The Efficacy of Artesunate Monotherapy Compared
to Quinine-Azithromycin Combination for Treatment of Uncomplicated
Falciparum Malaria in Children
Beby Syofiani, Ayodhia P. Pasaribu, Sisca Silvana, Munar Lubis, Syahril Pasaribu, Chairuddin P. Lubis
Child Health Department, Medical Faculty, University Sumatera Utara/ H. Adam Malik Hospital Medan
Abstract: Department of Health, Republic of Indonesia had changed the standard treatment of falciparum malaria into artesunate-amodiaquine combination since the end of 2004. We need to find alternative drug if this combination drug is not available. This study was aimed to compare the efficacy of artesunate monotherapy with quinine-azithromycin combination, as a treatment of uncomplicated falciparum malaria in children. A randomized open label clinical trial was conducted on July to August 2007 at Mandailing Natal, Sumatera Utara Province, in 5 to 18 years old children with positive P. falciparum from the peripheral blood smear. Group I received artesunate monotherapy orally and group II received quinine combined with azithromycin orally. Parasitemia was counted on day 0, 2, 7, and 28. The cure rate was 100% and no recrudescence for both group on day 2, 7, and 28 (P=0,001). Headache, vomiting, and tinnitus adverse event was found in 14, 7 and 4 children in group II (P=0,0001; 0,027; 0,039) respectively. Both of drugs can be used as alternative treatment for uncomplicated falciparum malaria in children, but combination of quinine-azithromycin have more serious adverse reactions than artesunate monotherapy.
Keywords: artesunate, quinine-azithromycin, falciparum malaria, parasitemia
Abstrak: Departemen Kesehatan Republik Indonesia melakukan perubahan standar pengobatan malaria falciparum dengan menggunakan gabungan artesunate-amodiakuin sejak akhir tahun 2004. Pada kondisi dimana obat kombinasi ini tidak tersedia maka perlu dicari obat alternatif yang lain. Penelitian ini bertujuan untuk membandingkan efikasi monoterapi artesunate dengan gabungan kinin-azithromycin sebagai pengobatan malaria falsiparum tanpa komplikasi pada anak. Suatu penelitian uji klinis acak terbuka yang dilakukan sejak bulan Juli hingga Agustus 2007 di Kabupaten Mandailing Natal, Propinsi Sumatera Utara, pada anak usia 5 sampai 18 tahun yang positif P. falciparum pada apusan darah tepi. Kelompok I mendapat monoterapi artesunate per oral dan kelompok II mendapat kinin digabung dengan pemberian azithromycin per oral. Parasitemia dihitung pada hari 0, 2, 7, dan 28. Pada kedua kelompok didapatkan angka kesembuhan 100% dan tidak ditemukan adanya rekrudensi pada hari ke-2, 7 dan 28 (P = 0,001). Pada kelompok II ditemukan adanya efek samping sakit kepala, muntah, dan tinnitus sebanyak 14, 7 dan 4 anak (P = 0,0001; 0,027; 0,039) secara berurutan. Kedua obat ini dapat digunakan sebagai terapi pilihan untuk pengobatan malaria falciparum tanpa komplikasi pada anak, namun gabungan kinin-azithromycin memiliki efek samping yang lebih tinggi dibandingkan kelompok monoterapi artesunate.
Kata kunci: artesunate, kinin-azithromycin, falciparum malaria, parasitemia
INTRODUCTION
Malaria is the major cause of mortality and morbidity in the tropical and subtropical
areas of the world.1,2
An estimated 300 to 500 million persons suffer from malaria every year and more than 1 million die every year.2
malarial deaths occur in infants and young children.3
In Indonesia, malaria is found in every island with different degree of endemicity and can be transmitted in 1800 meters above sea level. There are 15 million cases of malaria with 38000 deaths every year and it is estimated that 35% of Indonesian people live in malarial transmission risk area.4
Drug resistance is important to be considered. Malarial death is increased, it is probably cause by the drug resistance. Plasmodium falciparum has been resistant to some kinds of malarial drug except artemisinin derivate.1
Study on some places in Indonesia showed high resistance of chloroquine, about 75% to 95% in Irian Jaya and the study in Mandailing Natal Sumatera Utara Province showed resistance of chloroquine was about 32% and resistance of fansidar was about 29%.5
Since the end of 2004, Department of Health, Republic of Indonesia changed the standard of falciparum malarial treatment, which followed the programme of WHO that changes chloroquine with artemisinin combination therapy by combining artesunate-amodiaquine as first line drugs.6
In side of artesunate-amodiaquine combination, there is also other choices that can be used as alternative treatment of falciparum malaria, one of them is artesunate monotherapy.7
Combination antimalarial therapy, usually consisting of a rapid acting, short half-life antimalarial and more slowly acting agent with a longer half-life, has been advocated for the treatment of P. falciparum malaria. The macrolide antibiotics demonstrate modest antimalarial activity and, moreover, are safe in children and pregnant women. Azithromycin, the most potent macrolide antimalarial with a long half-life (68 hours), demonstrates synergism with quinine against P. falciparum in vitro.8
In this study, we compared the efficacy of artesunate monotherapy with quinine-azithromycin combination as alternative treatment for uncomplicated falciparum malaria.
