[urrent
Upilates
ol
Initial
$h0rh attf, $ttohe
ilaltagenteltl
in
Primary
Care
CEE
DING
3(}(}1{
I
sEMfitAB
flASl0ilAL
SABTU,
I
APfrIL 2016
07.00
-
16.00
wtB
)
+'r* coNtttturxG IrrEDrcAL EDUcATrox
FAKULTAS KEDOKTERAN t}AIiI ILMU KESEHATAN
UNIVERSITAS MUHATIMADIYAH YOGYAGARTA
q
I
DAFTAR
ISI
Kata
Pengantar...
...i Kala5ambutan...
...r; DaJiar1si...
...vii
Clinicul Practice Guideline For Manageruent Stroke
Puticttts lrt Prinrary Health Cctre
(Phc:)
...1Prut/'. Dr. dr. Rusdi Lamsudin, Sp S(K)., M.Med.Sc Surgicul lnclic'ation For
Stroke.
...Jrlr. Endro Basulci Sp.BS(K) M.Kes
Rccent Theraplt Of Autte Stroke
/
Tia In Prime TirueAt
Priman,Cure...
...17Dr. dr.
Tri
Wahyulictti Sp.S., M.Ka,sCurrent Update Management And Rehabilitation Of Septic Shock In Printary Health
Care...
...61dr. Rizka HumardewayantiAsclie, Sp. P
D-KPTI
PenatalaksanaanShock : Therapy CairanDan
MonitoringHemodinamikTerkini...
...69 dr. Bhirowo
Yudopranoto, Sp.An-KAKV
Syok Hipovolemik Pada
Anqk.
...73Dr.nted.dr. Intan Fatah Kumara, MSc., Sp.A
dr. Nurnaningsih, SpA(K)
vii
Diagnosis Dan Terapi Syok Kardtogenik Pada Layanan Primer...
dr. Erika Maharani, Sp JP(K)
Resusitasi Cairan Pada Syok
Akibat
Trauma...dr.
Ardi
Pramono, SPAn, M.KesTatalaksana Keperawatan Pasien Shock
Di
Pelayanan Kesehatan Primer ...Sttdiman, Ns., M.Kep Panitia Pelaksana
76
79
91
95
Ct
r
r a nt U p tl a t es o { lti
t i al 5h o ck a tzd S t r o i; r: i\,|il t t it St t t t(. I i tIst {)rintriru
{lnrt
Recent
Therapy
of Acute
Stroke /
TIA
in prime
Time
at
Primary
Care
Dr.
dr.Tri
Wahyulioti Sp.S., M.Kes Departemen NeurologiFakultas Kedokteran dan llmu Kesehatan
Un iv ers it as Muhamm adiyah Yo gyak art a
Abstract
TIA, or
traruient ischemic attack,is a
',mini stroke" that occuls whena
blood clot
blocks an arteryfor
a
shorl tirne. The only difference betweena
stroke andTIA
is thatwith TIA
the
blockage
is
traruient (tenporary).
TIA
synlptoms
occtu rapidly
and
last
a
relativelyshort
tinie.Unlike
a
strokc, whena TIA
is
ovcr,
thorc'sno
permancntinjury
to
thc
brain. Thcrc'sno wily
to
tcll
if- symptornsof
astroke
will
lcadto
a
TIA
or
a major stroke. It's important tomanagc imnrcdiately
for
any
TIA
sylptonrs.
Because, lnpeoplc
wlro
havea
TIA,
the incidcnceof
subsequent strokcSaturday, April 9th 201 6
Asri Mcdical Ccntc.r of Yogyakart;r 1.7
i*
t"t:t:r'ti j: l..i tttitli::,;:'i' !iiiiiir! liiit:it. iuti! ,\lrtrl;r fvitit!tt ';'ttt t:!
i t i i::' r i i t i.t.i t' t.i t...t t r i'
is as high as
l1o
over the next7
days and 24-21)'Yt overlte
following
5 ycars.Effcctive
trcatment
of
strokecan prcvcnt
long-term
disability and save lives.
The
spccific trcatmcntsrecommended
depend
on
whethera
strokeis
causcd
bya
blood clot
obstructingthe flow
of
blood
to
the
brain (ischaemicstroke)
or
by
bleedingin
or
aroundthe
brain (haernonhagic slroke).It
is
very
irportant
to
determaine adiagnosi.s
of
an
ischaernicstroke
or
haemonfiagic sfl'okebecause
the lalsc
Ircdication
cart rnke
the
bleecling thatoccurs in haeuronhagic strokes worse.
Key word
:TIA,
stroke. acute, therapyIntroducfion
A
transient
ischaemic
attack
(TIA)
or
"mirli
stroke"
is
caused bya
temporary disruptionin
the
bloodsupply
to part of the
brain.The disruption in blood supplyresults
in
a
lack
of
oxygento
the
brain. This can
causesudden
syrptorns
similarto
those
of
a
stroke, such
asspeech and visual disturbance, and nrrnbness or weakness in
the face. arnrs and legs.However, a
TIA
does not last as longSaturday,Aprij .,'i',116
i--*.i.rt:'L! Li
:tiilNt:;ti
!tiiiili
,:iiitttl,titti
.:::,i:i:i;t: lvl.tititii,i;;lii,')iiitt ilt iit:tt':: i.-;'i',
as
a
strokc.Thc
effects often only lastlbr a
tbw minutes or hours and lirlly rcsolve within24
hou's. But, in people who havea TIA,
the incidenceof
subsequent strokeis
as high asI I o/o over the next
7
days and 24-29o/o over the following 5years.
The incidence
of
TIAs
increaseswith
age,liom
l-3
cases
per
100,000 in those yolmger than 35 years to as lrulnyas 1.500 cascs
per
100,000 in thoscolilcr
than [i5 years. Theincidence
of
TIAs
in
men
(101
cases
per
100,000 population)is
significantty higherthan
that in
wornen (70per
100,000).The incidenceof
TIAs
in
blacks
(98per 100,000 population)is
higlierthan that
in
whites(81
per 100,000 population).The causes
TIAs
Durng
a
TI{
oneof
theblood
vessels that supplyyour
brain
with
oxygen-richblood
becorres blocked.This blockageis
usually causedby
ablood
clot that has formed elsewherein
your
body
and fravelledto
the blood
vesselssryptying the brain, although
it
can alsobe
caused by piecesof
fatty
nraterialor
air
bubbles.Certain things can increaseSaturday, Aprll 9 th 207 6
L'tirr*i!
Liyeiilt:s o{ btil-ial Sliack itttd Slrol;e kltncgemtntI tr. ]) r i rri s t' tl i.itre
your
chances
of
having
a TIA,
inch.rding:srnokinghypertensiorl obese, higfu cholesterol levels,
alcohol,
atrialftrillatiorL
diabetes,over
60
years
of
age,
ras
(peopleofAsiarq African
or
Caribbeanare
alsoat
a
higlrerrisk
of
having a TIA).
Preventing
TIAs
ATIAis
oftena sigt
that
anotherone rnay
follow andyou are
at a
highrisk
of
havinga
flrll,
life-threateningstroke
in
the
near flture.Regardlessof
whetheror
not
you have hada TIA or
stroke in the past, there area
nurnberof
waysyou
can loweryour risk
of
having eitherin
the f,rture'These include Lifbstyle changes:
.
maintaining a healthy weight.
eating
a
healthy
diet-a
low-fit,
rcdtrccd salt,high-fibre
diet
is
usually recommended, includirrg plentyof fi'esh
fruit
and vegetablesexercising
rcgularly-
for
most people.at
lcast 150minutes
of
nnderate-intensity aerobinc activity, suchas
cycling
or frst
walking,
every
week
brecommended
o
Sat.r ' jay, Apn, .' L 101ir
a
a
C t
r
rt n I Ll p d a tes tti lr i t iitl Si r o tk a nd 5 i r tt it t: A,li] r t {t tt t t ii: !-t iirr [)r'iittttt u {..o; ,,
stopping
smoking-
if
you
srnoke, stopping maysignificantly reduce
your
risk
of
havinga
stroke inthe future
cutting
dorvn
on
alcohol-
you
shouldaim
not
toexceed
the
recomrrended alcohollimitsofthree
tofour rmits
a
dayfor
rnen and trvoto
tlree turitsa
dayfor wornen
In
additionto
lifestyle changes,nnst
people who have had aTIA will
need
to
take one
or
rtore
daily
medicationsindefinitety
to
help reducetheir
chancesof
havinga
stroke or another TIA.Diagnosis
Ruling
out
metabolic
or
drug-induced causesof
syrptoms
consistentwith
a
transient ischemic attack (TIA)is
important.
lnitial
assessmentis
ainred
at
excludingemergency
conditions
that can
mimic
a TIA
(eg,hypoglycemia,
seizure,
or
inh'acranial henrorrhage).A
lingerstick
blood
glucosetest
shoulclbe
perfbrmed andblood drawrr
lor a
complete blooclcourt
(CBC), coagulationSa turday, Ap ril 9rt 201.6
L..'.urrtniLirdati:soI IrtiIiitl 5!toi:kitrulStroke:Niittttlli'trl{'rrI
l*
1:lriinu rv i-'.i;rt22
studies,
and
sertrr
electrolytelevels.
