre-COVID study found that mothers with HTN had a high risk of preterm birth (Shulman et al., 2017). For COVID-19, the same result was seen in mothers who had both COVID and preeclampsia (Papageorghiou et al., 2021).
15 Several studies showed that pre-COVID mothers with DM had a higher chance of lower uterine caesarean section (LUCS) and large baby (Persson, et al., 2018) than those without DM. Another study showed that the mother with DM has a high risk of having a premature baby (Kong, et al., 2019).
Origin of COVID-19
Spread of COVID-19
Global Situation of COVID -19
Situation of COVID -19 in Bangladesh
Hospital Situation in Bangladesh
Maternal Health Care Situation
UNICEF warns that countries must ensure that pregnant women still have access to antenatal, delivery and postnatal services, even if research shows they are no more at risk from COVID-19 than other groups.
Mode of delivery in COVID -19
Complication in Pregnant Women
Enhanced Chance of Serious Illness
In contrast to those who are not pregnant, those who are pregnant or have just given birth are at greater risk of developing severe COVID-19 disease. The physical changes that pregnancy brings can make it easier to get sick from respiratory viruses like COVID-19. When suffering from a serious illness, a COVID-19 patient may require: hospitalization, admission to a hospital intensive care unit (ICU) and a ventilator or other breathing aid device.
Risk Increasing Factors
Effect on the Results of Pregnancy
Studies on Influence of COVID Situation on Neonates
The primary outcome was the incidence of PTB between the 2 groups before and during the COVID-19 pandemic. They report no reduction in preterm birth rates in their United States hospital system during the COVID-19 pandemic. They took 140 pregnant women who tested negative for COVID-19 versus 70 pregnant women who tested positive for the virus.
The probability of having a normal-weight baby was shown to differ somewhat between COVID-19-positive (75.0%) and COVID-19-negative women (80.2 percent). There is an association between participants' COVID-19 status and poor infant birth outcomes (preterm birth, CS delivery and low birth weight). According to multivariate logistic regression, women with COVID-19 infection were 2.15 times (95 percent confidence interval, 1.06 to 4.37) more likely to deliver a preterm baby than women who did not have the infection.
Women with COVID-19 infection were 3.27 times (95 percent confidence interval, 1.51 to 7.07) more likely to have a CS than women without COVID-19 infection after controlling for variables. The multivariable logistic regression model also revealed no association between the pregnant women's COVID-19 status and the newborns' low birth weight (aOR, 1.56; 95 percent CI, 0.64 to 3.80). Women who tested positive for COVID-19 were older than those who tested negative for COVID-19, and there was a strong correlation between COVID-19 status and age groups (p-value <0.001).
In addition, the non-COVID-19 group experienced slightly more problems related to pregnancy than the COVID-10 group (7.9 versus 4.3 percent).
Gestational Age
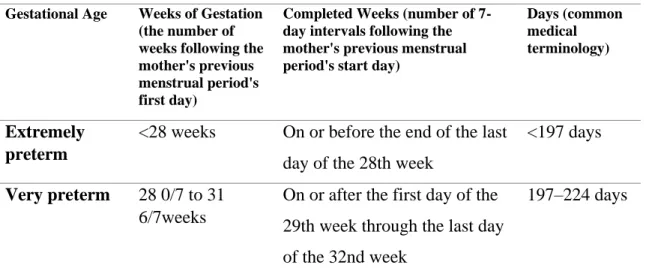
Classifications of Gestational Age
On or after the first day of the 33rd week to the last day of the 34th week. Preterm <37 weeks On or before the end of the last day of the 37th week. On or after the first day of the 35th week until the end of the last day of the 37th week.
On or after the first day of the 38th week through the end of the last day of the 39th week. On or after the first day of the 40th week through the end of the last day of the 41st week. On or after the first day of the 42nd week through the end of the day of the 42nd week.
Preterm Birth
- Causes of Preterm Birth
- Incidence of Preterm Birth
- Indication For Hospitalization of Preterm LBW Infants
- Complications of Preterm Baby
- Prognosis of Preterm Baby
- Complications on Mother Triggered by Preterm Birth
Preterm births (births that occur before 37 full weeks of pregnancy) are thought to affect 15 million babies a year and the number is rising. The leading cause of death for children under the age of five is complications of preterm birth, which contributed to an estimated 1 million deaths in 2015. Premature birth is a problem that affects the entire world, with more than 60% of births prematures occur in Africa and South Asia.
All but three of the 65 nations with accurate trend data show an increase in preterm birth rates over the past 20 years. Better measurement, rising maternal ages and underlying maternal health issues such as diabetes and high blood pressure, increased use of infertility treatments leading to higher rates of multiple pregnancies, and changes in obstetrical practices such as an increase in premature births by caesarean section are some possible causes. This is if birth weight <1800 gm, gestational age <34 weeks, baby unable to take feed from breast/cup and spoon, any sick neonate, regardless of birth weight/gestation (Khan & Rahman, 2011).
