FEMALE, HYPOALBUMINEMIA, AND PROLONGED
PROTHROMBIN TIME ASSOCIATED WITH QUALITY OF LIFE IN
CHRONIC HEPATITIS B
Gontar Alamsyah Siregar, Sahat Halim, Ricky Rivalino Sitepu, Muhammad Syakur Division of Gastroentero-Hepatology, Department of Internal Medicine, Faculty of Medicine,
University of Sumatera Utara/ Adam Malik Hospital, Medan, Indonesia
Abstract
Objectives. The purpose of this study was determine the health related quality of life (HRQOL) in chronic hepatitis B and also aimed to assess factors (baseline information of demographics and laboratory parameters) related with HRQOL in CHB patients.
Methods. Quality of life was prospectively investigated in February – July 2013. Simple random sampling was done to get 60 CHB patients, with or without cirrhosis. Diagnosis of chronic HBV infection was based on the presence of hepatitis B surface antigen for more than six months, elevated serum alanine aminotransferase levels, with or without HBV DNA as detected. The chronic liver disease questionnaire (CLDQ) was applied to measure the HRQOL. Complete blood count, prothrombin time (PT) with international normalized ratio (INR), alanine and aspartate aminotransferase, alkaline phosphatase, γ-glutamyl transferase, total bilirubin, albumin, blood urea nitrogen, and serum creatinine were recorded. SPSS for Windows version 22.0 was used for statistical analysis with 95% confidence intervals, analyzed using independent sample ttest and stepwise linear regression.
Results. Abdomen symptoms, fatigue, systemic symptoms, activity, emotional function, worry, and summary scores of the quality of life were significantly decreased in cirrhosis as compared to patients without cirrhosis (p<0.05). Gender, albumin, prothrombin time were found to be significant factors associated with CLDQ score in patients with CHB.
Conclusions. Liver cirrhosis has a higher negative impact on the quality of life than CHB. Female gender, hypoalbuminemia, and prolonged prothrombin time were factors associated with low HRQOL in CHB patients.
Keywords. Chronic Hepatitis B; Quality of Life; Cirrhosis
Tujuan. Untuk mengetahui kualitas hidup pasien hepatitis B kronik serta mengetahui faktor-faktor demografik dan laboratorium yang berhubungan dengan kualitas hidup pasien hepatitis B kronik.
Metode. Penelitian deskriptif analitik terhadap pasien hepatitis B kronik dari Februari – Juli 2013. Dilakukan Simple Random Sampling untuk mendapatkan 60 pasien hepatitis B kronik dengan atau tanpa sirosis. Diagnosis infeksi hepatitis Hepatitis B kronik berdasarkan adanya HBsAg lebih dari 6 bulan, peningkatan serum alanine aminotransferase, dengan atau tanpa HBV DNA yang terdeteksi. Kualitas hidup pasien ditentukan dengan menggunakan Chronic Liver Disease Questionnaire (CLDQ). Dilakukan pendataan hasil darah rutin, massa protrombin, alanine dan aspartate aminotransferase, alkaline phosphatase, γ-glutamyl transferase, bilirubin total, albumin, blood urea nitrogen, dan kreatinin. SPSS versi 22.0 digunakan untuk analisis statistik dengan tingkat kepercayaan 95%, dengan uji independent t test dan stepwise linear regression.
Hasil. Gejala abdomen, capek, gejala sistemik, aktivitas, fungsi emosional, khawatir, dan skor total CLDQ secara signifikan lebih rendah pada pasien sirosis dibandingkan tanpa sirosis (p<0,05). Jenis kelamin, albumin, dan massa protrombin merupakan faktor signifikan yang berhubungan dengan skor kualitas hidup pada pasien hepatitis B kronik.
Kesimpulan. Sirosis hepatis memiliki dampak negatif yang signifikan terhadap kualitas hidup pasien hepatitis B kronik. Jenis kelamin perempuan, hipoalbuminemia, dan massa protrombin yang memanjang berhubungan dengan rendahnya kualitas hidup pasien hepatitis B kronik.
Kata kunci. Hepatitis B Kronik, Kualitas hidup, Sirosis
Introduction
Hepatitis B virus (HBV) is the most common infection in the world. Chronic hepatitis B (CHB) infects approximately 400 million people worldwide and causes 1 million deaths annually of liver disease. 1 HBV is the leading worldwide cause of liver disease, liver death, and liver morbidity. 2 Chronic hepatitis is a disabling condition that leads to impairment of life quality.