Obtain
a
l2-lead electrocardiogam (ECG)with
rhythm strip, and evaluate forsynptorrntic
arrhyhmias
or
evidence
of
ischemia.Braininraging
is
recon'unendedwithin
24
hours
of
symptom onset.Brain iuragingcan identifi an
areaof
ischemiain
asn'rany as 2501, ol'patients, and
TIA
mimicsnuy
be
identifiedas
well.
Vessel irnagingcan identiff
a
stenosisor
occlusionthat may
warrant
early
intervention.Elecffoencephalography(EEG) may be indicatccl to evaluiate for seia:rc actffiy.
Signs and symptoms
The
mainsyrptoms
of a
TIAcan
be
renremberedwith the word
FAST
Face-Arms-Speech-Trne..
Face-
droppedon
one
side(not
be
ableto
srnile,nrouth or eye rnay have droPPed)
.
Atms
-
weakness or nurnbness in one arm.
Speech- shrred, garbled, not be able to talk at all.
Time-
it
is
tirneto
take care furrnediatetyif
you seeany of these signs or synPtonr's
Saturday, April 9th 2016
l-rtrrntLipilittesoi
jii.it.iitlsiio,'i..riitiiii:.i:i;t: i\v.i.;.;;i:i.i;;1i;.1;1;:.r ' rjJ: r. i . .
lnitial vital signs should includc
thefollowing:Ten:perahre,
Blood
prossrx-c,
Hcart
rate
andrhythnl
Respiratory rate and pattern, and Oxygen saturation.The
exarnincr should assessthe
paticnt's overall health andappearance,
nuking
an
assessnrclltol'
the
following: attentivcness,ability
to
interactwith thc
cxamincr, Ianguagcand memory skills, hydration statm, development.
Risk Stratilication
ScoresIn
pcople
who
have
a
TlA,
the
incidcnce o1.subsecluent stroke is as high as 1l%o over the next 7 days ancl
24-29"/,,
over
the
following
5
yeal.s.Appropriate riskstrati{icatiou utust
be
employedto
L.llsure that diagrostic andthcrapcutic
intcrventionsare
tar-gctcdto
thc
highcst-risk patients.Anulber
of
risk
stratification scolesare
availableto
assistin
llis
task,but thc
rnostwidcly
validatedis
thcABCD2 scorc.(See Table
I
below.)Saturday, Ap r ll9,s 201. 6
Asri Medical Center of Yogvakarta
23
I
pointA:
Age >60 years1 point
B
:
Blood
pressue:
Systolic>140
nrn Hg
or
diastolic >90
nrn
HgUnilateral weakness with or without speech inpairment C: Clinical features
2 points
I
point Speech inpairment withoutunilateral weakness
2 points
D:Duration >60 min
I
pointl0-59
minI
pointD:
Diabetes{'t s' r u
*
Li lt t}il
ts a { It r i f iol 5h a ck n t ul St r o k e Mn nage rnant ltzl]rim*rtl
CsraTable 1.ABCD2 Score
ln<lividurls
with
anABCD2
scoreof
6
or
7
have8% risk
of
stroke within
2
days, whereas those with ABCD2 scorc lowcr than4
havca l%
risk of strokc within days.Someof
thcsc
paticntswith
lowcr
scorcs nuyhave
non-TIA
eventsrather
than
ffue TIAs.lt
hasproposed
that this
scoring systemcan
be
used
tostratiland
to
predict
the
severityof
recurrent strokeTIA.
24
Saturday, April 9th 201 6 [image:11.462.30.448.41.574.2]L''trtr(iri
llr,ialt'qoi
ltriiiizl!,ittt,!,.irii
iiri:i:r:iv,lii:titlt)?\{:t!ii:i
Ptiiltis:t i.'il
r
Physical Examination
The goals
of
the physical examination areto
urcoverany
neurologic
deficits,
to
evaluate
for
underlyingcardiovascular
risk
frctors, and
to
seck any
potential thromboticor
embolic sourceof
the
event.Global
CNS depressionand
ainvay
or
cardiac
compromiseare
not[pically
features
of a TIA. In
filct,
the
level of
corsciousness
and
newologic
examinationfindings
areexpected to be at the patient's baseline.
Ideally,
any
neurologic deficits shouldbe
recordedwith
theaid
of
a
formal and reproducible stroke scale, suchas the National Institutes
of
Health Stroke Scale (NIHSS).A
stroke scale prompts the examiner
to
be thorough and allowsdifferent
examinemto
repeat
the
examination reliablyduring subsequent phases
of
the
evaluation.Any
neurologrcabnormalities
should
suggestthe
diagnosisof
sfroke
(or ongoing neurologic event) rather than TIA.Sa ttr rday, Ap ril9il. 201,6
26
t-' r ir r,t
i!
Li t, ii tt l " c o I I n i ti nl 5i t it tk it r td St r o k e Mn n itSc fft( t i i
ln l:trirnarv Carr
N eurologic Examination
A
ncur:logic
cxaminationis
the
forurdationof
ttr
TIA
evaluationand
should
focus
in
particular
on
theneurovascular
distribution
suggested
by the
patient'ssymptoms. Subscts
of
the
netnologic examination incfudethe
following:Cranial
nerve
testing,
Determination somatic rnotor strength, Somatic sensory testing, Speech andlanguage testing.
.Assessment
of
the
cerebellar system @esure to watch the patient walk)
For
sonratic
motortesting
test
musclereflexes
of
the
biceps, triceps, brachioradialis, patellaq andAchilles.
In
additioq
inspect posture andlook for
tremors-Tcst
the
sfrengthof
the
shoulder girdle, upper extremities,abdominal muscles,
and lower
exftemities.Test
pmovement
of
majorjoints
to
look for
spasticity, clonts,rigrdity.
Saturday, Aprii ,'Li' 2016
Cru'rtnt L[pdales ai lnit:ial Shotk
tnrl
Styr:i;t: Aikitnigjitt:rti itt I)rintnru {liit't'Stroke Scale
The
National
Institutes
of
Health
Stroke
ScaleNIHSS)
(see Table2
below) is used nrostly by stroke teamslbr
quaffirying neurologic
impairmcnt.It
enables
rapid detemrinationof
the
severityand
possible locationof
thestroke.
A
patient's score on theNlllSS
is str-ongly associatedwith
outconrc,and
it
can help
idcntdy thosc patients whoare
likely
to
benefitfrom
thrombolyic
therapyand
thosewho are
at
highe.
risk
for
developing
hemomhagiccomplications
of
tluombolytic use.TheNIHSS
is
easily usedand
focuses
on
the
following
6
nrajor
areas
of
theneurologrccxaurinationievel
of
corLsciousness,
VisLalliurction,
Motor
firnction, Sersationand
neglcct, Ccrcbcllar limctinn ancl Language.Saturday, April 9il' 2016
28
tJ.rit'rtni Littiar,'. r:{ lnifia! 5ltack
util|tyoke
Mrtnrtgtrrtnt fr.itriir;
rry{itrt
Table 2.
