Planning, Organizing
and
Management
of
the
Collaborative
Project
on
Breast Cancer
Santoso
Cornain*
Abstrak
Kanker payudara lelap merupakan masalah penting baik di negara maju maupun di negara yang sedang berkembang, yang memerlukan peneLitianlebihlanjutdalambeberapaaspek. Suatupenelitiankerjasamatentangetiologidanklinikopatologikankerpayudaraantara Jepang dan Indonesia telah dilaksanakan. Perencanaan, pengorganisasian dan manajemen dari proyek kerjasama tersebut dikem-bangkan di bawah koordinasi baik tim Jepang maupun tim Indonesia. Baik tujuan umum dan tujuan khusus dan hipotesis yang sesuai ditetapkan dan dirumuskan berdasarkan tiga aspek penelitian, termasuk penelitian epidemiologik, klinik dan patobiologik. Proyek tersebut telah dirancang dalam fase-fase yang dimulai dengan penelitian pendahuluan ('pilot study') dan diikuti dengan penelitian definittf. Pembahasan meliputi
5
fase manajemen proyek, yaitu 2 fase perencanaan Qtenetapan dan perencanaan) dan 3 fase implementasi (pengorganisasian, manajemen I pengelolaan dan pengakhiran), yang dimodifikasi sesuai dengan proyek penelitian khusus. Di antara berbagai upaya yang sesuai maka pembinaan tim dengan kepemimpinan telah menjadi sangat penting untuk diperhatikan, karena beberapa hal yang dihadapi i.e. kelompok profesional dan ilmiah, tim multidisipliner dan proyek penelitian internasional.Abstracts
Breast cancer remains as an important problem in both deveLoped and developing countries, which needs further investigations in several aspects.
A
collaborative sludies on the etiology and clinicopatholoy of breast cancer between Japan and Indonesia has been carriedou|.
The planning, organizing and management of the collaborative project were worked out under the coordination of boththeJapanese and the Indonesian teams. Both general and specific objectives and cort'esponding hypotheses were defined and formulated
in respect to a lhreefold studies inclutling epidemiological, clinical and pathobiological studies The project has been designed in phases initiated by
pilot
study and followed by definitive,study. The description covers 5 phases of project manatement, namely 2 phàsesof
planning (definition and planning) and 3 phases of implementation (organizing, management I controlling and terminating)iith ro^"
modification as to adiust Io specific research project. Among related attempts team building and leadership have become very important which needed special attention, due to several respects to deal with i.e. professional and scientific group, muyidisciplinary team andi n 1e rnat i ona I rcsea rch proj ect.
Keywords:
colLaborative project, planning, organizatioq management, implementation, breast cancer, team, Indonesia-Japan.Department of Anatomic Pathology and Research Cenler
for
Medical
Science and Technology, Facultyof
Medicine, Universityof
Indonesia, Salemba 6, Jakarta 10430, In-donesia.Coordinator of the Indonesian leam, JapanJndonesia Joinl Study on Etiology and Clin'rcopathology of Breast Cancer.
Breast cancer remains as an
important
câncerproblem,
both
in the
developed countries, such
as Japan andin
thedevelopillg
olles, such asIndonesia.
The
datacol-lected
frorn
13 Pathology Laboratories
spread
throughout Indonesia by
the National
Center for
Pathology
basedCancer
Registry
showed that
breastcancer
ranked the
second
among females,
18.03
%relative
frequency
(ASCAR=
agedstandardized
can-cerratio
17.847o)in
1988and
18.214%(ASCARI7.46
%)
in 1989-'''
Similar findings
were also revealed
in
two
Population
basedCancer Registries at
two
prov-inces:Yogyakarta
andSemarang.'
repre-136
Cornain
senting
the similar situation
in
the geographical
areaand ethnical group,
i.e. Asia
and
Afrika.a
Further-more, the
estimates
could be
used
to
generate
hypothesesof etiological
factors.
The
amual
incidence
of
breast cancer
in
Japan
hasbeen reported
to
be
lower,
1.e.12.l-16.6 per
100.000females,
than iu America,
i.e.