Health related quality of life (HRQOL) is a subjective multidimensional concept which includes functional status, emotional and social wellbeing as well as general health. In 1948, WHO defined health as not only absence of illness, but also complete physical, emotional and social welfare.
3
4
parameters, particularly in chronic disease in which mortality is not an immediate concern, because it also considers a patient’s functional health and well-being. 5
CHB is a common disease that causes significant morbidity and mortality, but there is little information on HRQOL in patients with CHB infection especially in Indonesia. Therefore, the general aim of this study was determine the HRQOL in CHB patients and also aimed to assess factors (baseline information of demographics and laboratory parameters) related with HRQOL.
Methods
Patient Selection
Quality of life was prospectively investigated at the Adam Malik Hospital and Permata Bunda Hospital, Medan, Indonesia in February – July 2013. Simple random sampling was done to get 60 CHB patients, with or without cirrhosis. Inclusion criteria were inpatients and outpatients with CHB, with or without liver cirrhosis, age >18 years. Patients with other chronic active medical diseases (such as congestive heart failure, chronic obstructive pulmonary disease), psychiatric conditions, malignancy, liver transplantation and those unable to communicate or who declined to participate were excluded. The diagnosis of chronic HBV infection was based on the presence of hepatitis B surface antigen for more than six months, elevated serum alanine aminotransferase levels, with or without HBV DNA as detected by the hybridization method. The study received ethics approval from the Ethic Board of University of Sumatera Utara, and all participants gave written informed consent.
Data Collection
At admission, each patient gave his or her informed consent. HRQOL was assessed by using CLDQ questionnaire. The baseline information of demographics and laboratory parameters such as complete blood count, prothrombin time (PT) with international normalized ratio (INR), alanine and aspartate aminotransferase, alkaline phosphatase, γ -glutamyl transferase, total bilirubin, albumin, blood urea nitrogen, and serum creatinine were recorded.
HRQOL Survey
emotional function (EF), and worry (WO). Scores for each question were ranked from 1 (the worst quality of life - “All of the time”) to 7 (the best quality of life - “None of the time”), for to the period of 2 weeks ago. Higher score on the questionnaire is indicative of minimum symptoms and lower score indicates poorer symptoms. The disease-specific CLDQ was more sensitive and addressed some important HRQOL domains (e.g. worry) specifically associated with this disease. 6
Statistical Methods
All data were analyzed with SPSS for Windows version 22.0. Categorical data were described as number and continuous data as mean ±SD, which were analyzed using independent sample t test. Stepwise linear regression analysis was performed to study the influence of independent variables on domains of CLDQ while controlling the effect of other variables, in which the dependent variables were domains of CLDQ; independents were age, gender, educational level, and laboratory parameters. A p<0.05 was considered as statistically significant.
Results
Demographic of Respondents
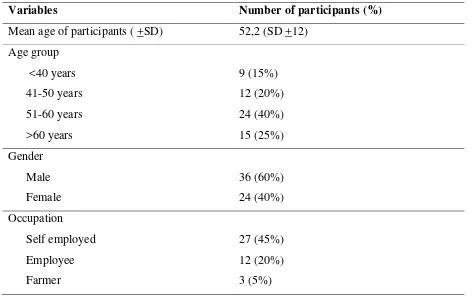
Table 1. Demographic characteristrics of participants with chronic hepatitis B
Variables Number of participants (%)
Housewife Retired
15 (25%) 3 (5%) Education status
Primary Secondary
Higher secondary and above
6 (10%) 13 (21,67%) 41 (68,33%)
Total 60 (100%)
Table one showed demographic data of respondents. There were 60 subjects, consisted of 36 males (60%) and 24 females (40%). Mean age was 52.2 + 12 (SD) years old. The highest number of age group was from the age group of 51-60. The majority of subject`s employment status was self-employed (45%) and housewife (25%). The majority of the subjects’s education level is high school or higher (68.33%).