National Institutes
ofHealth
Stroke Scale (NTHSS)Saturday, Aprii :t* 201,6
Asri Medical Cer,;er of Yogyakarta
Category Score -Description
la
level of consciousness (LOC)0 Alert
I
Drowsy2 Stuporous
3 Coma
1b LOC qucstions
(rxrnt[
agc)0 Answers both corrcctly
I
Answcrs Icon'ectly 2 Incorrcct on
both
lc
LOC
comrrxnds (open and close eyes,grip and release nonparetic hand)
0 Obeys both con'ectly
I
Obcys Icon'ectly 2 Incorrect on
both
2 Best gaze
(follow
finge00 Normal
1 Partial gaze
palsy
2 Forced
devration
., Best visual (visuiil lields)
0 No visual
loss
I
Paftialhemianopia
[image:15.463.118.452.58.552.2]\.' ! ! !' t' ( it
i
Li p d a t t:s oi
l t r i t iai Si r a' i. ii i t,i :) i :i: i;i: it,i;i : ii!'ir? tt
1 i !it; {)t
irril-l
{-'iu't'hemianopia 3 Bilateral
hemianopia
4 Facial palsy (show tecth, raisc brorvs,
squeeze eyes shut)
0 Nornral
1 Minor 2 Partial 3 Completc
5
Motor
arm
left*
(raise90o,
hold
10seconds)
0 No drift
I
Drift2 Cannot resist
gra\{ry
3
No
effortagainst
grauly
4No
movertent
6
Motor
arm riglrt*
(raise 90o,hold
10seconds)
0
No
drift1Drift
2 Cannot resist
gravity
3 No ellbrt agairst grauty
4No
rnovement
7
Motor leg
left*
(raise
30", hold
5seconds)
0
No
driftI
Drift2 Cannot resist gravrty 3
No effot
against
graviry
Saturday, April 9th 2016
{', ts- r u
*
Li y}',
t',-'' t' " r i I ial Si r o r:k a rrl
St rt:kt: M n t tit ! t t r i( fi t ln l:trim*rq Ctrt'4No
nrovement 0 No drift
1m
2 Cannot resist
Savity
3
No
effortagainst
gavity
4No
rnovernent
B
Motor
leg
riglrt*
(raise
30o, hold
5seconds)
9
Limb
ataxia (finger-nose, heel-shin)0 Absent
I
Presentin
Ilimb
2 Present in 2
limbs
10 Sensory
$inprick
to face,arrq
leg)0 Normal
I
Partial loss2 Severe loss
0 No neglect
I
Partialneglect
2 Conplete
neglect
11 ExtinctiorVneglect
simultaneous testing)
(double
0 Normal articulation
l
Mild
to nnderatedysarthria 2 Near to
txdntelligibl
e or worse t2
Dysartkia
(speechclarity
to
'Ynarna,baseball, huckleberry,
tip-top,
fifty-fiftv')
30
Saturday, April 9th 2015l3
Best
languagex*
(name
items,descnbe pictures)
0
No
aphasiaI
Mild
tomoderate
aphasia
2 Severe
aphasia
3 Mute
Total 0-42
*
For limbs with arrputation,joint
fusion, etc, score 9 and
e4plain.
*x
For intubation or other physical barriers to speech,score
9 and exphin. Do not add 9 to the total score
Cr*-rcnt Llpd.ales o{
}rit:iitl
Sitotki*ul
St.roi;t: }vlattit!*tit:rtil:t
{}rintnrst CcrtThe NIHSS
is a
42-point scalc, rvith nrinor strokesusually being corsidered
to
resultilr
il
score lower than 5.An
NIIISS
score higherthan
l0
corrclatcswith an
g0%lkelihood
of
visual
flow
deficits
olt
angiography. yet,discretion must
be med in
assessingthe
magnitudeof
theclinical
deficit;
for
instance,if a
patient'sonly
deficit
isbeing mute,
the
NIHSS
score
will
be 3.
Additiornlly, thescale
does
not
rrcasure
sonrc delicits
associatecl withpostcrkrr circulation strokes (eg, verligo and ataxia).
Saturday, April 9tt 2016
Currant Littdatcs sl
ln)ticl
Sltock cnd Stroke Mnrvtgemant {n l}yim'trvt)art
Managernent
The
following shouldbe
done
urgentlyin
patientswith
TlA:Evaluation,
I{isk
stratification
(eg,
with
theCalifornia
or
ABCID score),
Initiationof
stroketherapy.
For
paticnts
with
a
rccent
(<l
wcck)
TIA"guidelines
reconrrrrcnda
timely
hospital
refi:nll
withhospitalizetio
n
for the following:.
Crescendo TIAs.
Duation
of symptons longer thanI
hour.
Synptorrraticinternal
carotid
stenosis greaters0%
.
Known
cardiac
source
of
embolm
(eg fibrillation).
Known hypcrcoagulable state.
Appropriate combinationof
the
Califomia scoreABCD
score (category 4)Afthough
the
symptomsof
a
TIA
resolvein a
few minutesor
hourswithoutany
specific
treatment youSaturday, April 9th 2016
Asri Medical Center of Yogyakarta
t. !:;:'t'i!i Li::1i,ii;..,:.'i !;;tii,:t .1..,1]t1 t. ti;:r' .,; t,i;, \,,i;t:::t.t.,:|1t.. :
i1i !'" it:t,'t:1y tl. ; :
nccd
trcatmcntto
h.lp
prevent anotltcr
TIA
or a
fiJl strckc happcningin
the
futule.A
TIA
is
a
waming sign thatyou arc
at
a
significantly increasedrisk
of
havinga
fi-rllstrokc
ur thc
near
futu'e,with the
higltcst riskin
the
daysand
rveeks {bllowing the attack.A strokeis
a
serious healthcondition
tlratcan
causc
pcrnunont disability
arul
canbe fatal
in sorle
cases, but appropriate treatnrcnt following aTIA can
help
to
reducc
your risk of
havingone.You
treatment
will
depend
on your
individual circunstances, such as your age and nredical history.In sonrccases, surgery may
be
neededto
r.mblock the carotid afieries(the
rrnin
blood
vesselsthat
supplythe
brair with
blood). The healthcare team can discuss treatment options with you. andtell
you about possible benefits and risks.Pharmacologic rnanagement
for
transient ischemtcattacks
(TIAs)
is
aimedat
reducingboth
short-term andlong-term
risk
of
stroke.In
view
of
the high shorl-term riskof
stroke
after
TIA,
antithnombotictherapy should
beinitiated
as
soonas
intracranial hemorrhage has been ruledout.In
view
of
the high short-termrisk
of
stroke after TIA, antitluombotictherapy should
be
initiated
as
soon
asSaturday, April 9tt, 2016
C ur r - r;t LI y ii c t i::; r t ! I n i I inl 5l t o ck u rd St r oke Nfu urtge rnent
ln Priint rrt Cara
intracranial hemonhage
has
been nrled
out.noncardioembolic
TIA,
the
following antiplatelet agentsall reasornble
frst-line
optiors forffiial therapy:
V
.
Aspirin (50-325 mg/day).
Aspirinplm
extended-release dipyridannle.
ClopidogrelStroke
prevention rnedicationtypicalty
recornnrendedcardioembolic
TIA
is as follows:.
For
patientswith
atrial
fibrillationafter
TIA,
long-term
anticoagulation
with
warfrrin international norrnalizedratio
[fNR],
2-3);325 m/day
for
those unable
to
takeanticoagulants
F
are
iefi
a
ln
acutc
myocardial
infirction
(MI)
withventricular
tlrombus,
oral
anticoagulationwarfirin
(targctlN&
2-3;
concurrcntasprin
up
to162
mg/day
for
ischemiccoronary
afterytcADl)
34
Satur,iay,,.r,pril v ir 201 6C*rran! Littti.i,stt:s af' jtr.itial
5ita*
nizl 9!ri:i:t: lrlii:it:.,::i1ii:i'i!itt
{}rint*ry {.nrr'.
In
dilated cardiomyopathy,oral
anticoagulation withwarhrin
(target INR, 2-3) or antiplatelet therapy. In
rheumatic
mitral valve
disease,
oral anticoagulation with warfarin (targetIN&
2-3)For
patientswith
TIA
dueto
50-99% stenosisof a
rrnjor intracranial afiery, thefollowing
is recommended:.
Aspirin
50-325 rcrdday rather thanwarhrin \-/
.
Maintenanceof
blood
pressurebelow
140/90mm
V
Hg and total cholesterol below 200
m{dL
t/
.
Angioplastyor
stent placenrentis
investigational andof urknown
utility
t/
Antiplatclots
Platclcts
are blood
cells
that
hclpblood
to
clot(thickcn).
lf a
blood
vesselis
damaged, platelets sticktogethcr
to
form
a
blood
clot
to
prevent
bleeding.Antiplatelet agents
inhfuit platelet
fi"rnctionby
blocking cyclooxygenaseand
subsequent aggregation. Antiplateletrnec'licincs
work
by
reducingthe
ability
of
the
platelets toSaturday, April 9tr, 2016
Cur r u
*
Li it tl a I t:s o I I r r i I ial 5l t o ck n nd St r o k e Nl {t t tit Sl tw n tln Prirnct rtl C.ara
stick
together andfbnn
clots.If
you have hada TlA, it
blikely
that youwill
bcolllred
antiplatelet rn:dication.Two
comrron
antiplateletsoffered
to
pcoplchave
had
a
TIA
arc aspirinand
clopidogrcl. Aspirinalso
somctimcsbc
takcn
with another antiplatclctcalled dipyridanrole because
this
canbe
more effectivetaking these medications separately.