71.7
per
100.000
females,
asindicated in
the
CancerIncidence
in
Five
Continents, published-by
theInternational Agency
onResearch
on Cancer.)
Increased
fisures
have
beenestimated
and reportedin
later studiesï-8, namely up to2l
per
100.000
females
in
Japan
and up
to
91
per
100.000
in
Northern America.
Such
difference
hasattracted several investigators
tolook
upon several
aspectsof
breastcancer,
including
theepidemiological, clinical and
pathological
studies,by paying attention
to
thebiological
behaviour
of
the disease aswell
as theearly
breast cancer issues.An International
collaborative Study
on Breast cancerhas been proposed
in
order
to
allow
comparative
studies
looking
on both the Indonesian patients and the Japaneseones,
in
respect
to both
the
similarities
anddissimilarities.
A rnultidisciplinary
groups/teams
were
established,including
theepidemiologists,
breast ca llcer su rgeons and pathologists/irnmunopathologists
frorn both
sides.
The
Aichi
Cancer Center,
NagoyaCity
University,
Nagoya
University,
Nagoya
and the CancerInstitute
(Ganu
Ken),
Tokyo,
Japan have beencollaboratineg with
the
Faculty of Medicine,
Univer-sity of
Indonesia,
Jakarta.The study
has beeninitiated by
thesupport
of
a threeyear grant
No.
01042007
(April
1,
1989-March
31, 1992) under the auspicesof
theMinistry
of
Education, Science andCulture,
theGovemment of
Japan and theauthorization
by
the
Dean,
Faculty
of
Medicine,
Universi
ty
of
Indonesia, No.
4383/PT02.H4.FK/E
I88.
Favorablesituation
wasgiven
by the fact that the issuesof
breast cancer
were
consistent
with two
among thepriorities
of
the
prograrnlnes
of
the
Faculty
of
Medicine, University
of
Indonesia, namely the fields
of Oncology
&
Degenerative
Disease and the HurnanReproductive Health.
The
preliminary
study has revealed thatfatty
consulnp-tion was found
aruong
other significant
risk
factors.Both
teamswere interested
to
study
further
about thenutritional
factors, relative
to the Indonesiansituation.
The
nutritionists,
both frorn the
University
of
In-donesia and the Research andDevelopment
Centerfor
Nutrition
of
theMinistry
of Health,
were considered to be addedto
theworking
teams.MedJ
IndonesCorresponding
to
theprogress
andthe
findings
atwo
yearextension grant
wasprovided,
i.e.
No.
O4O42OL3(April
1,1992-March
31,
1994).The present paper
will
describe theplanning,
orgariz-ing
and managementof
theinternational collaborative
study.
The description
will
cover
5 phasesof
project
management,' namely
2 phasesof planning (defining
and planning) and
3
phases
of
implementation
(or-ganizing, management/controlling and terminating)
with
some
modifications
as
to
adjust
to
similar
guidancelo'11 and tofit
tospecific
reseairch pro ject.r2'r3Planning the
collaborative study
F
urther
situutian
analy
sisDuring
theearly Consultation Meetings
thedefinitive
planning
of
thecollaborative study,
a researchproject
with
three
fold
study namely
the
epidemiological
aspecls,clinical
aspects andhistopathological
aspectsof
breast cancer,was
put
forward. In
addition to
theinformations
about the breast cancerproblems both
in
Indonesia
andin
Japanmentioned
above, thesituation
analysis has revealed
that the materials, namely
thenumber
casesand
controls, could be
expected
to
becollected
in Dr.
Cipto
Mangunkusumo National
Central
GeneralHospital,
Jakartain sufficient
number
i.e.75 to
100 per annum. Sincethis
is thebiggest
stategeneral hospital,
the
majority of the
patients
visiting
thehospital were
expected toconsist
of low
tomiddle
socioeconomical
class people.As
counterpart,
the
Cancer
Institute,
Tokyo had
thehighest number
of
breast cancer patients
in
Japan.High level
laboratory
andclinical
expertise were
alsoavailable
in
both
places.
