FINDING AIRON DEFICIENCY ANEMIA (IDA)AT
YOUNG WOMEN WITH OVERWEIGTH OR
OBESITY
AmelyaAugusthina Ayusari
1, Shofura Azizah
2,Lilik Wijayanti
1,Dono Indarto
1,
YulianaHeri suselo
1, Yusuf ari Mashuri
1, Yunia Hastami
1, Dwi Rahayu
11
Lecterur at SebelasMaret University, Faculty of Medicine
2Student at SebelasMaret University, Faculty of Medicine
[email protected]
Abstract
Background
: Young women can suffer from anemia due to monthly menstruation and by
having many activities without adequate iron-filled nutrition. Otherproblems found on them
are overweight and obesity. The data show that one with overweight or obesity can lead to
iron deficiency anemia (IDA) along with increasingproinflammatory cytokines, which will
cause the transcription of hepcidin. The increaseof hepcidin transcription will inhibit the
absorption of iron from the intestine into the circulation, inhibiting spending iron reserves
into circulation, and inhibitingthe release of iron recycled from splenic macrophages. This
can cause IDA. The purpose of this study was to obtain the proportion of iron deficiency
anemia in overweight or obese young women.
Methods
: The design of this study was cross sectional using purposive sampling. The
subjects of this study were the student from fiveselected Senior high schools inBoyolali,
Central Java, Indonesia. The determination of IDAis done by using hemoglobin and indexes
of erythrocytes.
Results
: This study was the follow-upof the previous study, which was conducted to 14
obese and/or overweightyoung women withanemia From 14 subjects, there wasone subject
suffered from other anemia and 13 subjects with IDA (using index erythrocytes examination).
Their mean of MCV was 72.68±4.29fl, MCH was 23.08±2.63pg, and MCHC was 35.21±0.65
%.
Conclusions
: From this study, almost all overweight or obeseyoung women with anemia
were indicated as IDA (92.8%).
Keywords:
Iron Deficiency Anemia (IDA), young women, overweight and obesity
Presenting Author’s biograph
1.
Backgrounds
Health problems faced by adolescents are anemia and malnutrition (underweight, overweight and obesity) (5). The prevalence of anemia, especially in young women (13-18 years) is about 22.7 percent. While the prevalence of obesityin Indonesian adolescents at the age of 16-18 years is about 7.3 percent, which consists of 5.7 percent being fatand 1.6 percent of being obese. This number increased from the year 2007,reaching1.4 percent(3).
Young women usually suffer from anemia due to menstruation for about 3-7 days in each month, which decreases about 30 ml of blood per day. These conditions can lead to anemia especially foryoung women who have many activities and are not supported by adequate intake of iron nutrition. In addition, they are in puberty phase that need more iron nutrition for growth and increased blood volume. Iron needs are related to body weight and weight gain will increase the body's need for iron (Arisman, 2010). On the other hand, obesity can increase the risk of iron deficiency anemia, this occurs because obesity can increase proinflammatory cytokines such as interleukin 6 (IL-6), CRP (C-Reactive Protein), and leptin, which will cause transcription of hepcidin. The increaseof hepcidin transcription will inhibit the absorption of iron from the intestine into the circulation, inhibit spending iron reserves into circulation, and inhibit the release of iron recycled from splenic macrophages (1,6,8). The purpose of this study was to obtain the proportion of iron deficiency anemia in overweight or obeseyoung women.
2.
Methods
The design of this study was observational analytic, “cross-sectional,” using purposive sampling. The subjects of this study were the students from five selectedSenior high schools inBoyolali, Central Java, Indonesia. Theywere SMAN 1 Ngemplak, SMAN 1 Banyudono, SMAN 1 Ampel, SMA 3 Boyolali. The determination of IDA is conducted by using hemoglobin and indexes of erythrocytes at clinical laboratory of Banyubening Hospital, Boyolali. The method of hemoglobin harvesting was
cyanmethhemoglobin (cut off 12 mg/dl). Then IDA is measured by looking for microcytic
hypochromic anemia using indexes of erythrocytes (Cut off Mean Corpuscular Volume (MCV) = 80-100 fl, Mean Corpuscular Hemoglobin (MCH) = 26-34 pg, Mean Corpuscular Hemoglobin Concentration (MCHC) = 31-37%) (10)
3.
Results
This study was done to continuetheprevious study, which was conducted to 14 young women withanemia from obese and/or overweight40 girls (12).