The
rnain side
effects
of
antbhtelet
nredicationsindieestion
and
an increasedrisk
of
bleeding-
for
exampyou
may bleedfor
longerif
you cut
yourself, and you bruise easily.Antiplatelet Agents are :-
Aspirin. Aspirin
blocks
prostaglandin synthetaseand
this,
in
turn,
inhibits prostaglandin syitlrcsisprevents fornration
of
platelet-aggregatingA2.
Aspirin
25
rE/dipyridannle
200
ntg
:aspirin-dipyridamole therapy
has
been shown to cardiovascularevents following
TIAs.
Eachcontains
25 rrg
of
aspirin and200
mgof
Satr-rr iiay,
April';
:'20'1.6t--tii
rttrl
ilpiiittt:so
liiitiiti
!:liittrir rriti.i :\i ti)i;t.i.v,tiittit,itt;ft:r;!it; {}t intr"nt {'rtt't,
for a
daily total doseof
50
mgof
asplrin and400
mgof
dipyidamole.
Aspirin
ineversibly
inhibits
formation
of
cyclooxygcnase,
thus
prcvcnturg
Ibrmation
of
throrrboxane
N., a
platelet
agg€gator
andvasoconstrictor. Platelet inhibition lasts
for
the life
of
acell (approximately
l0
days).Dipyridanrolc
is a
platelct
adhcsion inhibitor
thatpossibly inhibits
red
blood
cell
(RBC)
uptake
of
adenosine,
itself
an
inhibitor
of
platelet
reactivity. lnaddition,
it
may
inhfoit
phosphodiesterase actMty.leading to
increased
cyclic
3,,5,-adenosinennnophosphate
within
plateles
and
lbrmation
of
thepotent platelet activator thromboxane
N..
Clopidogrel
:
Clopidogrel selectively inhibitsthe
bindingof
adenosine diphosphate(ADP)
to
its
platelet receptorand
subsequent
ADP-mediated activation
of
theglycoprotein
GPIIbAIIa
corrple4
thereby
inhfoitingplatelet aggregation.
Saturday, Ap rilgtt 201,6
{'.tirr*,-! 'ri triin{rs
ol
lrrilial Slnckntrl
Strokc Mnnit.\ement {tt l} r i i *,i t' tl l.^. i.t r'.'-
Dipyridannle
:
Dipyridannle
is
administered
toconplement
usrnl warhrin
therapy.
It
inhfoitsadhesiorl which rnay inhfoit adenosine uptake
by
RBCs'It
may
increasecyclic
3'.5'-adenosine(cAMP)
within
plateletsand
fonnationof
theplatelet
activator ttromboxane42. In
addition, it reducethe risk
of
stroke when
wed
asinstead
of
aspirin.-
Ticlopidine
:
Ticlopidine
is a
second-line antiptherapy
for
patientswho
cannot tolerate
or
dorespond
to
aspirin therapy.In
sorne circurnstances, itbe an altemative to clopidogrel Anticoagulants
Anticoagulant medicines
can
hep
to
prcventclots
by
changingthe
chemical conpositionof
the blooda
way
that prcvcnts clots.They are usually offcrcd towho
have hada
TIA ifthc
blood clot that catscd your originatedin
yoLrt' hcart.This
is
often due
lo
acalled
atrial
fibrillation,which
causesyour
heart
toinegularly.Anticoagulants agents are :
Saturday,
Apri'
rih 2016Asri Med-ica; C.-,
Jl.
t).ttirtn! Liptiitlt:s,;ti'ltriliiti Siri:;l; ituii
iiri:i:i:
i',.,iti:i,ititit,ti:iit
1)tiillt
tt,l i'_.'it:,,Warfrrin
:
Warfrrin
interfereswith
hepatic synthesisof
i,itamin K-dependent coagulation factors.
It
is
used forprophylaxis
and
treatment
of
venous
thrombosis.puknorary
embolisrrgand
thromboembolic disorders.A
side effect
of
all
anticoagulantsis
the
risk
of
bleedng causedby
the reduction in the blood's abilityto
clot. youmay need
regularblood
testswhile
taking warfarin, sodoctors can ensure your dose is not too high / low.
,
Antilrypertensives (blood pressure medication)
If
you
have highblood
pressue '(hvperlension), youwill be
offered
a
t),pe
of
medication
called
anantihypertensive
to
control
it.
This
is
became high blood pressure significantly increases yor.rrisk
of
havinga TIA
or stroke. There are lotsof
differentty;es
of
'redicine that can help control your blood prcssrrc,
incluiling:
\A/
.
thazrdc diuretics.
angiotensin-convertingev.)me (ACE)
inhibitors.
calcium channel blockers.
beta-blockersSaturday, April 9rr, 2016
40
{.|:ir r
*it
l !'/ ii rt t t:'; t 1 i t t i i ii tl Sl r tt r:k it r t d St r ttkt: NI it t t ii (('r,/{'ril{n l}rit*ti rti
iitrr
Sorne people may be offered
a
combinationol'two
or
threediffercnt rrcdications.
Paticnts
may
be
sigrrfficantlyhlpertcnsivc.
Unlessthere
is
specific conccm
for
end-organ danragcfrom
ahlpertensive emergency,
blood
pressrne shouldbe
rnanagedconseruatively
while
ischemic stroke is being ruled out.For
acute
ischemicstroke,
the
AHA
initiating antilrypefiensive therapy
only
if
blood
pressurehigher than
2201120 rnrnHg
or
if
mean arterialexceeds 130 mrn Hg. Unless there
is
a
cornorbid cardiacother condition tlrat necessitates reduction
of
blood allowingthe
patient'sblood
pressureto
autoregulate athigher level
(duringthe
acute
phase)nray
heS cerebral perfi"sion pressure.Statins
If
you
have high cholesterol,you
will be
advisedtake
a
nredicine known as a statin. Statins reduce the levelcholesterol
in
your bloodby
blocking an enrynre in thethat
produces cholesterol Statinsmay
alsohep
toSaturday, April 9th 2015
t
trt'rt nt Ll pdtttt:s rtllniiiei
Siitti l, it r r:i i!i'iii:t: i\,1,i t :'t{Jirii , r lI t t {}r. i ni ;i t.t! {l a t.,.
your
risk
of a
stroke whateveryour
cholcstcrol levelis,
soyou
llraybc
olli:rcd
a
statin evenil'yorx'
cholcstcrol level isnot
pafticularly high.Examplesof
statinsoften
offered
to peoplewho
have hada
TIA
include atorvastatin, simvastatinand rosuvastatin.
Surgcry
In
son-rc cascs,a
surgical proccdu'c callcd a carotidenda(erectomy mrly
be
recommendedalter
havinga
TIA.A
carotid
crxlarterectomyis an
opelation
that
ir-n.olvesrenmving
pafl
of
the
liningof
tlrc
carotidafiety.
plus anyblockage that has brrilt
.p
in
the artcry. The carotid arteriesdeliver
blood
to
your
brain.Whcn
htty
dcpositsbuild
upinside
thc
caroticl arteries,they
bcconrchard and
narow,nnking
it
nyorcdifficult
for
blood
to
flow
through themThis is known as atherosclerosis and
it
can lcadto TIAs
andstrokes
if
the
blood
supply
to
thc
brain
becomesdisrupted.By unblocking the carotid arteries in people whose
afieries
ate
nroderatelyor
severelyrnrowed,
a carotidendafterectomy
can
significantly reduce therisk
of
having astroke or another TIA.