Strong
epidemiological
groups
of
both sides also support substantially
the theme of thejoint
study emphasizing
on theepidemio-logical
study.
Establishment
of strategies
and
collaborating
teamsThe collaborating
teamswere established, narnely
the Japanese teamwhich
will
work with
their
counterparts the Indonesianteam.
The coordinator
of
the Japanesefeam was
Dr.
Yoshiyuki
Ohno,
Epidemiologist,
Chairman
of
theDepartment
of
Preventive Medicine,
formerly
at
Nagoya
City
University and later
atNagoya
University,
Nagoya;
while
the
members wereDr.
Nakako
Kubo,
Epidemiologist, Department of
Preventive
Medicine,
Nagoya
City
University,
Susumu Watanabe, Surgeon, Departrnent
of
Surgery,Cancer
Institute,
Tokyo.
During
later
phase, Dr.
Nakako Kubo
was replaced
by Dr. Kenji Wakai
andDr.
Sadao
Suzuki, Epidemiologists,
Department
of
Preventive
Medicine,
Nagoya
University.
The
coor-dinator of
the Indonesian team was
Dr.
SantosoCor-nain, Imrnunopathologist, Department
of
Anatomic
Pathology,
Faculty
of
Medicine, University
of
In-donesia,
Jakarta;
while
the
memberswere
Dr.
JoedoPrihartono and
Dr.
Setyawati
Budiningsih,
Epidemiologists,
Department
of
Community
Medicine, Faculty
of
Medicine, University
of
In-donesia, Jakarta,
Drs.
Didid
Tjindarbumi, Muchlis
Ramli
and
Idral
Darwis,
Surgeons,
Department of
Surgery, Faculty of Medicine,
University
of Indonesia,Jakarta,
Drs. Gunawan
Tjahjadi,
Esti Sutrisno
andEndang
Sri
Roostini,
Pathologists,
Faculty of
Medicine, University of
Indonesia,
Jakarta.The coordinators were
supposed
to
function
as
theleaders of the
rnultidisciplinary
teams and atternpted toobtain
full
support
from
their
headsof
the departments towork
toward the relevant
goals.Supervisory support
has beenprovided by
the Deanof
the
Faculty of Medicine,
University
of Indonesia.
Cor-responding
support
hasbeen also obtained
from
theDirector
of
Dr.
Cipto
Mangunkusumo
Hospital
andDirector
of
Research
and Development Center for
Nutrition, Ministry of
Health.
The
linkersystern within
the tearn was also establishedin
order
to
encourage
direct communication as
re-quired
during
thestudy.
In
each
study
field, the
tearn was supported
by
cor-responding
working
group including
interviewers,
nurses,nutritionists
andlaboratory
technicians.Amqng related attempts team building and
leader-ship'-^'
have
becorne
very important which
neededspecial
attention,
dueto
several
respectsto
deal
with
i.e.
professional
andscientific
group,multidisciplinary
tearn and
intemational
researchproject.
Designing and writing
research
proposal
Further
planning
has been discussedin
both
thejoint
meeting tretween the Indonesian and Japanese teams
in
the Consultation
Meeting
andin
thelocal
team meet-ings.The purpose and
objective
ofthe
study has beenfurther
defined
and
written in
the
official
proposal
for
grant
application. Thus, the three
folds
study including
epiderniological, clinicopathological and nutritional
aspects
of
breast cancer have been
clarifiod with
general andspecific objectives
for
eachfield.
The collaborative
research
was
designed
in
phases,initiated
with pilot
study
followed by definitive
study.
The epiderniological study
on risk
factors
in breast
cancer was planned
as case-control study.rr
Eligibility
of cases and
controls
were determinedin
the methodol-ogy(given
in theaccompanying paper). A
preliminary
qestionnaires and
its
guidelines
for
interviewers
were developed and testedin
thepilot
study.
The question-nairewere then standardized
aftersome
modification
for
further
datacollection in
thedefinitive
study.