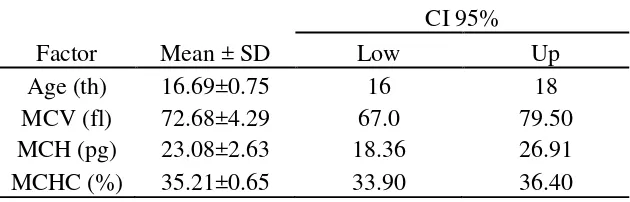
[image:2.595.135.450.664.765.2]From 14 subjects with anemia, we determinedthem using index erythrocytes examination (MCV<80fl, MCH< 26 pg and or MCHC < 31%), there wasone subject suffered from other caused anemia and 13 subjects with IDA.There were 13 young women with overweight or obese that had IDA (92.8%). The mean of MCV was 72.68±4.29fl.The mean of MCH was 23.08±2.63pg. The mean of MCHC was 35.21±0.65 %. They came from Ampel(1 subject), Boyolali(1 subject), Banyudono(4 subjects), Ngemplak(7 subjects).
Table 1. The characteristics of subjects with IDA
Factor
Mean ± SD
CI 95%
Low
Up
Age (th)
16.69±0.75
16
18
MCV (fl)
72.68±4.29
67.0
79.50
MCH (pg)
23.08±2.63
18.36
26.91
Figures 1. The Proportion of 13 subjects with ADB per each school
4.
Discussion
Iron is a very important element. It functions to distribute the bound oxygen from the lungs to the tissues, energy production, and cellular growth and proliferation (13). Iron can be found in hemoglobin or myoglobin. Approximately 25% of iron in our body is stored as ferritin, which are found in cells and circulates in the blood. Adult male has about 1000 mg of iron reserves, which would be sufficient to sustain the consumption of iron for threeyears, and women store approximately 3000 mg that is enough for sixmonths. When one reducesiron intake, iron reserves can be depleted, causing a decrease in hemoglobin levels in the blood, a condition called iron depletion. If iron reserves are no longer available, it would disrupt the system and lead to iron deficiency erythropoiesis (2,14).
Every day,humans consume approximately 10-20 mg of iron and only about 10% canbe absorbed (1-2 mg / h). Iron is absorbed in the duodenum and jejunum which will then be used by the bone marrow for erythropoiesis. In addition to absorption, iron is needed when the body loses large amounts of blood, such as in pregnancy, menstruation, and other bleeding (13).
Transport of iron is carried out by the body iron called transferrin.Transferrin is a glycoprotein, which will bind two atoms of iron and carry it from place absorbed into tissues which need the iron. Of the 75 percent absorption of iron, will be bound proteins such as hemoglobin that will serve as the transport of oxygen. About 10-20% is stored as ferritin iron so that a balance will be maintained (13).
Anemia is defined as a condition where a decline in mass amounts of erythrocyte (red cell mass) that it cannot fulfill its function to carry oxygen in sufficient quantities to peripheral tissues (decreased oxygen carrying capacity), anemic condition is indicated by a decrease in hemoglobin (9). Cut-off point anemia differentiatesaccording to age and sex; women of 15-49 years old suffer from anemia when Hb<12.0 g / dL. Anemia is a condition caused by the decreased levels of hemoglobin or red cell count. The most common cause of anemia is due to iron deficiency, but there are also other causes such as nutritional deficiency (folate, vitamin B, and vitamin A), acute and chronic inflammation, parasitic infections, and congenital diseases or acquired that disrupt the formation of hemoglobin, erythrocyte production, and survival of erythrocytes (9,10).
IDA is triggeredfrom an imbalance between the intake of iron, iron reserves, and loss of iron, which causes inadequateamount of iron in the erythrocytes formation. According to Gibson (11), there are
BOYOLALI, 1
NGEMPLAK, 7 BANYUDONO, 4
a. Iron depletion, characterized by a reduction in reserves of iron in the liver, which is characterized by lower levels of serum ferritin. At this stage, hemoglobin levels are within normal limits.
b. Iron-deficient erythropoesis, characterized by endless reserves of iron. This stage is often called “iron deficiency without anemia.” At this stage, the supply of iron to erythrocytes is disrupted due to reduced transferrin saturation. At this stage, the hemoglobin begins to show a decline, total iron binding capacity (Total Iron Binding Capacity / TIBC) increases, and increased serum transferrin receptor.
c. Iron deficiency anemia, characterized by endless fall of reserves of iron and steel in circulation, and the occurrence of hypochromic microcytic anemia. Hemoglobin levels fall due to the unavailability of iron to the bone marrow.
This study was done to continuetheprevious study, which was conducted to 14 young women withanemia from obese and/or overweight 40 girls (12). There wasone subject suffered from other anemia and 13 subjects suffered from IDA (using index erythrocytes examination). The mean of MCV was 72.68±4.29fl.The mean of MCH was 23.08±2.63pg. The mean of MCHC was 35.21±0.65 % (shown in Picture 1 and Table 1).