Birth Weight
- Relation of Birthweight to Gestational Age
- Birth Weight Recording
- Importance of Birth Weight
- Relation of Maternal Nutritional Status with Fetal and Postnatal Growth 31
- Classification of Birth weight
Birth weight matters, for example - the second most common cause of death in newborns is low birth weight. Low birth weight was also associated with higher demand for health care and higher health care costs. Rates of low birth weight have recently increased, highlighting the need for greater focus (Gomella, et al., 2020).
There are 7 types of birth weight for newborns namely extremely LBW or Micro Preemie, extremely low birth weight (ELBW), very low birth weight (VLBW), low birth weight (LBW), normal birth weight (NBW), high birth weight (HBW) or Big Baby, Very High Birth Weight (VHBW). Newborns with a birth weight of less than 1000 g are considered extremely low birth weight (ELBW) (2 lb, 3 oz) babies. Very low birth weight (VLBW) infants, or less than 1500 g at birth, account for only approximately 1% of all births, yet account for nearly 50% of neonatal deaths (Marcdante & Kliegman, n.d.).
A baby not growing properly during pregnancy is another factor in very low birth weight. Low birth weight can be prevented by eating a balanced diet during pregnancy and not using drugs, smoking or drinking alcohol. Very High Birth Weight (VHBW) is also called fetal macrosomia if the birth weight is >4500 grams.
High birth weight babies were more likely to require a caesarean section and to experience fetal death.
Maternal Comorbidities
- Diabetes Mellitus During Pregnancy
- Disorders of Hypertension During Pregnancy
- Asthma During Pregnancy
- Thyroid Dysfunction in Pregnancy
- Premature Rupture of Membranes (PROM)
According to research, a low-glycemic diet and exercise during pregnancy can reduce the incidence of macrosomia. One of the common medical problems associated with pregnancy is hypertension, which has a major impact on maternal and perinatal morbidity and mortality. These are hypertension, proteinuria, gestational hypertension, preeclampsia, eclampsia, HELLP syndrome, chronic hypertension, superimposed preeclampsia or eclampsia, chronic hypertension with superimposed preeclampsia and eclampsia.
A previously normotensive and nonproteinuric lady develops hypertension to the level of 140/90 mm Hg or more, which is a symptom of preeclampsia, and it is a multisystem disease of unclear origin. Maternal complications during pregnancy include labor, puerperium eclampsia, sepsis, preterm birth, accidental hemorrhage, oliguria and anuria, visual impairment, blindness, cerebral hemorrhage, and acute respiratory distress syndrome (ARDS). Maternal complications of untreated hyperthyroidism are miscarriage, premature birth, preeclampsia, congestive heart failure, placental abruption, thyroid storm and infection.
Fetal and neonatal complications of untreated hyperthyroidism include IUGR, prematurity, stillbirth, hypothyroidism, and increased perinatal morbidity and mortality. Premature rupture of membranes is a term used to describe any spontaneous rupture of membranes that occurs after 28 weeks of pregnancy but before the onset of labor. Premature PROM refers to a rupture of the membranes that occurs before 37 full weeks of pregnancy, while the term PROM refers to a rupture of the membranes that occurs after 37 weeks but before the onset of labor.
Membrane rupture that lasts more than 24 hours before birth is termed prolonged membrane rupture.
Studies on Influence of COVID Situation on Maternal Co-morbidities in
Study Area
Study Design
Study Population
Development of Questionnaire
Data Collection
Data Analysis
The study includes 713 number of cases in pre-COVID and COVID periods to find out if there is any association between COVID and preterm birth. Infants with intrauterine death (IUD), stillbirth, dilatation and curettage (D and C), ectopic pregnancy, ectopic pregnancy, and threatened abortion were excluded from the analysis.
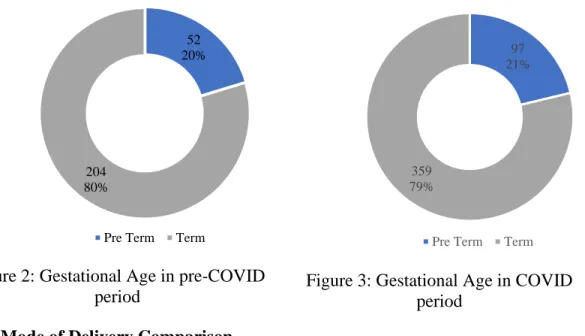
Preterm-term Comparison
Live babies whose gestational age was between 28 weeks and 42 weeks were included in this study.