Thestandardized questionnaire
were printed
with
copiesusing non-carbonized
papersfor direct
datadistribu-tion
to both
Japanese andIndonesian
teams.
SeeAp-pendix-A.
They
were
made
in
English
and in
Indonesian
languange.
The
English
version was
sentto
Japan,while
theIndonesian version was meant
for
comprehernive
useby
the nursesfor intewiewing
theIndonesian breast cancer
patients and controls.
The
manualfor
interviewer
wasgiven.
SeeAppendix-
B.The
clinical
study was planned
for
analyzing
clinical
aspects
of
the
disease andspecial
clinical
study
form
was developed
for
datacollection.
SeeAppendk-C.
The
histopathological
study wasplanned
for analyzing
histopathological
features
of
breast cancers.
Similar
sfudies were conducted in Japan,
applying
basic designof
case-controlstudy.
In
theextersion study
further nutritional
analysis was plannedby developing
specialquestionnaire. This
was also testedin
a pilotstudy
beforestarting
thedefinitive
study
of nutritional analysis. For
the extention study
the
questionnaire
for
epidemiolgoical study
were
simplified to
accompany the questionnaire
for
nutri-tional
study.
SeeAppendix-D
and.Appendix-E.
Implementation of research project.
The
implementation
includes
organizing,
controlling
and
terminating
theproject.
O rganizing the
proj
ec t.After
approval
of
theproposal the components
of
theresearch
project
werecommunicated
to the team mem-bers and related supervisorsin
order toallow
sufficient
preparation
for implementing
the
project.
The
teamswere provided
with
the available informations
on
breast cancerin
Japanese*orn"rr.l4'15
It
was considered
important to
standardize
the
138
Cornain
Therefore, the Indonesian pathologist was
sentto
theCancer
lnstitute, Tokyo, to allow
common
agreementin
thehistopathological
identification
ofbreast
cancercases. The general rules for_clinical
andpathological
recording
of
breast cancert" were thoroughly
dis-cussed
with direct clinicopathological
presentations.For the clinical study
in
Indonesia
it
was
agreed toapply
the rnanagernentprotocol of
the IndonesianSur-gical Oncology
Association"
which
was adaptedfrom
widely
accepted standards.The activities
of
the teams were coordinated
andor-ganized
specifically.
Theepidemiologists
supervized thecollection of
epiderniological
databy
interviewing
cases
and
rnatched controlsn
by weli
trained
inter-viewers using
standa rdizeclquestiomai
res.The
identification
and diagnosisofbreast
cancer caseswere performed
by
the
clinicians
(breast
surgeons)'which
also evaluated
relatedclinicopathological
data.The
pathologists
were
responsible
for
evaluatiug
thehistopathological
featuresof
specimensderived
from
breast
çallcer
câses.Modified WHO
histopathological
classification
recommended
by
JapaneseSociety for
Breast
Cancer was used.In addition,
theinterest
wasgiven
toinclude
thestudy
of
the
expression
of hormonal
(estrogen
and
progesterorÙ receptors,
sittce the
tearn
c,o"nsideredit
migtrt
Ueapplicable to
the present
studyls'l9
and
for
clinical
lnanagement.
The
immunopathologist
wasresponsible
to
take care
of
establishing the
relatedimmunoperoxidase
techniques.The study
has been
inwater
with pilot
study
in
two
phases,
carried
out
in
December
1988
and
January1989.
It
was followed
by
definitive study
in three
phasescarried out
until
November
1991.Since the preliminary
results20inclicated interesting
findings, inter alia that
fatty
food
consurnption
wasshown as significant
risk
factor
in
the
Indonesian
breast caucer as
well,
an
extension
study on
further
nutritional
analysis
has beeu granted.Irr the
extension study
nutritionists
organized
prelimi-nary
study for further nutritional alalysis.
The
teamsstarted to study^the
guideline provided
by the Japaneseexperience."'tt
They
areresponsible
for
supervizing
the
nutritional
datacollection by interviews
conductedby well-trained field nutritionists
using special
nutri-tional
questionaire.