METHODS
A randomized open label clinical trial was conducted on July to August 2007 at district of Mandailing Natal, Sumatera Utara Province. The subjects were recruited from all
5 to 18 years old students suspected with malaria. If P. falciparum was found, the child was included in the study. After inform consent was taken, anamnesis and physical examination were performed, then pheriperal blood smear was taken. Exclusion criteria were severe malaria, unable to participate until the end of study and irregularly or refused to take the medicine.
Eligible sample was randomized with simple random sampling method in to two groups: group I received artesunate monotherapy with dosage 4 mg/kgbw orally in day 1 then 2 mg/kgbw orally for next 6 days and group II received quinine orally for 7 days with dosage 10 mg/kgbw/3 doses for 4 days continued with 5 mg/kgbw/3 dose for 3 days combined with azithromycin orally for 3 days with dosage 10 mg/kgbw. All anti malarial drugs were taken after meal. Repeat physical examination and pheriperal blood smear were performed on day 2, 7 and 28. Parasite was count in 200 leucocytes. Patient was defined as cured if there is no parasite and no recrudescence in 28 days of observation. Antropometric measurement was performed: body weight was measured with weight meter MIC (sensitifity 0,05 kg) and height with stadiometer MIC (sensitifity 0,1 cm). Nutritional status was calculated with standard antropometric technic based on CDC NCHS-WHO.
Data was analyzed with SPSS for WINDOWS 14 (SPSS Inc, Chicago). Wilcoxon signed rank test was used to analyze the data before and after therapy. Characteristic data and side effect was analyzed using x2
. P < 0,05 was determined as significant. The study was approved by ethical committee of University of Sumatera Utara and informed consent was taken from the parents.
RESULTS
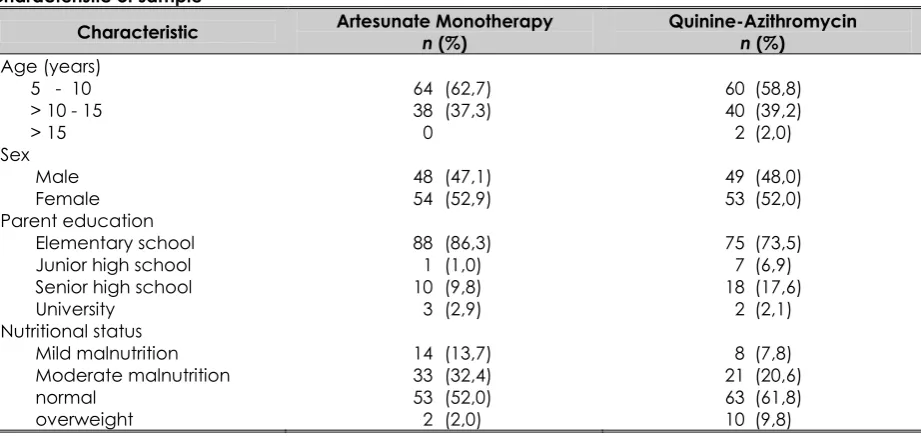
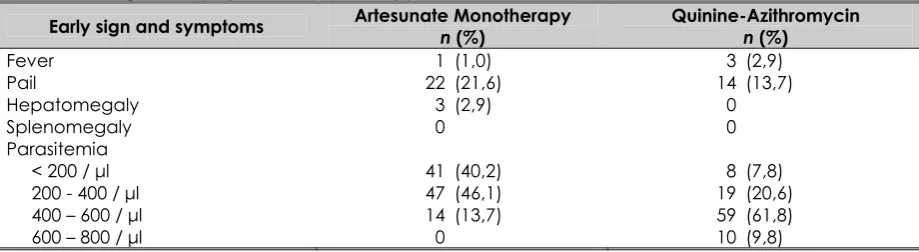
Distribution and characteristic of sample were similar in both groups (Table 1). In the early of study, physical examination was performed to evaluate fever, pale, hepatomegaly, splenomegaly and parasitemia in both groups. Hepatomegaly was found only in 3 children (3%) in group I and splenomegaly was not found in both groups (Table 2).
