THYROID NODUL “COLLOID GOITER”
WITH UNILATERAL THYROIDECTOMY
Ashri Yudhistira, Farhat, Rizalina A Asnir, Suriyanti
Otorhinolaryngology Head and Neck Department
Medical Faculty, University of Sumatera Utara
Introduction
Lumps in the thyroid gland is a symptom that is often found in the thyroid gland abnormalities, clinically recognizable, and most patients come to the clinic with complaints of a lump in the front of the neck. Basically enlargement of the thyroid gland can be caused by various diseases that do not require surgery. Enlargement of the thyroid gland is generally known as a goiter. Surgical treatment is mainly done in thyroid cancer, may also be indicated on a benign enlargement of the thyroid gland when it puts pressure on the trachea, esophagus, with shortness of breath, a sense of choking and swallowing disorders (Pasaribu, 2006).
Case Presentation
A 22-year-old female, was admitted to Adam Malik General Hospital on Mei 15th 2012 with chief complaint visible lump of the anterior leftneck region for the last 5 years presented, grew slowly, painless and lump part moves upward when the patient swallows. She also complaint neck discomfort and worried if the lump get bigger. Th
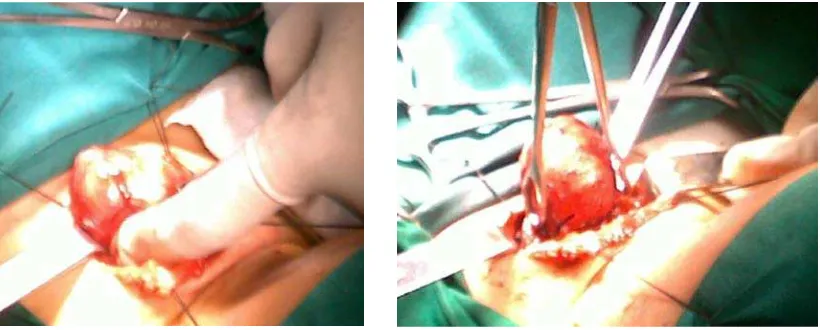
On physical examination vital sign was normal. ENT routine examination, we found ears were normal, nose were normal, the patient presented with single, solid, well-defined, nontender mass with size 4 x 4 x 3 approximately of the anterior left neck region (Fig. 1 and 2).
ere was no history of dysphagia, dyspnoea, hoarseness and loss of weight. She didn’t have history of head and neck irradiation exposure.
Previous Fine Needle Aspiration Biopsy (FNAB) revealed colloid goiter with hyperplasia epitel folikuler. Laboratory finding T3 : 1,45, T4 : 9,17, TSH : 1,650. Radiologically, cervical plain rontgen revealed there was no abnormality.
Figure 1& 2. Mass of the left anterior neck region.
Figure 3. Pehacain injection Figure 4. Horizontal incision
.
Figure 7. Tumor mass Figure 8. Rinse with NaCl
Figure 9. Wound suture Figure 10. Post operative
Discussion
A clinically solitary thyroid nodule is a discrete swelling within an otherwise palpably normal thyroid gland. With time, solitary thyroid nodules may enlarge, shrink, or even disappear spontaneously, but most do not change appreciably. Most of these nodules are benign colloid nodules composed of irregularly enlarged follicles containing abundant colloid. Most are actually the largest of multiple colloid nodules in small, clinically unrecognized multinodular goiters. Other causes of benign solitary nodules are thyroid adenomas, cysts, and thyroiditis. Approximately 5 percent of all solitary thyroid nodules are thyroid carcinomas (Wood et al 1998).
Fine-needle aspiration (FNA) is the main modality used today to investigate thyroid nodules. Its high accuracy, low morbidity, and cost-effectiveness make it an important tool in determining the need for surgery or observation (Bahar 2003, Myer 2009 ). In this case we found colloid goiter with hyperplasia epitel folikel.
Given the imprecision of palpation, ultrasonography is critical for evaluating changes in nodule or goiter volume in studies of therapy, but it is not indicated for routine clinical management. In these cases, ultrasonographic guidance didnot used.
The main indications for treatment of a euthyroid patient with a benign thyroid nodule that is not hyperfunctioning are compression of the trachea or esophagus, growth of the nodule, and recurrence of a cystic nodule after aspiration. Other indications for treatment are neck discomfort, cosmetic concern, and the patient's anxiety about the nodule. The main therapeutic options are surgery and thyroxine treatment (wood, 2003). In this case patient felt neck discomfort and anxiety about the nodule, so we managed the nodule by unilateral thyroidectomy.
Conclusion
Fine-needle aspiration biopsy should be the first test performed in a euthyroid patient with a solitary thyroid nodule. Indications for treatment are : Compression of the trachea or esophagus , venous-outflow obstruction, growth of the goiter, neck discomfort and cosmetic issues.
We reported a case of colloidal goiter that managed with unilateral thyroidectomy in a 22- year- old female and resulted in favorable out come.
References
Bahar G, Braslavsky D, Shpitzer T, Feinmesser R, Avidan S, The cytological and clinical value of the thyroid “ follicular lesion” , American journal of otolaryngology, 2003
Christiansen, Leighton L, Thyroidectomy and thyroid lobectomy, IOWA head and neck protocol, 2014
Frilling A, Liu C, Weber F, Benign multinodular goiter, scandinavian journal of surgery 93: 278-281, 2004
Holzheimer RG, Mannick JA, Benign nodular thyroid disease, surgical treatment: evidence- based and problem-oriented; 2001
Myers E N, Thyroidectomy, Myers surgery, 15- 9 -2009
Pasaribu E T, Pembedahan pada kelenjar tiroid, majalah kedokteran nusantara volume 39, no 3, september 2006
Sharma B, A case of colloidal nodular goiter, indian journal of research in homoeopathy, vol 5, no 2, april- june,2011
Wong C, Wheeler M, Thyroid Nodules : Rational Management, World journal of Surgery, 24, 934-941, 2000