Saturday, Ap r il 9 a. 201. 6
42
C.urrant Llrrdntr.s o/ lrriticl Shack nnd Stroke hLcnogemant
{n l:'rirntt r.tl Cayt
Driving
after
aTIA
Although
a TIA
shouldn't have any long-termon
your
darty
activities,
you mtst
stopimmediately.Ifyour
doctor
is
happythat you
have nndegood
recoveryand
there
are
no
lasting effectsafter
orcmonth
you can start driving again.Prognosis
With
passive reporting the earlyrisk
of
strokeTIA
is
approximately4%
at2
days, 8o/o at 30 days, andat 90
days.When
patients
with
TIA
areprospectively, lrowever,
the
incidenceof
stroke is as highl1o/o
at
7
days.Thc probabilityof
strokc
in thc
5following
a
TIA
is
rcporled
to
bc
24-290/,
lrt patientswith TIAs
or
stroke have
an
incrcascd risk coronary artery disease.Patient
EducationBefore
bcing dischargedfrom
the
hospital,who
have
been
diagnosedwith
TIA
mmt
receiveSaturday, April 9th 2015
C m' r en t L) p d a t cs
oi
Itti titl
Sh o & n nrl 5 t r ok
Nl tt n a gt r nc n thr Printcry
Cn't
instruction
to
ensurethat they
understandthe
needfor
aconplete and rapid
workrp
tl,roWh
closefollow-up
care.Also
essentialfor
patientsis
educationon
stroke symptoms,the
needto
call
enrcrgency services inrnediatelyif
any
of
these
synptorns
occur,
and
the
contact nurnber
for ernergency services (911 in the United States and Canada).Despite program
efforts
in
public educatioq
rnanypatients still
do
not
seek nredical attention after experiencingTIA
synptoms.A
2010
population-based study found that3l% of
all
patientswho
experienceda
recurrent strokewithin
90
daysof
their
frst TIA
or
minor strokehad
not sought nredical attention after theinitial
event.Public
health professionalsand
physiciansneed
todo
ff)ore, such
as
promotingand
participatingin
medical scrccningfrirs
and
public
otrtreach prograrns.In
additioq patients needto
be
educated about lifestyle nrodffication andcardiovascular risk fictors
Saturday, April 9th 2016
-44
C w' r
tnl
L I y ti * t cs r: { ln i t:isl 5h o ck uti
St r * f; e klit n n g: rn* n!{n Prirusrq
{ara
Noncardioembolic
transient
ischemic attackAntiplatelet agents,
rather
than
oral
anticoagulants,are
reconrlrcnded as initial therapy.Aspirin
50-325 mg/da1;a
combinationof
aspirin and extended-release diplridarnoh, and clopidogrelare
all
reasonable fost-lineoptiors
(classI
reconnnendation).
The AHA/ASA
guidelines state thatthe
combinationof
aspirin and clopidogrel mightbe
consideredfor
initiationwhhn
24
hoursof a
minor ischemic strokeor TIA
and lbr contirurationfor
2l
days.
However,
the
combinationaspirin and clopidogre[ when initiated days
to
years after aminor stroke
or TIA
and continued2 to 3
years, increasesthe
risk of
hemonhage relativeto
either agent alone and bnot
recomnrcnded
for
routine
long-term prevention after ischemic stroke or TIA.Cardioembolic transient
ischemic attackIn
patientswho
have atrial fibrillationin
associatbnwith
a
TIA,
long-term anticoagulationwith
warfrrin
to
aSaturday, Ap t il 9 th 20'1, 6
l'ii.i ri:rt! i-i tt!itii:g r:1" ltt.ii titi 5!r r.:r'k
l
tzri Sirtti;t: i"4ti*i7t;i:tttt:fi|)it {riutnrry {.'rit't
target
intemationalnonnalized
ratio
(lNR) of 2-3
istypically
recorrncnded.
Aspirin
325
n'dduy
isrecornnrended
for
patients
unable
to
take
oralanticoagulants.
However,
the
addition
of
clopidogrel
to aspirin therapy, conparedwith
aspirin therapy alone, mightbe reasonable.
For
most patients witha
strokeor TIA
in thesetting
of
AF,
it
is
reasonableto
initiateoral
anticoagulationwithin
14
days after
the
onsetof
neurological synptorns'Anticoagulation
can
be
delayedbeyond
14
days
in
the presence of higfu risk for hernonhagic conversion'The
2014 AHA/ASA
guidelinesalso
state
thatbridging
therapy
with
subcutaneou
low-rnolecular-weightheparin
(LMWH)
is
reasonablefor
patientswith
atrialfibrillation
who
require
tenporary
intemrption
of
oralanticoagulation but are at high risk for stroke.
In
acute
myocardialinfirction
(MI)
with
left
venfricular thrombus,oral
anticoagulationwith
warfarin (targetIN&
2-3) is reasonable.ln
dilated
cardiomyopathy,
either
oral anticoagulationwith
warfarin (target
IN&
2-3)
or antiplatelet therapy rnaybe
considered.In
rheurrntic mitralSaturday, APril 9th 201 6
46
Ct*'rtnt
Ll p$ nir.s cf' lnifkil
Sltock ntzd Str':i,:e Mitnagtrnrn! {n Frimcrry Carevahe
disease,oral
anticoagulationwith
warfrrin
(targetIN&
2-3)
is
reasonable.Antblatelet
agentswould
nornormally
be
added
to
warhrin
urless
patients experiencerecunent embolism despite
a
therapeuticINR.
The beneftof
warfrrin
aftersfoke or
TIA
in patients with sinus rhythmand
cardiomyopathy clnracteized,by
systolic dysf,mction has not been established.In
mitral
valve
prolapse, long-term
antiplatelettherapy
is
reasonable.In
mitral anrular
calcification,antiplatelet therapy
can
be
considered. Patientswith
mihal regurgitationcan
be
consideredfor
warfrrin
or
antiplatelet therapy.In
aortic valve
disease, antiphtelet therapy rnay beconsidered.
For
patientswith
mechanical prosthetic vahes,oral
anticoagulationwitlr
warfrrin
(targetIN&
2.5-3.5)
b recomnrended.For
those
who
experienceTIAs
despitetherapeutic
IN\
aspirin75-100
rrrdday can be addedto
theregimen. Patients
with
bioprostheticvahes
and no
othersource
of
thromboembollsmwho
experienceTIAs
can
becorsidered
for
oral
anticoagulationwith
warbfo.
(targetrN&
2-3).Saturday, April 9th 2016
C.wrent Llp'lutes ctl
hitinl
Slrccknnr! Strake hlrtn*gerncnt htl>rinmrtlCrrt
Intracranial
atherosclerosisThe
2014
AIWASA
guidelines statethe
followingfor
patients wittr strokeor TIA
dueto
50-99% stenosisof
annjor
intracranial artery:,./ .
Aspirin
50-325
@day,
rather than
warhrin,
isrecorrrnended
,/ .
Maintenanceof
blood
pressurebelow
140/90nm
Hg
and total
cholesterolbelow
200
mddL
isrecornrnended
.
Exffacranialor
intracranialbypass surgery
is
notreconnnended
.
Angioplastyand
stent placementare
investigationaland of unknown utility
A
randomizedtrial
has
shown
that
aggressive rnedicalrBnagement (antiphtelet
therapy
combinedwith
intensivernanagement
of
vascular
risk
fictors)
is
safer
thanpercutaneou translurninal angioplasty
and
stenting (PTAS)in
patientwith
70-99%
stenosisof
a
major
intracraniala(cry.
Enolkncnt in this trial was stopped after 451 patientsrurderwent randomization because the 30-day rate
of
strokeSaturdav, April9th 201,6
Asri Mc.j..cal Ce- .el of Yogyakarta
I
Currcnt Llpttliles of lttilinl Shock nnd Stroke Managerrrcnt
[fl Primarv Cart
or
deathwas
l4.7Yoin
the PTAS grorp
and5.8% in
themedical-management goup.
Long-Term Monitoring
Patients selected
for
outpatientcare
should have aclear follow-rp plan and
stroke
prevention initiated asdescribed, including antiplatelet
medicatbn
and
risk-rnodification Antblatclet agents
Spically
shouldinitiated
as
soon
as
intracranial bleedingis
nrled
out.noted
(see above),the
agentto
be
used varies with patient and the specific indicationThe
following
rrrcasures shouldbe
includedin
anyterm rrrcnitoring
of
TIA patients:.
Anhhyperlensivecontrol
should
be
optimizedpatients with hlpertersion
. Lipid
control
should
be
initiated,including a statin agent
.
Blood
glucose
conffol
should
be
optimizedpatients with diabetes
Saturday, April 9th 2016
Asri Medical Center of Yogyakarta
t'.rs'rtnt Llp'lntcsol {rtif irt" Slratk itnd Stroke Manugtrncnt
ltt
?rinnry Cwt
A
snroking-cessationstratery,
which
may
inchrdemedicatioq shouid be initiated
Heavy
drinkers should eliminateor
reduce alcohol consunptionOverweight patients should
be
encouragedto
loseweight
All
patients should be encouraged to exerciseRecommendations
These guidelines
cover
both
ischaemicstroke
andtrarsient ischaemic attacks
(TIAS).
Separate guidelines existor
are
being preparedfor
intracerebral haernorrhage andsubarachnoid haenronhage.