After therapy, side effect was evaluated in both groups (Table 3). There were
significant different of side effect in both groups, in quinine-azithromycin combination group, there were 14 children (14,6%) suffer from headache, 7 children (7,3%) vomit and 4 children (4,2%) tinnitus.
In 28 days observation, there were significant effect on parasitemia on day 2, in wich the parasitemia became negative. While in day-7 and 28, parasitemia were still negative (Table 4).
Study participant (n=204)
Artesunate Monotherapy (n=102)
Quinine-Azithromycin (n=102)
Participate until the end of study and
observed for 28 days (n=99) and observed for 28 days (Participate until the end of study n=96) 3 children lost follow up 6 children drop out :
- 3 taking during irregularly - 3 lost follow up
Figure 1. CONSORT algorithm
Table 1.
Characteristic of sample
Characteristic Artesunate Monotherapy n (%)
Quinine-Azithromycin n (%)
Age (years) 5 - 10 > 10 - 15 > 15 Sex Male Female Parent education Elementary school Junior high school Senior high school University
Nutritional status Mild malnutrition Moderate malnutrition normal
overweight
64 (62,7)
38 (37,3)
0
48 (47,1)
54 (52,9)
88 (86,3)
1 (1,0)
10 (9,8)
3 (2,9)
14 (13,7)
33 (32,4)
53 (52,0)
2 (2,0)
60 (58,8)
40 (39,2)
2 (2,0)
49 (48,0)
53 (52,0)
75 (73,5)
7 (6,9)
18 (17,6)
2 (2,1)
8 (7,8)
21 (20,6)
63 (61,8)
Table 2.
Evaluation of sign and symptoms before therapy
Early sign and symptoms Artesunate Monotherapy n (%)
Side effect of therapy
Side effect Artesunate Monotherapy n (%)
Parasitemia on day-2, 7 and 28
Peripheral blood smear
D0 D2 D7 D28
Artesunate Monotherapy
Positive 102 (100%) 0 0 0
Negative 0 99 (100%) 99 (100%) 99 (100%)
Quinine-Azithromycin
Positive 102 (100%) 0 0 0
Negative 0 99 (100%) 96 (100%) 96 (100%)
Result of Wilcoxon signed rank test on D0 and D2: P = 0,0001
DISCUSSION
Malarial treatment is based on the species of the Plasmodium, severity and drug availability.9
Chloroquine resistance is the main reason of changing the standart therapy guidelines for malaria falciparum with no complication. To provide maximal control of malaria, the medication given must be effective, has rapid onset, well tolerable and cheap (easy to get). Artemisinin-based combination (ACT) are the standart therapy regimen for malaria falciparum in many areas of the world including the south east asia region.10
ACT are the drug of choice because of the high level of efficacy, low incidence of recrudescence and potentially decreasing resistancy.11
Until now, there was not any report about resistancy of this regimen.14,12
WHO recommended the use of artemisinin and its derivate to cure uncomplicated malaria falciparum. Artemisinin and its derivate was firstly found, tested and marketed in China where this drug could decreasing duration of fever and diminishing parasitemia faster.9
In certain condition where combination of artesunate-amodiaquine were not available or if one patient does not tolerate well with these combination, we could give artemisinin monotherapy especially artesunate.10
There has not been any report of 5 days. When use as monotherapy for a short period of time, for example 3 to 5 days, the decreasement of parasitemia in the blood are only about 50%.9
several days.13
A study in Gabon which use artesunate (4 mg/kgbw/day) for 3 days for uncomplicated malaria falciparum found parasitological cure rate sebesar 90% on 14th
day, but on the 28th
day decreasing to 62%.7
Meanwhile, on study in Africa, reported 100% parasitological cure rate on day 14, 95% on day 28 and 85% on day 42 with artesunate therapy for 7 days.14
A study shown that artesunate monotherapy for 7 days for adult and children with bw > 5 kg have 92% cure level on day 28.15
Studies in Thailand and China found low cure level (20% to 54%) with artesunate monotherapy for 3 days.16,17
Other studies using artesunate monotherapy for 5 days in Gabon found 90% cure level.18
Consequently, since 2000, WHO and the International Artemisinin Study Group have recommended that uncomplicated P. falciparum malaria be treated with artesunate either in combination with another effective blood schizontocide or alone for seven days to prevent recrudescence and to delay the selection of resistant strains.14
But eventually, these 7 days artesunate monotherapy is associated with obedience of patient to consumpt the drug.10
In our study we found 100% cure level in 7 days artesunate monotherapy group and found no recrudescence on 28th
days follow up. Parasitemia are still negative which means there were no recrudescence on this group. It was reported that the number of recrudescence are associated with high level of parasitemia during early treatment.14
No recrudescence founded on these study probably because the low parasitemia level during early examination (<1000 parasites).