MedJ
IndonesFurther
dataprocessing and analysis were performed
by
electronic data
processing,
using computer
soft-wares
i.e.
standard statistical
packages
(SPSS
andSAS)
andFood Composition
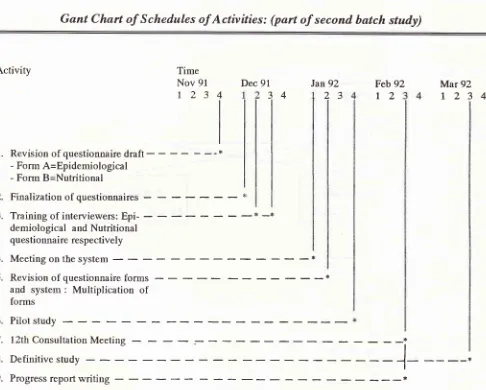
Tables.Management and
controling of
theproject.
Further
arrangements
were made
in
relation
to
thescheduling
andassignment
of
the tasks, according
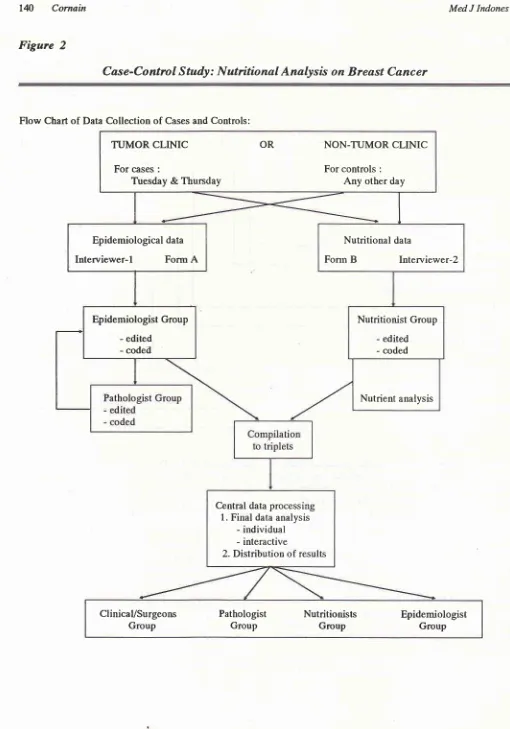
to Gannt Chart system and\ilork
Breakdown Structure or
Flow
Chart.
See
Fig. 1
&
2.
Control system
was developedfor
ensuring the completeness andreliabili-ty of
datacollection,
regular communications
amongthe team members and immediate evaluations
of
theprogress
of
the study. Materials
of
progress
reportswere
being
made
by
each
study
field
team
and
col-lected
by the coordinator. lnformal
and
formal
team meetingswere carried out
periodically.
Regular
Con-sultation
Meetings between
Japanese andIndonesian
teams
were scheduled
3times per
year,to
discuss thegrant, progress
ofthe
research, data analysis andreport
writing.
Progress reportswere
made readyafter
sum-ming
upof
eachConsultation Meeting.
