242
Tedjasulonanaetal. Med J IndonesRetrieval Impairment
in
Generalized
Tonic-Clonic Epilepsy and
Complex
Partial
Epilepsy
Rimawati
Tedjasukmana, Lily
D.
Sidiarto, Sidiarto Kusumoputro
Abstrak
Banyak pendertn epilepsi mengeluhkan gangguan daya ingat, terutama epilepsi parsial kompleks. Selain itu daya ingat pada epilepsi dilaporkan dipengaruhi olehfalctor-fal<lor seperti jenis serangan, f'rekuensi serangan, umur pada serangan awal, obat-obatan,
dII.
Tetapi data-data yang adadari
hasil penelitian masih membingunglcan.Untuk mengevaluasiritrival
pada penderita epilepsi digunakan Test PengingatanSelektifpada44penderitaepilepsi(30penderita epilepsi umum tonik-klonik dan l4penderitaepilepsiparsial
l<nmpleks) yang berobatdi
Poliklinik
Saraf RSCM selama perbde satu tahun. Setelnh dilakukan tes dinilai skor ritrival dan penùnbunan. Kemudian gangguanitrival
dianalisis terhadap beberapa variabel: jenis serangan, frekuensi serangan, umur pada serangan awal dan dosis obat (fenobarbital). Juga dilakukan analisis proses daya ingatyang terganggupada penderitayangritivalnya
buruk. Pada sebagianbesar(757o) kasus epilepsiditemukan skorritrivalnyaburuk. Padakelompok epilepsiumum-tonikklonikrata-rata skonnya 7,77, sedangl<nn pada epilepsi parsial kompleks 8,36. SIar
ritival
tidak dipengaruhi oleh jenis serangan, frekuensi serangan dan dosis obat. Walaupun secara statistik tidak bermakna, terdapat kecenderungan skor yang buruk lebih banyak lerdapat pada kelompok dengan serangan awal pada usia kurang dari 10 tahun. Pada analisis proses daya ingat yang terganggu ditemukan bahwa walaupun rata-rata penimbunan awal dan rttrival pada kedua jenis epilepsi tak jauh berbeda, tetapi rasio penimbunan/rttrival pada epilepsi parsial komplekslebih
baik dibanding dengan epilepsi umum tonik-klonik Jadi pada kelompok epilepsi parsial kompleks penimbunanterjadilebihdini. Sebagianbesarkasusskorrttivalnya buruk dan halini
tak dipengaruhiolehienisserangan,frekuensiserangan, serangan awal maupun dosis
obat
anti-epilepsi. Jadi kemungkinan gangguan retrival pada epilepsi merupakan akibat multifaktoiaL Pada epilepsi umum tonik-klonik selain gangguctnritrival terjadi
gangguan penimbunan, hal ini kemungkinan terjadi kar ena gan g g uan at ensi.Abstract
Many epileptic patients complain of
poor
memory, especially those with complexpartial
seizures. Memoryin
epilepsy is reportedly influencedby
severalfactors
like seizure type, seizure frequency, age at onset of epilepsy, anti-epileptic medication, etc. However, the available data are somewhat confiising and do not provide any clear answers. In order to evaluate retrieval in epileptic patients the Selective Reminding Test was used in 44 epilcpsy partents (30 with generalized tonic-clonic epilepsy and 14 withpartial
complexepilepsy)whoweretreatedintheoutpatientclinic of
the DepartmentofNeurologyoftheDrCipto Mangunkusumo Hospitalduring
one year period ( 1993-1994). AII subjects had passed elementary school, were without severe brain damage, had their last seizure more than 24 hours ago andonly take one anti-epileptic
drug
(phenobarbital). Retrieval impairment was analyzed with respect to thefollowing vaiabLes: seizure type, seizurefrequency, age at onseî and drug dose. In subjects with impaired reffieval the ncnwryprocesswereanalyzed. Impairedretrievalwasfoundinmostsubjects(75Vo). The mean retrieval scoreswereT.TTforsubjects with generalized tonic-clonic epilepsy and 8.36for
subjects with partial complex epilepsy. There is no correlation betvveen seizure type and retrieval (t test). Mosr subjects had low frequency seizures, but mean retrieval scores were impaired both in the high frequency (717o) and the low frequency (687o) group (not significantwith chi-square test). Althoughit
was statisticallynot
significant there wasa
tendency that thegreatestretrievalimpairmentw,asinthegroap with early ageat
onset (lessthanl0years).Althoughmost subjects had low doses of phenobarbinl, most of themlnd
impaired retrieval. There is no correlation between drug dose and retrieval (chi-square). In analyzing the impaired memory processes although there was little dffirence in the initial storage and retrieval in both types of epilepsy, the storage/retieval (S/R) ratio were belterin
complexpartial
epilepsy (0,5or
less)than
in generalized
tonic-clonic epilepsy (more than 0,5). In complex partial epilepsy initial storage occured earlier. Most epilepsy patients had impaired retrieval; and it wasnot
influenced by seizure type, seizure frequency, age at onset and anti-epileptic drug dose. Impaired retrieval in epilepsy is probablya multifactorinl disability. Also in
generalized tonic-clonic epilepsy there was impaired initial storage besides retrieval, this was probably caused by disturbance of attention.Keyworils: epilcpsy, seizure type, seizurefrequency, age at onset, drug dose, selective reminding test, retieval, storage.