Prospective clinical studies of more than 10.000 patients, and post-marketing surveillance of over 4.600 patients in Thailand has not shown any serious drug-related adverse reactions.9
In our study we found vomiting in 1 patient as an adverse reaction and there were no other symptoms of adverse reaction.
Quinine are malarial drug which achieve maximal concentration in plasma 1-3 hours after given with approximately 11 hours of half time. This drug is being metabolized in liver and there were no toxicity for long periode usage.19
Quinine effectivities has been
recognized for more than 350 years ago, it is avalaible everywhere and not expensive but has serious adverse reactions and in many countries not being use alone because there been many cases of resistancy.20
For children with uncomplicated malaria, WHO recommended using oral quinine with dose 8 mg/kgbw/divided in 3 doses for 7 days.21
Azithromycin can not be use alone becuse its slow onset.22
In 1995, daily azithromycin showed an efficacy of 83% in preventing P. falciparum malaria in highly immune adult males in western Kenya.23
We combined oral quinine with dosage of 10 mg/kgbw/3 doses for 4 days and continued for 3 days with dosage of 5 mg/kgbw/3 doses for 3 days with oral azithromycin for 3 days with dosage of 10 mg/kgbw for uncomplicated falciparum malaria in children.
Quinine (30 mg/kgbw/3 doses) and azithromycin (1 g/day) for 3 days in adult are effective for resistant falciparum malaria and being tolerate better than combination of quinine-doxycycline for 7 days.22
Combination of quinine-azithromycin has rapid ability to decreasing parasitemia, where azithromycin with its long half time able to diminishing the parasites left.24
In our treatment, we found 100% cure level with combination of quinine-azithromycin, and found there were no recrudescence on the 28 days follow up.
After using azithromycin for 4 weeks, we found pruritus, erythema and rash as adverse reactions in 0,67% of cases.25
More often adverse reactions for combination of quinine-azithromycin are kinkonisme and ECG changing (prolonged QT interval).24
Our study found that significance differences of adverse reaction from therapy of quinine-azithromycin combination with artesunate monotherapy, which were tinnitus in 4 cases (P = 0,039), headache in 14 cases (P = 0,0001), nausea and vomiting in 7 cases (P = 0,027).
REFERENCES
1. Daily JP. Malaria. In: Gershon AA, Hotez PJ, Katz SL, editor. Krugman’s infectious diseases of children. 11th
ed. Philadelphia: Mosby; 2004. p. 337-52
2. South East-Asia Regional Office. Regional guidelines on the management of severe falciparum malaria in level I hospitals. WHO. New Delhi; 2004. p. 1-32
3. Krause PJ. Malaria (Plasmodium). In: Behrman ER, Kliegman MR, Jonson BH, editor. Nelson textbook of pediatrics. 17th
ed. Philadelphia: Saunders, 2004. p. 1139-43
4. Soedarmo SS, Garna H, Hadinegoro SR, Satari HI. Malaria. In: Buku ajar infeksi & pediatric tropis. 2nd
ed. Jakarta: Ikatan Dokter Anak Indonesia; 2008. p.408-37 5. Azlin E, Batubara I, Dalimunthe W,
Siregar C, Lubis B, Lubis M, et al. The effectiveness of chloroquine compared to fansidar in treating falciparum malaria. Pediatr Indones. 2004; 44:17-20
6. Gebrak malaria. Pedoman tatalaksana kasus malaria di Indonesia. Departemen Kesehatan RI; 2005. p. 1-16
7. Borrmann S, Adegnika AA, Missinou MA, Binder RK, Issifou S, Schindler A, et al. Short-course artesunate treatment of uncomplicated plasmodium falciparum malaria in Gabon. Antimicrob Agents Chemother. 2003; 47:901-4