Thus, diversity could
be
managed
and
controversy
could tre made constructive. Close
communicating
were also established
by
expressservice, telefax,
electronic
rnail or direct
phone
call. The
above
men-tioned model
had tremendouspower
to
instill
project
lement
team development
tocet
^rn.23'24
The-lattàr
helpedquality
control.25'26In
the
rneantime,
rearrangernent and reorganizing
oÏ
the
activities
andmethodologies were
madein
respectto
solving
problems, such as theinegular
procurement
of
cases
and controls due
to
ternporary
change
of
hospital
ward situation
and data analysis toward
micronutrient due
to
unavailable Food
Composition
Table for certain food
items.The budgetting was
arranged
according
to
'per unit
cost
system' relative to
numberof
subjects (cases pluscontrols), which
covered costsfor activities mentioned
above
plus
overhead costs.Part
of
the budget
was specially allocated
for
paperwriting
and
its publication
in
standard international
joumals
aswell"
Besides the
grant provided
by
the
Ministry of
Educa-tion
andCulture,
theGovernment of
Japan,part
of
thefunding was supported
by
the
grant from the
Vol 4, No
j,
July - September 1995Figure
7Management of Collaborative Research Project 139
Gant
Chart of
Schedules
of
Activities:
(part of
second
batch
study)
Activity
Time
Nov
91r234
Thus,
by
theeld
of
thethird
year thecollection of
datacould
becompleted
to
300 cases and 600controls
for
the
first
batch
of
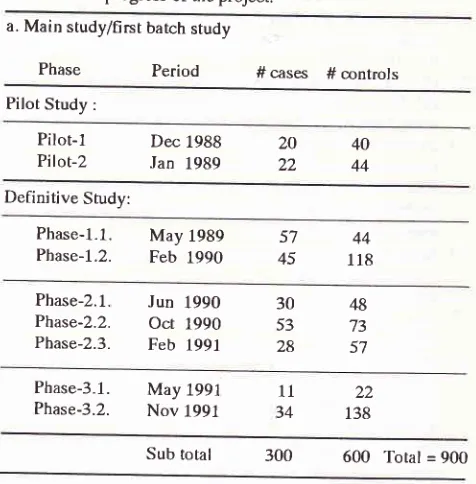
the study. This has
fulfilled
theoriginal plalning
i.e.
estirnated 75 cases.per year.
The attempts
to
perform biochemical analysis for
triglycerides,
cholesterol,
beta-carotene andretinol in
sub-samples
of
breast callcer patients were
lot
yetsuccessfully
done due
to shipment trouble to
Japan.The duplicates of
the samples aregoing
to be testedin
Jakarta andincorporated to
thepost-project planning.
Such study has been considered
important
to clarify^qhemicronutrients
related to
therisk
of
breastc
ncer."'
In
the rneantime, preliminary/pilot
study of
theuutri-tional
analysis
has beenperformed.
The results
have been usedtô
design the
definitive
study
of nutritional
analysis.Final
reports,
including
pilot
study
of the nutritional
analysis,
have been rnade and
the
results have
beendiscussed
in
a OneDay Seminar.
The
full
papers arebeing published
in thiiissue ofthejournal.
Definitive study
of
the nutritional analysis
(secondbatch
of
the study)
is in
progress.
Further
analysis
in
epidemiological, clinicopathological and nutritional
aspects arebeing
preparedfor further
publications.
As for
post-project plaruring, the
teams are interestedto
extendfurther
studiesincluding:
1)Further
analyti-cal
phaseof
theepidemiological
study
of risk
factors,
2)
Further clinicopathological study
in
early
breast cancer and breastconserving treatment,
and 3)Further
pathobiological study
i.e.
the
roles
and
interaction of
hormonal
(estrogen andprogesteron)
receptors and the oncogenes(c-erbB-Z
andp53).
Theevaluation
of suchmolecular markers
still
needs
clarifying
for
the
relationship
of their
expressions
to
the breast
cancerrisk, prognosis
and responseto
treatment.lE'28'29Dec
91Jan92
23
Feb 92t2
Mar
1234
9234
1.
Revisionofquestionnairedraft
- - --*
- Form
A=Epidemiological
- Form
B=Nutritional
Finalization of
questionnaires
-Training of interviewers:
Epi-demiological
andNutritional
questionnaire respectively
4.
Meeting
on thesystem
- - -
+Revision
of
questionnaire
forms
- - -
x'and
system
:
Multiplication of
forms
Pilot
study
l2thConsultationMeeting
-
- - --*
Definitivestudy
-
----]-Progress
report
writing
- - -*
)
J.
-* -*
6.
7.
8.
9.
l4
Cornain
Figure
2
MedJ
IndonesCase-Control Study:
Nutritional
Analysis
on
Breast Cancer
Flow
Chart
of
Data
Collection of
Cases andControls:
TUMOR CLINIC
For
cases :Ttresday
&
ThursdayOR
NON-TUMOR
CLINIC
For
controls
:Any
other
dayNutritional
dataFonn
B
Intenriewer-2
Epidemiological
datalnterviewer-l
Form
A
Nutritionist
Group
-
edited-
codedEpidemiologist
Group
- edited
-
codetlNutrient
analysisCentral
data processing1.