Departmeû of Neurology, Faculty of Medicine, University
of
IndonesialDr.Cipn
Mangtnhuwno Hospinl, lalarta,
Indonesia
Vol 5, No 4, October - December 1996
100.000
and
the prevalence
is
4-8 per
100.000. The numbers wererelatively
constantin
sàveral countries.2In
Indonesia
epidemiological
study
onepilepsy is
not
yet performed,
but
it
was surmised that
theincidence
andprevalence is
the same.Traditional
or
conventional
treatmentin
patients
with
epilepsy is directed to
drugtherapy
adjustments basedon the type, severity
and
frequency
of
seizures, andthe
side effects
of
anti-epileptic drugs. However,
epileptic
seizures andanti-epileptic
drugs have a greatimpact
on
the
life of
a
patient
with epilepsy,
i.e.psychosocial problems. Several factors
influence
thequality of life of
thepatient
with
epilepsy,
i.e.
seizurereccurency,
psyhosocial adaptation, behavior
dis-turbances, also
deficit
of
cognitive function
and
be-havior
disturbances causedby
anti-epileptic
drugs.Many epileptics,
even thosewith
mild
symptoms,com-plain
of poor
memory.'
In
clinical
practice generally
the patients wereonly
treatedwith
anti-epileptic
drugs, thememory
deficits
went
frequently
unnoticed.
How-ever, this
problem
needs specialattention
as thepatient
requires a
holistic
treatment approach,
including
his
social function.
Memory deficits
in
epileptic patients
merit
specialattention
sincethey
seek helpfor
these morefrequently
thanfor
anyother mental impairments. Interest
in
thisarea
is
not new; Tissot (1170), Gowers (1881),
andReynolds (1861)
had discoveredthat memory
impair-ment was
frequently
found
in
epileptics.a
In
clinical practice memory
disturbance
is more
fre-quently found
in
complex
partial
epilepsy. However,
in
many
studies
there is still
disagreement whether
thereis
adifference
in
thememory functions
of
com-ple"x.partial
and
g
epilep-sy.J'J'u"
Most
comp
edfrom
temporal
andfrontal
7O-8OVoof
temporal lobe epilepsy begin
in
thehippocu-por.8
These facts are a
little
perplexing
as we understand theimportant
role of
thetemporal lobe
andespecially
thehippocampus
in
memory functions.
Another problem
is
what
other factors can influence
memory. Besides seizure type, other
fac-
tors like
seizure
frequency,
seizure onset,drugs, etc,
had beenreported to
influence
memory; however, other
studiescould
not
prove
it.
In
developing countries
like
Indo-nesia drugs are more
often
chosenfor their
availability
and their
low
prize,
so many epileptics here
usephenobarbital.
Reports ofdeleterious
effects ofpheno-barbital on cognitive function
present
an important
question
of how
farit
has reduced the human resources here.Retrieval in
Epilepsy
243ln
conclusion, the available
datais
somewhat
confus-ing
and do
not give
any clear
answersto
those
ques-tions. Probably
this
was
causedby
differences
in
thetype of
test used(many
tests werenot especially
madefor memory
testing), the sampling method
and usageof
anti-epileptic
drugs.In this study
we propose to usea
simple
and
widely
usedtest
that
can show
the
dif-ferences
in
the
memory process,i.e.
the
selective
reminding
test.Also
the patientsincluded
in
this study
only
used onekind
of
anti-epileptic drug
(phenobarbi-tal).
MATERIALS
AND METHODS
Subject
Subjects were patients attending the
outpatient clinic
of
theDepartment of
Neurology of Dr.