The
classesof
evidence andlevels
of
reconrnendations usedin
these guidelines are defi ned accordingto
the criteriaof
the Euopean Federationof
Neuological
SocietiesSaturday, April 9th 201 5
Asri Medical Center of Yogyakarta
o
a
a
a
Currcnt Llptd tlcs aj'
lnitkil
Sltock nnd Stroke Monogernent[n Priynsrv Care
tiG s:
iEs
PU6'=-U
S$a
E8E
, ora.E I
EH5
E.:l
E;l
t
*'88
E ; AA
F
:bE
g
U EEP EEIIo oOO c uv=
I
u TEr
i;"
c
a-E sa-E
c !EEb,
qtr: i oft!r.i!!
? e q E --E'
.ge&ro=E6E
t:;tXEE;
b;PEETEE
EEEEE,*tg.
E HEEE E
I;
- u"ic " o? E
5 S E
e*
x€
3hq=od-i-g.T E
E;
E;;
Ef;EEEXHg
raptu*=b"
EEEEEg;E
o r d tr'v hq c*o*;EiE9
fi i c o -e q o o o d c 8t p a c D s ? g E E o o EF $g
E aP
.Qo5
Eli
EgE EES .sEE E14U$t
E E EEEiE
EEE
E
E"8
E 6E
= -'Q
b a-!l?o
*En
t u;
EEg
!t! LYU
o Ell
eIdo;o
ioH fi -9o:c >to
t;Ex >r
Yoy aat
{
E
.HE
fr
3BEA
EE:;
a
$;ii
: FE i i9
r
efl
I $9
9ptre".E
qrU^-C.Y
e$h8EEE
p;:E5e:
H3€
!
E H EIEEiEflE
oBEh'E2c
EtE
EEfiE
dts,i*j..tti q E f o o E I E 8N E o r? c a fi q ( o o E o u o E
,
!
q E:
o g E a E * E o E E o tEE
f,E
gEEE
=E ipf;88
E€Eg
"€uPIr€*
$!::
ob = I
ssEh
EEEfi
E i tr il E n o q c e u -f g E T o o i! r b e E H r.l;
DSaturday, April 9th 2016
Asri Medical Center of Yogyakarta
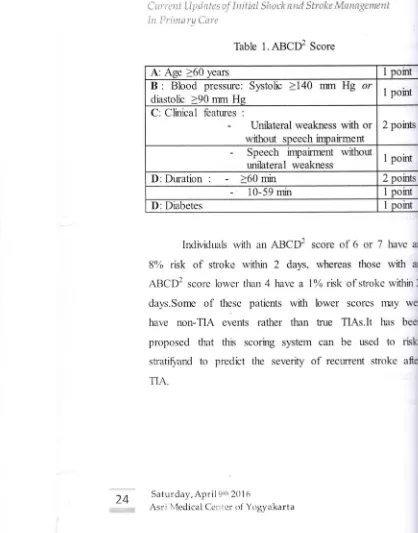
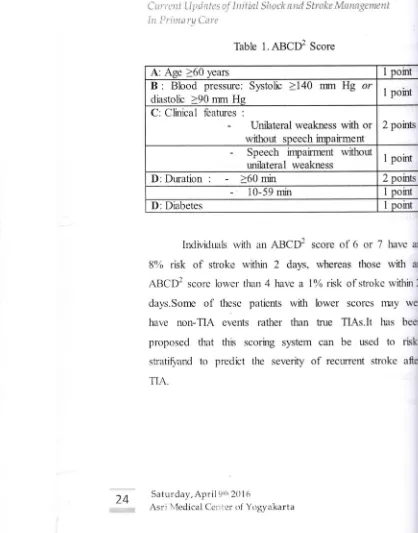
Table 9.2 De{initions {or levels of recommendation (from [583]).
o
an
(,
v\)
x-(^
ea,
:t-.jv
>
\t
^=
Level A Established as usefuTpredictive or not usefullpradictive for a diagnoslic measure or established as
effective, ineffective or harmful for a therapeutic intervention; requires at least one convincing Class I
study or at least two consistent, convincing Class ll studies
Established as usefuUpredictive or not uselu,lredictive for a diagnostic measure or established as
effective, ineffective, or harmful {or a therapeutic rntervention; requires at least one convincing Class ll
study or ovenvhelming Class lll en/idence
Established as usefu7predictive or not usefuUpredlctive for a diagnostic measure or established as
effective, ineffective or harmful for a therapeutic interventron; requires at least tr,!o Class lll studies Recommended best practice based on the axperience of the guideline development group. Usually based
on Class lV evidence indicating large clinical uncertainty, such GCP points can be useful for health workers
Level B Level C
Good Clinical Practice (6CP) points
H
7
9-.)
Ai LD
*'!) rDE o!) ts\<
hJ>
<'o
31
I'N, tD o\
ffiuli
l:r P il
[image:38.591.82.499.187.349.2]\-52
Curt'ent Llpttielcs
r:l'iirificl
S!ncktnd
Strol;e Mitnngernentln Primartt Carc
Sroke
services and stroke unitRecommendations
.
lt is recornrnended that all stroke patients should betreated in a stroke unit (Class l, Level A).
.
lt is recornmended that lrealthcare systems ensure thatacute stroke patients have access to high technology medical and surgical stroke care when required (Class lll,
Level B).
.
The developrnent of clinical networks, including telemedicine, is recommended to expand access tohigh-technology specialist stroke care (Class ll, Level B).
Diagrostic innging
Recommendations
r
ln patients rvilh suspected TIA or stroke, urgent cranial CI{Class l), or alternativety MRI (Class ll), is ncommended
(Level A).
.
lf fulRl is used, the inclurion of diffusion-weighted irnaging(DW) and T2t*veighted gradient echo sequences 1s
re(ommended (Class lt, LevelA).
'
ln patients with TlA, minor stroke, orrecovery immediate work-up, urgent
vascular imaging or MR
angiography) is ((lass l, A),
Saturday, April 9th 201.6
Ctrrcni
Ll.ttlates ojbtitid
Sltock anri Sirake Manogernt:ntlit
Prinnry
Cwt'Other Doagnosis Tests
Rerommendations
r
!n patients with acute stmke and Tl,{ early dinical evaluation, including physiological parameters and routine blood tests. is recommended (Class l, Level A)..
For all stroke and TIA patients, a sequence of blood testsis recornmended (table 9,3, table 9.5).
o lt is recornmended that all acute stroke and T[,A patientr should haw a 1Z-lead ECG, ln ddition continuous E(G
recording is recomrnended for ischaemic stroke and TIA patient: (Cla:s t, Letel A).
.
[t is recornmended that for stmke and TtA patients :een after the acute phase, 24-h Holter ECG rnonitoring should he pe#ormed when anhythmias are suspected and no other causes of stroke are found (Class l, Lerel A)..
Echocardiography ir recommended in selected patients(Class lll, Lercl B).
Satur.rlay, April 9th 2016
Curr
u*
Lllt d n t e s o f ln i t'ktl Sl t o ck n nd St r o ke Mit n t ge meutIn Primurv Care
Managenent of Vascular Rlsk
Eecprrrnendethns
' Blgcd pEsaire sfEukt hE clucfieo rEgulrry. tt ts
feromnErE€d uElt hlgh EBd Frscjfe $Euld E
nanrgEd Qlrh ilfusryE lTEdtca$rn ir6 h{r}rtrluJlred
Fnrmradog(al lhEraFy LE E{ lri drnlrE at
mnnrl ler€ls gf 14
fPdrt tillurB dlnbEtsE,ar cfrunlf, rxld
anlil?ErtEmhE m€dlatE{r E lntlclted tcts l, LRH 4.
r EIEECI EuEose stro{:lu be chB(Hl rErylarly. It b
rffirnnreDJed trlat daDetEs ghflJld be marraqed vl,tth
lfesty'e mEdltEto[ arld ltddl:UellDe.l Fhilrnafffogl{al
tner+I {ga5r lv Lerd ci. h d3e[c paenls, htgh bhsd FrEsurE lls"rE EB ,rt;lnaEd htefEl$eu {€ta55 l, Lelel {l atrnlng ior lsrg! bgril# l3offilrflml{q Flass l4 LsfEt rl.
wnere FerHe tEatrmnt stsjld lrl|lucle !n Bt. lorEngn
cofterur€ ErrlTrfle lrfilHto] or sngb&n{n rece@r
rntrJsnlrt {clars I, l-sl€l A}
r Blaod rhdc6teml shauE E ElErXEd r€gulxly. I ls
reffimtEffil$Ihet hlgh blffid {ndE5terol (E.9. tot}
l50r€tt l3.gmnsuD snoukr bE rnfi4ed ${fi $ttrqle flEdtfl(3Itrr (cless lY LEtcl q trrd a ltaIn itrla5 1.
l-fi,td Al.