Quality of Life in Chronic Hepatitis B Patients
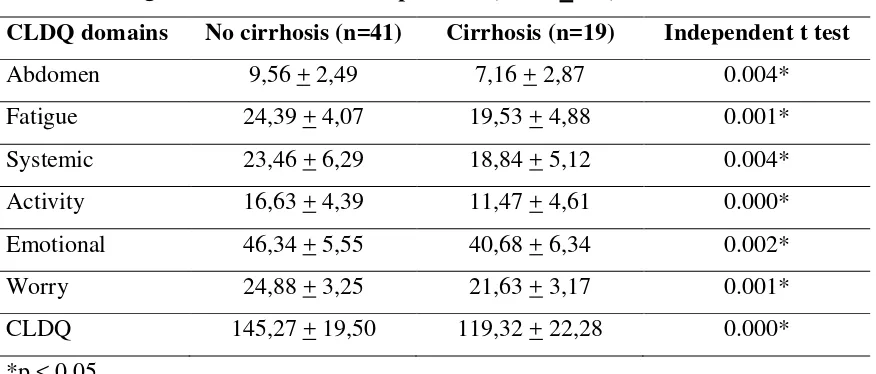
Table 2 . HRQOL scores in chronic hepatitis B (mean + SD)
CLDQ domains No cirrhosis (n=41) Cirrhosis (n=19) Independent t test
Abdomen 9,56 + 2,49 7,16 + 2,87 0.004*
Fatigue 24,39 + 4,07 19,53 + 4,88 0.001*
Systemic 23,46 + 6,29 18,84 + 5,12 0.004*
Activity 16,63 + 4,39 11,47 + 4,61 0.000*
Emotional 46,34 + 5,55 40,68 + 6,34 0.002*
Worry 24,88 + 3,25 21,63 + 3,17 0.001*
CLDQ 145,27 + 19,50 119,32 + 22,28 0.000*
*p < 0.05
Table 2 showed scores of CLDQ between CHB patients with and without cirrhosis. There were 41 CHB patients without cirrhosis and 19 patients with cirrhosis. Lower CLDQ score indicates poorer symptoms. Statistical analysis showed significantly worse abdomen symptoms, fatigue, systemic symptoms, activity, emotional function, worry, and total CLDQ in patients with cirrhosis in comparison to patients without cirrhosis (p<0.05).
Factor determining HRQOL
Item CLDQ and unstandardized coefficients (n=41)
AS FA SS AC EF WO CLDQ
Constant 6.000 9.350 11.431 9.219 37.262 21.419 94.376
Age — — — — — — —
Gender — — — — -9.134 -3.476 -13.230
Education — — — — — — —
Hemoglobin — 1.200 — — — — —
WBC — — — — — — —
Platelet — — — — — — —
TBIL — — — — — — —
Albumin 5.099 7.484 12.153 7.323 5.493 4.907 46.197
PT — — — -0.394 — — -1.811
AST — — — — — — —
ALT — — — — — — —
GGT — — — — — — —
ALP — — — — — — —
BUN — — — — — — —
Creatinine — — — — — — —
R square 0.614 0.580 0.874 0.849 0.461 0.531 0.765 WBC: white blood cell, TBIL: total bilirubin, PT: prothrombin time, AST: aspartate aminotransferase, ALT: alanine aminotransferase, GGT: γ-glutamyl transferase, ALP: alkaline phosphatase, BUN: blood urea nitrogen, AS: abdomen symptoms, FA: fatigue , SS: systemic symptoms, AC: activity, EF: emotional function, WO: worry, CLDQ: chronic liver disease questionnaire. Only data with p<0.05 were expressed as values of beta-coefficients. “—”: p>0.05.
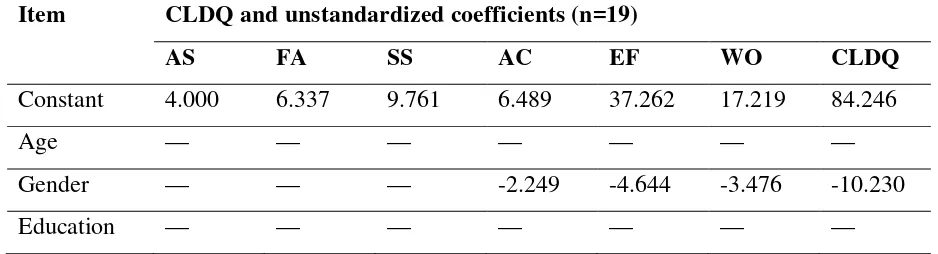
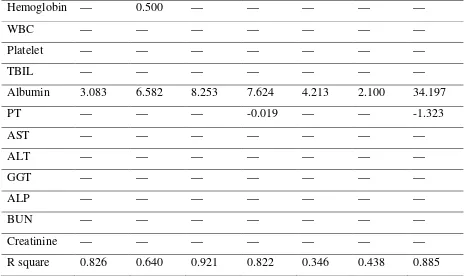
Table 4. Factors determining CLDQ score in chronic hepatitis B patients with cirrhosis
Item CLDQ and unstandardized coefficients (n=19)
AS FA SS AC EF WO CLDQ
Constant 4.000 6.337 9.761 6.489 37.262 17.219 84.246
Age — — — — — — —
Gender — — — -2.249 -4.644 -3.476 -10.230
Hemoglobin — 0.500 — — — — —
WBC — — — — — — —
Platelet — — — — — — —
TBIL — — — — — — —
Albumin 3.083 6.582 8.253 7.624 4.213 2.100 34.197
PT — — — -0.019 — — -1.323
AST — — — — — — —
ALT — — — — — — —
GGT — — — — — — —
ALP — — — — — — —
BUN — — — — — — —
Creatinine — — — — — — —
R square 0.826 0.640 0.921 0.822 0.346 0.438 0.885 WBC: white blood cell, TBIL: total bilirubin, PT: prothrombin time, AST: aspartate aminotransferase, ALT: alanine aminotransferase, GGT: γ-glutamyl transferase, ALP: alkaline phosphatase, BUN: blood urea nitrogen, AS: abdomen symptoms, FA: fatigue , SS: systemic symptoms, AC: activity, EF: emotional function, WO: worry, CLDQ: chronic liver disease questionnaire. Only data with p<0.05 were expressed as values of beta-coefficients. “—”: p>0.05.