Final
data analysis- individual
-
interactive
2.
Distribution
of
resultsTerminating
the project
The overall picture
of
the
progress
of
collection
of
cases andcontrols is
given
in
Table 1.
Table 1. Tbe progress of the project:
a. Main study/first barch study
Phase
Period
#cases #mntrols
Pilot Study :
Sub total 300
600
Total = 900Detailed analysis has been able to perlorm after complete data
management covering 300 triplets data sets.
b. Extension study/second batch study
Phase Period #
cases
# controlsPilot Study
Pilot-1
FebI992
5A 5BPilot-2
Acknowledgments
The author is
grateful to prof.
Haruo Sugano,
CancerInstitute Hospital,
Tokyo, profs.
Kunio Aoki
andResearch
and Development Center
for
Nutrition,
Ministry
of Health,
Bogor for allowing
excellent
mul_tidisciplinary
team building andimplementation of
theproject,
This work
was supportedby
the Ministryof Education
and Culture,
Japan,
Grants
No.
01042007
and
040420131- and wa
Cancer Foundatio
part
of
Special
CaInternational
Scieapproval of
the Dean,Faculty
of Medicine, University
of
Indonesia, No.
4383 lPT02.H4.FK / E /
8g"REFERENCES
1. Cornain S, Mangunkusumo R, Nasar IM, prihartono J. Ten Pathology based
Can-:
Cancer Registry inCenter, Jakarta
Coor-3. Sarjadi. Cancer Incidence 1995-19g9
in
Semarang, In_donesia. Indonesian Cancer Society, 1990.
4. Parkin
DM.
The nature and sourcesof
cancer data from developing countries. In: Khogali M, OmaryT,
Gjorgov A,Ismail
AS,
editors.
Cancer preventionin
devel,opingcountries. Proceedings
of the
2nd UICC
Conference on Cancer Prevention, Kuwait, 19g6. Oxford: pergamon press, 1986:9-22.5. WHO and IARC. Cancer lncidences
in Five
Continents. IARC Sci Publ No.15, Vot.tII, Lyon, 1976.6. Parkin DM, Laara E, Muir CS. Estimates of the worldwide frequency
of
sixteen major cancersin
19g0. InJ
C_ancer1988;41:184-97. Pilot-1
Pilot-2 Jan Dec
1988 20
1989 22
4440 Deiinitive Study:Phase-l.1.
Phase-1.2.
May 1989
Feb 1990 4557
44
1r8
Phase-2.1. Phase-2.2. Phase-2.3.
Jun
1990Oct
1990 Feb 199130 53 28
48 73 57
Phase-3-1. Phase-3.2.
May 1991
Nov 1991
11
34
22
138
May
1992
20A
208
40A
408
Definitive Study # cases
#control-l #
control-2Phase 1.1. Sept 1992 28
A(4)
8A
lsB(4)
8B
33B
^(2)
(2)Phase 1.2. Febr 1993
164(7)
16A
2eB(7)
t6B
6A(4)
6B(4)
Notes:
A
=subjects interviewed for epidemiological data(Form A2)
B
=subjects interviewedfor
nutritional data (FormB2)
[image:7.595.42.280.156.398.2]1.42
Cornain
7. Donn AS, Muir
CS.
Breast cancer: Epidemiology and risk factors. In: KhogaliM,
OmarYT,
GjorgovA,
Ismail AS'editors.
Cancerprevention
in
developing
countries.Proceedings ofthe 2nd UICC Conference on Cancer
Preven-tion, Kuwait, 1986. Oxford: Pergamon Press, 1986:155-66. 8. Hanai
A,
FujimotoI.
Population-based cancer registry inJapan. In: Sasaki R,
Aoki
K,editors.
Epidemiology andPrevention of Cancer. Proceedings of Monbusho (Ministry
of Education, Science
&
Culture) lnternational Symposiumon C-omparative Study of Etiology & Prevention of Cancer,
Nagoya, 1989. Nagoya: The University
of
Nagoya Press,1990:199-210.