Ciptomangun-kusumo
Hospital
andthe
PemudaNeurologic Clinic,
Jakarta,
during
one year
period
(1993-1994).
All
patients were
confirmed to
haveepilepsy by
history
of
seizures,
neurological examination and/or EEG,
andcould
beclassified according
to thelnternational
Clas-sification
of
Seizures. Patients
were
selected
for
in-clusion based
on
the
criteria:
minimum
education
primary
school, noneurological
signs onexamination,
useonly
one
anti-epileptic drug (phenobarbital),
and thelast
seizure wasmore
than 24hours
ago.The
generalized
tonic-clonic
epilepsy
group
with
generalizedtonic-clonic
seizureswithout
aura andnor-mal EEG
or
generalized
epileptiform/slow
wave
bursts. Thecomplex partial epilepsy
groupwith partial
seizures and loss
of
consciousness,
not followed
by
generalized
seizures at leastduring the previous
year,and
normal EEG
or
focal
epileptiform/slow
wave
bursts. Patients with history
of
head trauma,
CNSinfection
or
neoplasm;
with
secondarily
generalized
seizuresor
generalizedtonic-clonic
seizureswith focal
bursts
onEEG were excluded
from
the study.
During
one year
period we found
44 caseswhich fuititted
thecriteria,
30 cases generalizedtonic-clonic
epilepsy
and14 cases
of
complex
partial
epilepsy.
Procedure
Examinations
were conductedin
aquite
andadequate-ly
lighted room. Name, gender, education,
seizuretype, EEG
patterns, seizure
frequency,
age
at
onset,anti-epileptic
drugs and dosage were recorded.Educa-tion
waslevel of
education
passedin
years.EEG
was244 Tedjasulonana et al.
The
selective
reminding
test was administered
to all
subjects.
The patient was
askedto
learn
a
list
of
10words by verbal recall
in
any order. The entirelist
was reaù a\ouù once to thepatient
at a2-seconùratebelore
his
first recall
attempt. The patient
thentried
to recall
all of
thewords in
thelist in
any order. Thepatient was
selectively reminded only
those items he did notrecall
on the immediate
preceding
trial
before he
again
at-tempted
to recall
all
items
in
the list.
The
procedurewas
continued
until all
10 itemscould be recalled
on 2consecutive
trials.
Retrieval score
is
the number
of
trials
minus
one.Buschke had discovered that
recall failures
representretrieval failures rather than loss
from
storage.eIn
conclusion recalled items are
itemsretrieved from long
term
storage.Yunus found thatthe mean
retrieval
scorewas
4
or
less
in
normal
individuals,
and
it
was
not
influenced by age
oreducational
level.l0
The subjectswith
poor
retrieval
scoreswere
analyzedtheir
storage/retrieval ratio.
Storage score
is
the number
of
trials
when
all items
had entered storage.
An item is
con-sidered
in
storagewhen
the subject canrecall
theitem
without
representation. Data were
analyzedwith
t testfor
2independent
samples and thechi-square
test.RESULTS
During
oneyezr period we found
44 casesof
epilepsy
which
fulfilled
the
study
criteria,
30
cases with
generalizedtonic-clonic
epilepsy
and 14with
complex
partial epilepsy. Descriptive information on the two
groups
included in this
study
is
presentedin Table
1.Between the
two
groups there were
no
significant
differences
in
gender(chi-square test), age,
education, anddrug
dose(t test).
Table 1. Characteristics of the two groups of epilepsy
Characteristic
Generalized
ComplexTonic-clonic
PartialStatistic
Med J Indones
Both
groups
hadthe
samedistribution
of
seizure
fre-quency
with
low
seizure frequency
in
most
cases.In
the
generalizedtonic-clonic
(GTC)
group
56.677o (17c,ases) anù
in
the comp\ex
paftïa\ (CP)
group
42.8590(6
cases) had lessthan
I
seizureper year.
Only
afew
cases hadhigh
seizurefrequency,
1 case (3.33Vo)with
GTC
and
2
cases (14.29Vo)with
CP
seizures.
There wasno difference
in
ageat onset
of
seizuresin
both
groups.
Most
cases had seizure onsetin
the age
rangeofl0-17
years, 43.33Eo
(13
cases)in
the GTC
group
and
57.l4Vo
(8
cases)in the
CPgroup.
In
conclusion
both
groups had the same characteristics.Table
2lists
the
retrieval
scoresof
both
groups.