Table 3 showed the results of stepwise linear regression analysis of different demographic and laboratory parameters on CLCQ scores in chronic hepatitis B patients without cirrhosis. Table 4 showed the result of stepwise linear regression analysis in chronic hepatitis B patients with cirrhosis. On multivariable linear regression, gender, albumin, prothrombin time were found to be significant factors associated with CLDQ score in CHB patients with or without cirrhosis, and also hemoglobin associated with fatigue domain.
Discussion
HRQOL has become a vitally important aspect in clinical practice. Quality of life is a subjective indicator for evaluations in the physiology, psychology and social dimensions which is widely applied in clinical and health service management. 8
Mean age of CHB patients in this study was 52.2 + 12 (SD) years old. which is considered a productive age group. In addition, the highest number of age group was from the age group of 51-60. This result is in accordance with the results from the previous studies such as that by Lam TP which reported the mean age of CHB patients was 50.4 + 12.3 (SD) years old and the study by Gao R, et al., which reported a mean age of 53.8 + 13.4 (SD) years old.
Research regarding HRQOL is scarce in the world and especially from Indonesia.
[9,10]
Majority of the subjects in this study was male (60 %). This result is in accordance with the previous studies which also suggested more male subjects than females.
Our data found that abdomen symptoms, fatigue, systemic symptoms, activity, emotional functiom, worry, and total scores of the quality of life were significantly decreased in cirrhosis as compared to patients with less severe liver disease (without cirrhosis). Patients with liver cirrhosis suffer from complications, which will reduce their HRQOL. Those who have developed complications such as cirrhosis have many distressful symptoms including pain, fatigue, loss of appetite, abdominal distension, etc which cause emotional function and anxiety worsen that will reduce HRQOL. This result is in accordance with the results from the previous studies. Gao R, et al found that increasing severity of chronic liver disease was associated with a decrease on HRQOL.
4,9,10
10
Svirtlih N, et al showed significantly lower mental and physical total numeric scores in patients with cirrhosis in comparison to patients without cirrhosis. 11 Lam TP reported the presence of advanced complications such as cirrhosis was the most significant negative determinant of HRQOL in patients with CHB infection. [9] Bondini S, et al examining the impact of liver cirrhosis found that the presence of cirrhosis was associated with lower HRQOL scores.
Results in this study have shown that CLDQ score is not significantly different among different age groups. However, it remains unclear whether any association between aging and HQROL. Other studies reported that older age was associated with lower HRQOL in patients with chronic liver disease,
12
[10,13-15]
but another study found insignificant or positive effect on HRQOL.
Females with or without cirrhosis have lower HRQOL scores than males, as shown in other studies.
12,16,17
13-16
on their health. Females tend to be more likely to worry about their illness and they have lower HRQOL scores.
Our study has shown that low Hb in patients with or without cirrhosis had affected the fatigue domain. Low Hb in chronic hepatitis B infection is multifactorial; chronic disease, poor nutritional intake because of diet restriction imposed on such patients by community as well by physicians, hypersplenism and history of gastrointestinal bleeding in cirrhosis patients. 4
This study found an association between serum albumin and prothrombin time with HRQOL. Albumin and prothrombin time are classified as marker of severity of liver disease. Albumin and prothrombin time are associated with HRQOL as suggested by CLDQ score therefore HRQOL can be improved if these factors are taken care of on time. Low albumin usually indicates poor nutritional status and associated with low CLDQ score by impairing the all domains of CLDQ by usually causing ascites. This result is in accordance with the results from the previous studies such as that by Les I, et al and Kondo Y, et al found an association between HRQOL and serum albumin.