9. Weiss JW, Wysocki RK. 5-phase project management:
A
practical
planning and implementation guide'
Mas-sachusetts: Addi son-Wesley Publi shi n g Cn., 1992.
10. Michael
N,
BurtonC.
Basic project management. Singapore: Singapore Institute
o[
Management and HeinemannAsia, 1992.
11. Dyer WG. Team Building: Current Issues and New Alterna-tives. 3rd ed. New York: Addison-Wesley Publishing Co. 1995.
12. Hawkins C, Sorgi
M.
Research: How to Plan, Speak andWrite about
it.
Singapore: Narosa Publishing House,Top-pan ComTop-pany (S) Pte. Ltd.,1992.
13. Boyd NF. Epidemiology of cancer. In: TannockIF,Hill RP, editors. The basicScience of Oncology.2nd ed. NewYork:
McGraw-
Hill
Inc., 7992.-'l-22.L4. Sakamoto
G,
SuganoH,
HartmanWH.
ComparativePathologica I study of breast carcinoma among American and
Japanese women. In: McGuire WL, editors. Breast Cancer.
Nashville USA: Plenum Publishing Co., 1981.
15. Sakamoto G, Sugano H. Pathology of breast cancer: Present
and prospect in Japan. Breast Cancer Research and Treat-ment 1991;18:S81-3.
16. Japanese Breast Cancer Society. The general rules for
clini-cal
and pathological recordingof
breast Cancer. Jpn JSurgery 1989 ;19 :6 12-32.
17. Indonesian Surgical Oncology Association. Breast C-ancer
'
Management Protocol.(ln
Indonesian). Ropanasuri 1989;18:89-93.
18. McTieman A" Thomas DB, Johnson LIÇ Roseman
D.
Risk lactors for estrogen receptor-rich and estrogen resePtor-Poorbreast cancers. JNCI 1986;77 :849 -54.
MedJ
Indones19. Cavalli
PF.
Clinical researchin
advanced breast cancer:Back to the future ? Ann Oncology 199l;2:621-2.
20. Cornain S, Ohno Y. Progress Report: Japan-Indonesia Joint Study on Etiology and Clinico pathology of Breast Cancer,
Jakarta: Scbool of Medicine University of Indonesia, 1992,
Muy.
21.. Ohno
Y.
Methodology and evaluation of dietary factors inJapan. In: Mettline Cl, Aoki K, editors. Recent Progress in
Research on Nutrition and Cancer. New York: Wiley-Liss
Inc., 1990:11-20.
22. Ohno Y, Yoshida O, Oishi K, Okada, Yamate H, Schoeder
FH. Dietary p-carosene and cancer of the produk:
A
case-control study in Kyoto,Japan. CancerRes 1988;48:1331-6.
23. Breiner
'W,
GeddesM,
HastingsC.
Project leadership.Hampshire: Gower Publishing Co.Ltd., 1993.
24. Katzenbach JR, Smith DK. The Wisdom of Teams: Creating
the high Performance Organization. Boston: Harvard
Busi-ness School Press, 1993.
25. Besterfield DH. Quality control. 3'd ed. New Jersey:
Pren-tice-Hall lnc., 1990.
26. Ichikawa
K.
What is total quality control ? The Japaneseway. (LuDJ, translator). New Jersey: Prentice-Hall Inc,
1985.
27. Potischman
N,
McCulloch
CE, ByersT,
Houghton L,Nemoto
T,
Graham S etal.
Associations between breastcancer , plasma triglycerides and cholesterol. Nutr Cancer
lgg1lst2}s-r5.
28. lwaya
K,
TsudaH,
HiraideH,
TamakiK,
Tmakuma S,Fukutomi T et
al.
Nuclear p53 immunoreaction associatedwith
poor prognosisof
breast cancer. JpnJ
Cancer Resl99L1,82:835-40.
29.
Takikawa
Y,
Noguchi
M,
Kitagawa
H,
Thomas M.Immunohistochemical detection
of
p53
and c-erbB-2