The mean score of GTC group was 7 .77 and CP group 8.36.Analysis
\À/ith t testfor
2independent
sampleswith df
42
revealed
no significant difference
between
the
2 groups(p>0,2).
From
the
44
casesstudied,
25Vo(11
cases)had
goodretrieval with retrieval
scores4 or less
and 75Vo (33cases) had poor
retrieval
with
scores more than 4.More
thanhalfofthe
cases (23 cases) had less thanI
seizure per year(Table
3).However, nearly all cases
hadpoor
retrieval,
andmost cases
with
poor
retrieval
(36.78Vo)had
lessthan
1 seizureper year. So we can conclude
that
retrieval
scoresis not influenced by
seizure
fre-quency (chi-square
test,p>0,2).
The situation
appearsclearer when we
simplify
theseizure frequency
to
low
(less than once
per
month)
and
high
(onceper month
or
more) frequency.
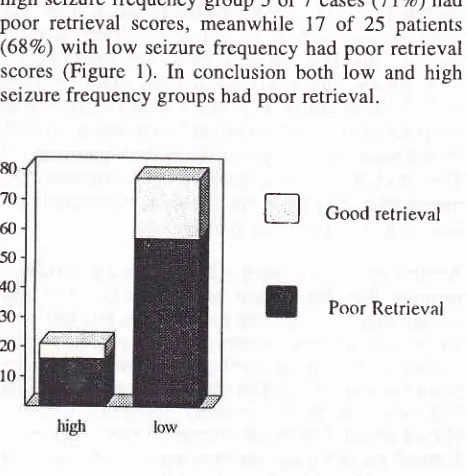
In
thehigh
seizurefrequency group 5
of7
cases(71Vo)had
poor retrieval
scores,
meanwhile
17
of
25
patients (687o)with
low
seizure frequency had
poor retrieval
scores
(Figure 1).
In
conclusion
both
Iow
and
high
seizurefrequency
groups hadpoor
retrieval.
E
Good retrievalPoor Retrieval
No.
Age:
- Mean-SD
Gender:
- Male- Female Education: - Mean
-SD
Drug dose: - Mean-SD
30
2',1.2
't.38
18
l2
10.33 2.5 114.5 59t4
27.64r0.99 6
8
NSU
NSb
80
70
60 50
40
30
2n
10
8.79
NSU3.2
114.64
NSa73.97
a t
test for 2 independent samples
o chi-square test witb
Yates correction Figure
I.
Seizure [image:3.595.310.543.481.719.2] [image:3.595.49.281.553.734.2]Vol 5, No 4, October - December 1996
Table 2. Seizure type and retrieval.
Retrieval in
Epilepsy
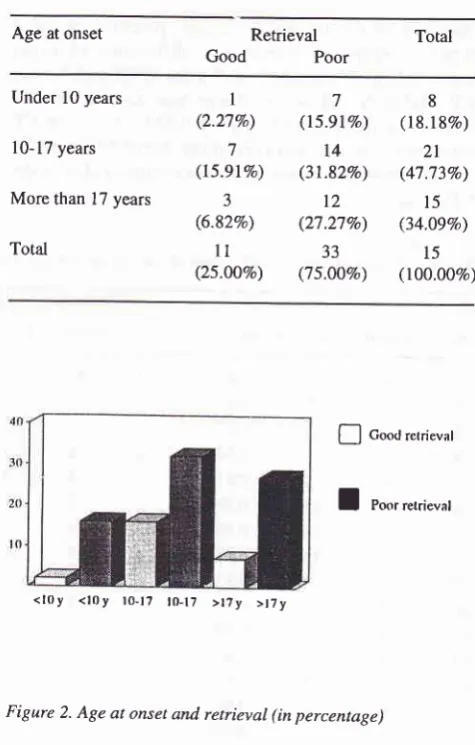
245Age
at onsetin
most cases
(47.73Vo) wasin
the rangeof
10-17 years.[n
thegroup
with
age at onsetunder
l0
years
only
I
of
7
patients had
good retrieval,
in
the10-17 years
group 7
of
14patients and
in the
group
with
age at onsetof
morethan 17
years 3of
12 patientshad good
retrieval. Although
it
was statistically not
significant (chi-square test),
from this data we
canconclude
that there was
a
preponderance
of
poor
retrieval
scoresin patients
with
early
onsetof
seizures(Table
4 andFigure
2).Table
4. Age
at seizure onset epilepsyand retrival
in
both typesof
Age at onset Total
Generalized Tonic-Clonic
No
ScoreComplex Partial
No
ScoreI
2 3 4 5 6 7 8 9l0
ll
12l3
t4
l5
16 t7l8
l9
20 2t 22 23 24 25 26 27 28 29 30l5
9 8 10 J 9l5
5l4
6l0
7 J 4 7 6 6 5 3 7 4 6lt
J t5 8 8 7 t5 4I
2 J 4 5 6 7 8 9l0
1t t2 t3l4
l5
l4
l0
l5
4 4 4 15 5 8 6 8 6 3 RetrievalGood