Low hemoglobin (anemia) may lead to symptoms like tiredness and fatigue in general condition which depend upon severity of anemia.
18,19
Prolonged prothrombin time had negative effect on HRQOL and activity domain. Using another instrument to evaluate quality of life, Gao et al showed prolonged prothrombin time had negative effect on HRQOL because patients with poor prothrombin function reduced their ability on physical, social, and mental domains.
Liver biomarkers, such as AST, ALT, ALP, GGT was not found to have any significant association with HRQOL, though it is an important clinical markers to assess the severity of liver and determine indication for treatment and often used as a guide to anti-viral treatment.
10
9,12
Conclusion
We conclude that significantly lower HRQOL in patients with cirrhosis in comparison to patients without cirrhosis. Female gender, hypoalbuminemia, and prolonged prothrombin time were important factors reducing HRQOL.
Acknowledgements
The authors thanks Khaerani and Sulasmi for their help in data collection.
1. Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J Viral Hepatol 2004;11:97-107.
2. Lavanchy D. Worldwide epidemiology of HBV infection, disease burden, and vaccine prevention. J Clin Virol 2005;34(Suppl 1):S1-S3.
3. Heidarzadeh A, Yousefi-Mashhour M, Mansour-Ghanaei F, et al. Quality of Life in Chronic Hepatitis B and C Patients. Hepat Mon 2007; 7(2): 67-72.
4. Parkash O, Iqbal R, Jafri F, Azam I, Jafri W. Frequency of poor quality of life and predictors of health related quality of life in cirrhosis at a tertiary care hospital Pakistan. BMC Res Notes 2012,5:446-53.
5. Ong SC, Mak B, Aung MO, Li SC, Lim SG. Health-Related Quality of Life in Chronic Hepatitis B Patients. Hepatol 2008;47(4):1108-17.
6. Younossi ZM, Guyatt G, Kiwi M, Boparai N, King D. Development of a disease specific questionnaire to measure health related quality of life in patients with chronic liver disease. Gut 1999; 45: 295-300
7. Levy AR, Kowdley KV, Iloeje U, et al. The impact of chronic hepatitis B on quality of life: a multinational study of utilities from infected and uninfected persons. Value Health 2008;11:527-38.
8. Chao J, Song L, Zhang H, et al. Effects of comprehensive intervention on health-related quality of life in patients with chronic hepatitis B in China. BMC Health Serv Res 2013,13:386-94.
9. Lam TP. Health-related quality of life of Chinese patients with chronic hepatitis B infection [Thesis]. Hongkong: University of Hongkong, 2010. p. 176-223
10. Gao R, Gao F, Li G, Hao JY. Health-Related Quality of Life in Chinese Patients with Chronic Liver Disease. Gastroenterol Res Pract 2012; 516140:1-7.
11. Svirtlih N, Pavic S, Terzic D, et al. Reduced Quality of Life in Patients with Chronic Viral Liver. Disease as Assessed by SF12 Questionnaire. J Gastrointestin Liver Dis 2008; 17( 4), 405-9.
12. Bondini S, Kallman J, Dan A, et al. Health-related quality of life in patients with chronic hepatitis B. Liver Int 2007;27:1119-25.
14. Sobhonslidsuk A, Silpakit C, Kongsakon R, Satitpornkul P, Sripetch C, Khanthavit A. Factors influencing health-related quality of life in chronic liver disease. World J Gastroenterol 2006;12:7786-91.
15. Afendy A, Kallman JB, Stepanova M, et al. Predictors of health-related quality of life in patients with chronic liver disease. Aliment Pharmacol Ther 2009; 30: 469-76.
16. Dan AA, Kallman JB, Srivastava R, Younossi Z, Kim A, Younossi ZM. Impact of chronic liver disease and cirrhosis on health utilities using SF-6D and the health utility index. Liver Transpl 2008;14:321-6.
17. Sumskiene J, Sumskas L, Petrauskas D, Kupcinskas L. Disease specific health-related quality of life and its determinants in liver cirrhosis patients in Lithuania. World J Gastroenterol 2006;12:7792-7.
18. Les I, Doval E, Flavia M, et al: Quality of life in cirrhosis is related to potentially treatable factors. Eur J Gastroenterol Hepatol 2010, 22(2):221–7.