. lt E rsEEmn€ndE{t tfiitclgErstG rmoxtEg bE dlsEuJralEd
trlss lll, L€t el E).
. lt E rEEomrEr{rErl fint hem,y lrse of iholEl bE
clssrraged (oE ll. LErsl E).
t R€qur phyrlcal aEt[lty E resmr€ldEd {ElEs lll,
Ls\E q.
. a EtEt l$r' h satard 5ltjt3ted f.t htgl ln liut afrd \ESFEot€s 3rd rLtr lll llre E rEmm]r€nu€{r {o& ll,
L€r€ E.
. lubJerts wlEl 3n €lalBlEd Eodf rlrralB lrr:lg are
reomnErroed to tete r urggrrt-rE[tuchg dlgt (El6 lt,
Lere E.
r Antrqrldnnt vttamh $JpplEm€BE a{e not rtrsrnrnsrlEd
{ClsE l, lrrg Al.
. HoTTEIE r€pE0Elmnt tntr#t ls nst lEtrIrnEnded iff
tne pflrrsy praEnflon of strd{E iEl6 t. tB€t A).
54
Saturday, April 9th 2016Cts'rcnt Llpilatcsof
[nitki
Slro*l*d
Strok MsvrLt4ttncntltr Prinut"rtl Crn'e
Prinnry
Prevention-
Anfithrpntbic Therapy"
Lorl-dcce arpirin is rBcsmfi?rded in r.Em€n aged 45!.aar: flr rnore wtlo re rtot Et increaged dd< for
lntrecerebrd haerylsrrh€e and who hav* good
gastrrJntectinal tdrance; ho!.,Errerr its effect is very
srnall (Class l, Lerrpl A).
.
lt is recsnmerrded that lorv-dcre aspirin rrry bersrsi&red in rnBn
fs
fte primsy prerrerxlrr of rnyoerdid hrfarction; trowwer. it does nct rpduce the riskof isdraernk 5tulte (Cks 1. terre{ A},
.
Afltidratrht EsEflts otlnr tfran aspitn am not recomnrendedfor primary shtg{<e pr*rent}rn {Chs,V, 6Cp}"
.
Asfrdrin nry be recorrrrended lor pxients withncn-vakr.rler AF who are yo.rnger than 65 yean and
frce of vrcula risk factss (Chs l, Lerrel A.
.
lhlees *wrbaiir$<ated. eitlpr aspirin or aa oralanlimaguhr.rt {nt€matimal ncrmaked ratio flf{Rl t.A-3.0} is rxonxner#Bd for patientr with non-vaha.dar AF r+ho
are aged 65-75 yean md fee af rrascuhr risk fartor,s
(Class
I
tsvel A)..
Lhles: contrairdcated, an oral antiroagul*nt tf{R 2.0-3.0}i: reromrnended far patients wifi non-rrahaJar AF wfro are agrd >75. or wtro are ya"rrger but hane risk lartors ardr al higt| bhod prer*nq [eft rrrnficular d6function.
q dabeter rrpilihJs (Clar l, t-srel A).
,
lt ic rscsmendsd that patients !v,i6 AF u*ro are unahleto receive ord anticaa$,iants shoutd be sffsrcd asphin
(flarr L Levd A).
.
lt h rxornmendcd *rat paient5 wifi AF who hatremxhmkal prosth*tic h*art vahrcs shcr.rld receive [ongrterm antiroeryrlatic* r+ith a target INB based om rtre
prosltr*i: {ype. but nd less than INR 2-3 {Clnss ll, Lor*l B}"
.
Lour<Jpse xpirin is reronrrended for patients u4thaqrnptcrnati< inp'nal ramtid art€ry (lCA) stenoris >5016
to rpdure th*ir drk of vascular e\rents (Clss 11, LorEl E).
Saturday, April 9th 201 6
56
C. urr e nt Ll trt d t l t s t: !' l i i i t ktl Sl i o
*
ri n.d St r o k c Nliut fi q t rrrc ntln Primarv Care
Secondary Prevention
Optimal rnanagement
of
vascular risk frctorsRerommendetlons
. lt is recrynmended rltat blood prrrsui€ b€ che<ked
regrlorly" Blood prerure lcniveriqg ir reronnflsfided aftei'
tte acute phase, includng in patieflts with nornral blood
prersure {Ckss t, ta/el A).
" tt i: reromrnended that blood glueos* lhould be rhe<ked reElularly. 11 ie recorrrnerded drat diabetes drould be
nranaged widr li{estyle moditi(Eti,on and individualEed
pharrmr,:l,rgieal therapy {Class l\4 CCP).
. ln patienls with type 2 diabetea who do not need insulin,
traatment witt| f,ioglitarnnE is rpcornrrerd*d after stroke
{f,ltsss lll. Lev*l B).
. statin theraty is rerorrurended in subj*ds with
nsr-cardir:*mbalic stroke (Cln55 l, Lscel Al.
. lt is r*commended that rigarette sEnohinq be drcnr:raged
(Class lll, Leirel C],
. it is rec,:nrmended that healy u*e ol alcohol be
di:couraged (Class tV. GCP).
. ftequlo,r phryncd activity b recomrnended {Claas lS GCP}.
. A diet lerw in sah ard seturated fat high in fruit and
veg€tnbles. and ri<h io fibre is re(ffnm*adsd ({lass l{
GCPi.
. Subiects with an elevated hody mass indeot are
recomnrended to ddopt a weight-reducing diet (da5s lV,
Lelsl (i.
. Antioxidant vitamin s-rpple.rnents ar* not rec(}nrn]Ended
(Class l, level A].
. Hormonp reSa<ement th*raFry i! n$t recomnr*nded for
rhe secondary p{evprnion of stroke {Cless l, Level A},
. h is recrrnrrnended that deep-clis,:nCered breathing aurh as obrtru.tive sle*p aFnoea be trentFd rrvith continuous
pr: itive airwqy Frplstre breathing {Claso tll. Laiel G(P}.
. lt i: recemrnended thgt €ndovascular cls*re of FFO b*
con*dered in p*tients with <rlptogenic stroke and high
risk PFO {llass M GCP}.
Saturday, Ap r il 9 th 20L 6
Asri Medical Center of Yogyakarta
Ctu'rent Llp'lates ai
hiticl 5ln&
itnrl Strakc Mn na*etncntilt
l>i'inrcry CnreAntithrombotic therapy
R€(ommendetlons
. lt b rc<a*rmended $al patients re<eirre antithronrb<dk
tlerapy {Class l, Loel $.
r h k reco*vnended that patienB not req.rhng
antkoaErlation shquld receirE antiplx*let therapy (Cfa* l, Lercl A)- Where possible, combined aspririn and
dipyridannle, or dopidogpd alone, should be giwn.
Ahernatimly, aspirin alooe or triffusal done rnry be u:*d
(Ctass l, Lnrel A].
. Ihe cnmbination of aspirin and <lopidogrel ir not
recomm+nded in patients with recent isfraernic strc&e, exceFt in $niipnts with specific indcations (e.9. un*able
angina or non-Q-ware Ml ff rpcenl stpntiflg); traatrEent sh*.rld be qiven for r*p to 9 months alter thp eryent Klass
l, Le\ipl A),
. tt ts re(rrmrnended that patients r*-ho harn a stroks fli antiplatelet therapy shorld be re-evduated for
pathophy:iology and risk Iirtors (Clasr I{ 6CF}.
r Oral antiroagulation {lNR 2.0-3,0} is reconrmended afler
i:<haemic atrol<e areodated with Af tClass l. Lelel A]. Oral
anticoagulation h not recomrnended in patients \.r,ith con"rorbid conditions such as falls, poor <onplian<e.
urrontrCled epileply, r gastrointesinal bleedng {Class
Itl, lelel C)" lncrea$ng age alone is not a conraindication
to oral antkoagulation {Chss l, Lelel AI
. ft is re(offan€fided that patimts nith cardoernboli< sboke
r.nrelated to AF:hou,ld reeive antico.gulaftts {lNR
2.0-3.0) if thp rhk of recunence is hiEh (Cla:s t{, LE /el C).
e lt k rxamrnendsd that aflti.oa$Jlation *mrtrd not be
u:+d after ncn-cardio+mb,o{i< isdramic stro&e, except in
tom€ spe{ific 5ltuatiom, such as aortir ath.eromas"
fusiform aneurysnrs of the basilar ortery cer,vkal artery dsaectiol't. or patent feranren crrah in lhe presence of
proven deep vein thrombo,sb (DMO or arrial septal aneurysm (Class lV GCPI
r tt is recsrilnerd€d that <omtrined low dme apirin ard
dipyridrnole *ouH be giwn if oral anticoagdation is
contdrdicated (Class lV, GCP).