8. Miller RS, Wongsrichanalai C, Buathong N, McDaniel P, Walsh DS, Knirsch C, et al. Effective treatment of uncomplicated plasmodium falciparum malaria with azithromycin-quinine combinations: A randomized, dose-ranging study. Am J Trop Med Hyg. 2006; 74(3):401-6
9. WHO. The use of antimalarial drugs. Report of an informal consultation. Geneva: WHO; 2001
10. Giao PT, Binh TQ, Kager PA, Long HP, Thang NV, Nam NV, et al. Artemisinin for treatment of uncomplicated falciparum malaria: is there a place for monotherapy?. Am J Trop Med Hyg. 2001; 65(6):690-5
11. Mutabingwa TK. Artemisinin-based combination therapies (ACTs): Best hope for malaria treatment but inaccessible to the needy!. Acta Trop. 2005; 95(3):305-15
12. Adjuik M, Agnamey P, Babiker A, Baptista J, Borrmann S, Brasseur P et al. Artesunate combinations for treatment of malaria: meta-analysis. Lancet. 2004; 363:9-17
13. Kofoed PE, Puolsen A, Co F, Hedegaard K, Aaby P, Rombo L. No benefits from combining chloroquine with artesunate for three days for treatment of Plasmodium falciparum in Guinea-Bissau. Trans R Soc Trop Med Hyg. 2003; 97(4):429-33
14. Menard D, Matsika-Claquin MD, Djalle D, Yapou F, Manirakiza A, Dolmazon V, et al. Association of failures of seven-day courses of artesunate in a non-immune population in Bangui, Central African Republic with decreased sensitivity of plasmodium falciparum. Am J Trop Med Hyg. 2005; 73(3):616-21
15. Price R, Van VG, Nosten F, Luxemburger C, Brockman A, Phaipun L, et al. Artesunate versus artemether for the treatment of recrudescent multidrug-resistant falciparum. Am J Trop Med Hyg. 1998; 59(6):883-8
16. Bunnag D, Viravan C, Looareesuwan S, Karbwang J, Harinasuta T. Clinical trial of artesunate and artemether on multidrug resistant falciparum malaria in Thailand. A preliminary report. Southeast Asian J Trop Med Public Health. 1991; 22(3):380-5
17. Li, G.Q, XB Guo, LC Fu, HX Jian, XH Wang. Clinical trial of artemisinin and its derivatives in the treatment of malaria in China. Trans R Soc Trop Med Hyg. 1994; 88(Suppl.1):S5-S6
18. Schwarz NG, Oyakhirome S, Potschke M, Glaser B, Klouwenberg PK, Altun H. 5-day nonobserved artesunate monotherapy for treating uncomplicated falciparum
19. Pukrittayakamee S, Wanwimolruk S, Stepniewska K, Jantra A, Huyakorn S, Looareesuwan S, et al. Quinine pharmacokinetic-pharmacodynamic
relationships in uncomplicated falciparum malaria. Antimicrob Agents Chemother. 2003; 47(11):3458-63
20. Kremsner PG, Krishna S. Antimalarial combinations. Lancet. 2004; 364(9430):285-94
21. Le JM, Jullien V, Tetanye E, Tran A, Rey E, Treluyer JM, et al. Quinine pharmacokinetics and pharmacodynamics in children with malaria caused by plasmodium falciparum. Antimicrob Agents Chemother. 2005; 49(9):3658-62 22. Barennes H, Nagot N, Valea I,
KoussoubeT, Ouedraogo A, Sanou T. A randomized trial of amodiaquine and artesunate alone and in combination for the treatment of uncomplicated falciparum malaria in children from Burkina Faso. Trop Med Int Health. 2004; 9:438-44
23. Heppner DG, Walsh D, Uthaimongkol N, Tang DB, Tulyayon S, Permpanich B, et al. Randomized, controlled, double-blind trial of daily oral azithromycin in adults for the prophylaxis of plasmodium vivax malaria in Western Thailand. Am J Trop Med Hyg. 2005; 73(5):842-9
24. Noedl H, Krudsood S, Chalermratana K, Silachamroon U, Leowattana S, Fukuda M, et al. Azithromycin combination therapy with artesunate or quinine for the treatment of uncomplicated plasmodium falciparum malaria in adults: A randomized, phase clinical trial in Thailand. Clin Infect Dis. 2006; 43:1264-71