Mode of Delivery Comparison
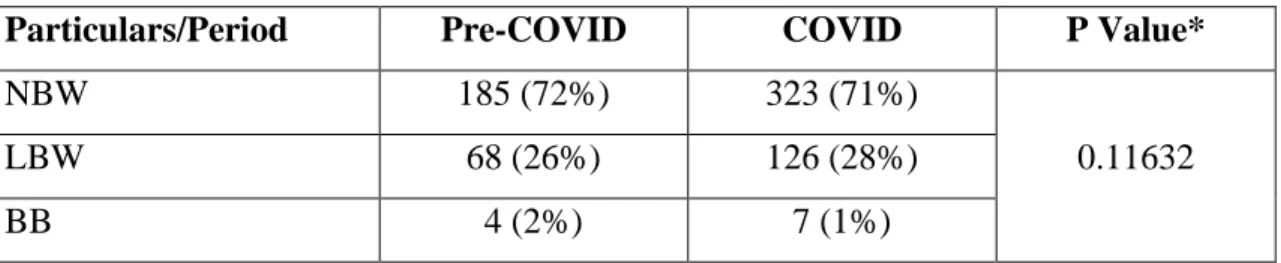
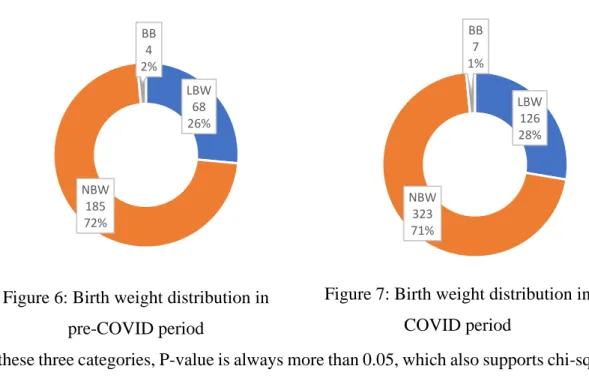
Birth Weight Comparison
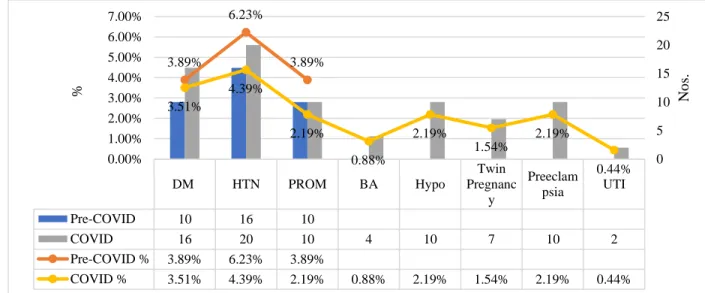
Prevalence of Diseases
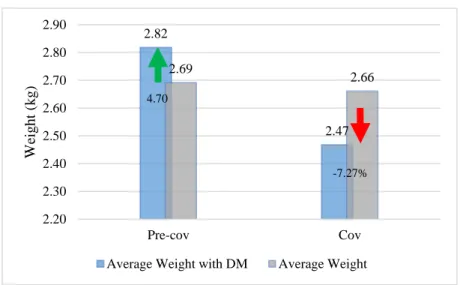
Comparison of Preterm, Term and Weight of Babies of DM Mothers
Comparison of Preterm, Term and Weight of Babies of HTN Mothers
49 It was also observed that babies of HTN mother's average weight in pre-COVID and COVID time was similarly less than the average weight of all babies shown in Figure 10.
Comparison of Preterm, Term and Weight of Babies of PROM Mothers
50 It was also found that for babies of mothers who had PROM, their average birth weight was 19.62% less than the average weight of all babies in the pre-pandemic period. During the COVID era, it decreased to 37.06% of the average weight of all babies, indicating that more low birth weight babies were born than in the pre-COVID era, as shown in Figure 11.
Situation of Childbirth from Mothers with Other Complicacies
Many studies have been conducted to understand whether the number of preterm births increases or decreases during COVID 19. This study was conducted during pre-COVID (June 2019-December 2019) and during COVID-19 (June 2020-December 2020) to understand whether there is any association between preterm birth, birth weight, mode of delivery and other associated maternal factors with COVID 19. The study clearly shows that there is no evidence of an association between preterm birth and COVID 19 in the study population.
The study further confirms that there is no role of COVID 19 in child birth weight distribution. The findings of this study may be useful in understanding the role of COVID-19 in mothers and infants. The association of term and preterm birth with COVID-19 positive mother could not be assessed in this study.
Every now and then we learn new knowledge about COVID-19 and the process should continue. The association of term and preterm birth with COVID-19 positive mother is also a scope of future investigation. Consideration of psychological stress, socio-economic conditions, maternal age, educational qualifications, employment status and their interaction with COVID-19 may improve the field of study in the future.
An unprecedented reduction in very low birth weight (VLBW) and extremely low birth weight (ELBW) infant births during the COVID-19 lockdown in Ireland: a "natural experiment" allowing analysis of data from the previous two decades. Pregnant mothers and babies born during the COVID-19 pandemic threatened by strained health systems and disruptions in services. Available at: https://www.unicef.org/bangladesh/en/press-releases/pregnant-mothers-and-babies-born-during-covid-19-pandemic-threatened-strained-health.