Saturday, April9th 201,5
58
C ur r
tnt
Llpt d a t es o,f ln i tinl Sl rc ck t n.d S t r o k e M a n n gr: ment{n Primarv Carc
Conclusion
Pharmacologic
managenrnt
for
transient ischemicattacks
(nAs) is
ainrd at
reducingboth
short-term andlong-term
risk
of
stroke.In
view of
the higlr short-term riskof
stroke after
TIA,
antithrombotictherapy should
beinitiated
as
soonas
intracranial hennnhage has been ruled out.Saturday, April 9th 2016
Cttrr*tt
Llprllttr:s oihtitial
Slrrst"k nnd StT oke iv'lftntt4i:n{ntltr l'rinr.nty Cnrt
References
l.
Ringleb,M.G.
Bousser,G.
Ford,P.
Bath,M.
Brainin, V. Caso,A
Cervera, A.1 Chamorro, Charlotte Cordonnier, L.Csfua,
A.
Davalos,H.
-
C. Diener, J. Ferro, W. Hacke, M.Hennerici,
M.
Kaste,P.
Langhorne,K.
Lees,D.
Leys, J.Lodder,
H.
S. Markus, J.- L.
Mas, H. P. Mattle, K. Muir, B.Norrving,
V.
Obach, S. Paofucci,E.
B.
Ringelstein,P.
D.Schellinger,
J.
Sivenius,V.
Skvortsova,K.
StibrantSunnerhagen,
L.
Thomassen,D.
Toni, R.r von Kummer, N.Gunnar Wahlgren,
M. F.
Walker,J.
Wardlawm20ll
-Ischaemic stroke and transientischaemic attack
-
European Handbookof
Neurological Management: Volume 1, 2nd EditionEdted by N. E. Gilhus, M. P. Barnes and M. Brainin201 1 Publishing Ltd. ISBN: 978-l-405-18533-2
2.
WilliamJ.
Powers,MD, FAHA,
Chair; ColinP.
Derdeyn,MD, FAHA, Vice Chair;Jos6 Biller, MD, FAHA; Christopher
S. Coffey, PhD; Brian L. Hoh, MD, FAHA;Edward C. Jauch,
MD, MS, FAHA; Karen C. Johnston, MD, MSc;S. Claiborne
Johnston,
MD,
PhD,FAHA;
AlexanderA.
Khalessi, IvfD,MS,
FAHA;ChelseaS.
Kidwe[ MD,
FAHA;
James F.Meschia,
MD,
FAHA;Bruce Ovbiagele.MD,
MSc, MAS,FAHA;
Dileep
R.
Yavagal,
MD,
MBBS,
2015.AHA/ASGuidelines
for
the
Early Management offatientsSaturday, April 9th 201 6
Asri Medical Center of Yogyakarta
59
60
Cun'ent Llyrtiaics t:! )rritktl Sltotk r,"ttd StrokcMtriitgtttwnt
In l!rimurq Carc
With
Acute
Ischemic Stroke
Regarding EndovascularTreatment.
A
Guidelinefor
Healthcare Professionals Fromthe
American
Heart
Association/AmericanStrokeAssociation. Stro k e. 2015;46:000-000.
3.
Ashish Nanda,Niranjan N Singh, Robert E O'Conno, 2015-
Transient Ischemic Attack, Treatment and ManagementMedscape Medical News. Updated:Dec 01,2015
4.
[Guideline]National Institute
for
Health
andExcellence
(NICE)
Stroke
Guidelines. Availablehttp//zuidance.nic e. ore.uk/CG68/Guidance/pdf/Enslish.
Accessed: September 22, 2010.
5.
Wu CM, Mclaughlin K, Lorenzetti DL, Hill MD, MannsGhali WA. Early risk of stroke after transient ischemic
a
systematic review and meta-analysis. Arch Intern2007 Dec 10. 167 (22):2417 -22.
6.
AmarencoP,
GoldsteinLB,
SillesenH,
BenaventeZweifler RM, Callahan
A
3rd, et aL Coronary heartrisk in patients with stroke or transient ischemic attack and
known coronary heart disease: frrdings
from
thePrevention by Aggressive Reduction
in
Cholesterol(SPARCL) tr'nL S tro k e. 201041(3) :426-30.
Saturday, April 9th 2016
Asri Medical Center of Yogyakarta
Cw"rent Llp,lutes a{
lrif
kti Slratk nnd Strai:t: M*n*gtrtrcnt lit l>rinutril Crirt7.
Chandratheva A, Lasserson DS, Geraghty OC, Rothwell PM.Population-based
study
of
behavior
immediately aftertransient ischemic
attack
and
minor stroke
in
1000consecutive patients: lessons
for
public education. Stroke.2010 Jun. al (6):1 108-14.
8.
Bos MJ, vanRln
MJ, Witteman JC, HofmanA,
KoudstaalPJ,
BretelerMM.
Incidence and prognosisof
transientneurological attacks. JA M A. 2007 D ec 26. 298(24):2877-85.
9.
Giles MF, Ahers GW, Amarenco P, Arsava EM, Asimos AW,Ay H, et al. Early stroke risk and ABCD2 score performance
in
tissue-
vs
time-defned
TIA:
A
multicenter strdy.Neurology. 2011 Sep 27 . 77(13):1222-8.
10. Shcchan OC, Mcrwick A, Kelly LA, Hannon N, Marnane M,
Kync
L,
et al. Diagnostic usefulness of the ABCD2 score todistinguish transient ischemic attack
and
minor ischemicstrokc from nonccrebrovascular events: the North Dublin TIA
Study. Stroke. 2009 Nov. 40(Il):3449-54.
ll.
TsivgoulisG,
StamboulisE,
ShamraVK,
Heliopoulos I, VoumvourakisK,
TeohHL,
et
al.
Multicenter externalvalidation
of
theABCD2
scorein
triagingTIA
patients.Neurology. 2010 Apr 27 . 74(17):1351-7.
Saturday, April 9th 2016
Cur r ent LI p d a t r,s a { }r t i
titl
Sl rc ck nnd S t r o ke Mn n c gu nant{n Prirnarv Carc
12. Asimos
AW,
JohrsonAM,
Rosamond WD.evaluation of the ABCD2 score accuracy for predicting
ischemic stroke in admitted patients with transient ischemb
attack. Ann Emerg Med. 2010:201-210
13. Chandratheva
A,
GeraghtyOC,
Luengo-FernandezRothwell PM. ABCD2 score predicts severity rather than
of
early recurrent eventsafter
trarsient ischemic aStrok e. 2010 May. 4l(5):85 1-6.
14. Stead LG, Suravaram S, Bellolio MF, Enduri S, Rabinstein
Giknore RM, et al. An assessment of the incrementalvalue
the ABCD2 score in the emergency departrnent evaluation
transient ischemic atlack.
Ann
EmergMed.
2011 J 57( I ):46-51.15. Fothergill
A,
Christiarson TJ, Brown RD Jr, RabinsteinValidation and refinement of the ABCD2 score: a popula
based analys its. S n"o k e . 2009 Aug. 40(8):2669 -7 3.
16. Amarenco P, Labreuche J, Lavall6e PC, Meseguer E,
L,
Slaoui T, et al. Does ABCD2 score below 4 allowtime
to
evaluate patients witha
transient ischemic attacStroke. 2009 Sep. 40(9):3091-5.
17. Merwick
A,
Albers GW, Amarenco P, Arsava EM, Ay CalvetD,
et al. Addition of brain and carotid imaging toSaturday, April 9t'. 2016
Asri Medical Center of Yogyakarta
t...-. i ; r r * *
i
L i ;L, i, t l t:s tti
i t t.i t i a i 5h ts i :k t t ui 5 i t' o k i: ;\'4 i;i n ttt
t r *: ri tJti iltint*r:1
{.trt
ABCD'zscoretoidentifypaticntsatearlyriskofstrokeafter transient ischaemic attack: a multicentre observational study.
Lancet Neur

![Table 9.2 De{initions {or levels of recommendation (from [583]).](https://thumb-ap.123doks.com/thumbv2/123dok/733620.573629/38.591.82.499.187.349/table-initions-levels-recommendation.webp)

![Table 9.2 De{initions {or levels of recommendation (from [583]).](https://thumb-ap.123doks.com/thumbv2/123dok/733620.573629/88.591.82.499.187.349/table-initions-levels-recommendation.webp)