The results are consistent with the research conducted by Aerbeli et al. and Kapil and Sareen (1,7),which showed the relationship between obesity and anemia. This research was also supported by Cepeda-Lopez et al.’s studiesconducted in Mexico (4). Children and women of Mexico with obesity is one of the signs of decreasing levels of iron as an early sign of anemia. Therefore, obesity can increase the risk of iron deficiency anemia.
In addition to the fact that obesity can increase proinflammatory cytokines such as interleukin 6 (IL-6), CRP (C-Reactive Protein), leptin will cause the transcription of hepcidin. The increase ofhepcidin transcription may cause Hepsidintoinhibit the absorption of iron from the intestine into the circulation, inhibit spending iron reserves into circulation, and inhibit the release of iron recycled from splenic macrophages (1,6,8). Hepcidin concentrations in the circulation are controlled by various compounds involved in iron metabolism including through BMP-Smad pathway, transferrin receptor complex or STAT3 signaling (6,15). Special BMP-Smad signaling cell, increased iron stores in the liver and spleen will enable the growth factor interacts with the receptor BMP6 and BMP1 or BMP2 in the membrane of hepatocytes with the presence of co-receptor neogenin and hemojuvelin. Furthermore, ligand binding to its receptor activates Smad 1, 5 and 8 to join the Smad 4, which is then translocated into the nucleus to bind to the hepcidin response element (6)
5.
Conclusion
From this study, it can be concluded that almost all young women with overweight or obese
that had anemia; and they were indicated as IDA (92.8%)
Acknowledgements
Thanks to The Headmasters and deputy of student field at five schools ; SMAN 1 Ngemplak, SMAN 1 Banyudono, SMAN 1 Ampel, SMA 3 Boyolali, Banyubening Hospital, Human Proteomics Research groups, Risbiniptekdok 2015, and Medical faculty of SebelasMaret University.
References and citations
[1] I. Aerbeli, RF Hurrel, MB Zimmermann. Overweight children have higher circulating hepcidin concentrations and lower iron status but have dietary iron intakes and bioavailability comparable with normal weight children. International Journal of Obesity, 33: 1111–1117. 2009.
[2] Arisman. Buku Ajar Ilmu Gizi :Gizi dalam Daur Kehidupan. Penerbit Buku Kedokteran EGC. Jakarta. 2010.
[4] AC Cepeda-Lopez, SJM Osendarp, A. Melse-Boonstra, I. Aerbeli, F. Gonzales-Salazar, E. Feskens, S. Villalpando, et al. Sharply higher rates of iron deficiency in obese Mexican women and children are predicted by obesity-related inflammation rather than by differences in dietary iron intake. The American Journal of Clinical Nutrition, 93: 975-983. 2011.
[5] M. Dhamayanti. Overview Health Problems and Services. idai.or.id/public-articles/seputar-kesehatan-anak/overview-adolescent-health-problems-and-services.html .2013– DiaksesJuni 2015.
[6] T. Ganz. Systemic iron homeostasis. Physiological Review, 92: 1721–1741. 2013.
[7] U. Kapil, N. Sareen. Prevalence of anemia amongst overweight and obese children in NCT of Delhi. Indian Journal of Community Health, 26 (3): 295-297. 2014.
[8] E. Nemeth. Anti-hepcidin therapy for iron- restricted anemias. Blood, 122(17): 2929–2931. 2013.
[9] IM Bakta. Pendekatan Terhadap Pasien Anemia. Dalam: Sudoyo AW, Setiyohadi B, Alwi I, Simadibrata M, Setiati S (eds). Buku ajar ilmu penyakit dalam jilid II. Jakarta: Pusat Penerbitan Departemen Ilmu Penyakit Dalam FKUI, pp: 1109. 2009.
[10] WHO .Iron Deficiency Anaemia Assessment, Prevention, and Control A guide for programme managers. World Health Organization. 2011.
www.who.int/nutrition/publications/micronutrients/anaemia_iron_deficiency/WHO_NHD_01.3 /en/ - DiaksesJuni 2015
[11] R. Gibson. Principles of NutritionalAssesment. Oxford: Blackwell ScienceCetke 1 Edisi 2. 2005.
[12] S. Azizah. Pengaruh obesitas terhadap kadar hemoglobin pada remaja perempuan. Skripsi ; FK Universitas Sebelas Maret. 2015.
[13] CDC. Normal Iron Absorption and Storage. Center for Disease Control and Prevention. 2006.
www.cdc.gov/ncbddd/hemochromatosis/training/pathophysiology/iron_cycle_popup.htm - DiaksesJuni 2015
[14] UCSF. Hemoglobin and Functions of Iron. University of California San Fransisco. 2009.
www.ucsfhealth.org/education/hemoglobin_and_functions_of_iron/ - DiaksesJuni 2015
[15]
F. D’Alessio, MW Hentze, MU Muckenthaler. The hemochromatosis proteins HFE, TfR2, and