PoorUnder
l0
yearsl0-17 years
More than 17 years
Total
I
(2.27%) 7 (l5.9lVo) 3 (6.82Vo)ll
(25.00Vo) 7 (l5.9lVo)l4
(31.827o)t2
(27.27Vo) 33 (7 5.ÙOVo) 8 (18.187o) 2t (47.73Eo)l5
(34.09Vo)l5
(t00.00Vo)Table 3. Seizure frequency and retrieval in both epilepsy groups
Seizure
Retrieval
TotalGood Poor
{-l
Goo<J retrieval [image:4.595.176.538.83.649.2]I
PoorretrieralFigure 2. Age at onset and
retieval (in percentage)
Most
patients (40.9|Vo) were
receiving
phenobarbital
5l-l0Omg per
day,
only
a few
patients
(6.g2%o)received more than
200 mg per
day.
However,
most
patients had
poor retrieval,
even those
who
received
low
dosesof
the drug (Table 5). Analysis
with
chi-square test revealed no
relationship
between drug dose andretrieval.
Once or more per week
l-3 times
a monthLess than once a month
Less than once a year
Total
I
(2.27Eo)I
(2.278o) J (6.82Vo) 6 (13.64Vo)ll
(25.00Vo) 2 (4.548o) 5 (11.37Eo) 9 (20.45Eo)l7
(36.78%) 33 (75.00Eo) J (6.8lVo) 6 (t3.64Vo) t2 (27.27Eo) 23 (52.2880) 44 (100.00%) [image:4.595.59.301.88.548.2] [image:4.595.308.546.264.637.2] [image:4.595.49.282.568.736.2]7
246 Tediasukmana et aI.
Table 5. Drug dose and retrieval in both epilepsy types
Drug dose Retrieval
Med J Indones
DISCUSSION
During
one year wefound
44 caseswhich
fulfilled
the studycriteria. This
was arelatively
small
samplecom-pared
with
other studies, but the advantage ofthis
study was a more homogenous sample.In this
study subjects wereambulatory epileptic
patients usingonly
onedrug
(phenobarbital)
andwithout
major CNS
disturbances.EEG
with
simultaneous
video monitoring
is
not
yet
available
in
our
country,
soit
is possible that patients
with
GTC
seizures
actually had partial
secondarily
generalized seizures.
It
is also
possible that
patients
had
subclinical
seizureswhile
undergoing
the testthat
could influence
the test results.The
30 patientswith GTC
and 14patients
with
CP hadthe
samecharacteristics
(age, gender,education, drug
dosage).
Most
casesof
both groups
had less
than I
seizure ayear,
and age at onsetfrom
10-17 years.We
conclude that both groups were
relatively similar
and homogenous.Total Good Poor
0-
50 mg51-100 mg
l0l-150
mgl5l-200
mg201-250 mg
J (6.82Vo) 5 (11.37Vo)
I
(2.27Vo)I
(2.27Vo)I
(2.27Vo) 6 (13.63Vo)l3
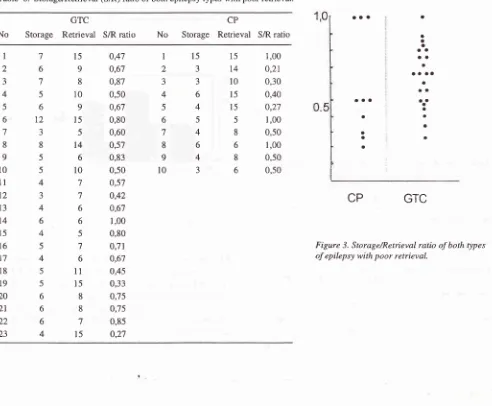
(29.54Vo) 7 (ts.91%) 5 (ll.37Vo) 2 (4.45Vo) 9 (20.45Vo) 18 (40.91%) 8 (l8.l8Vo) 6 (13.64Vo) 3 (6.82%)Analysis
of
the impaired memory
proccess
in
the
2types
of
epilepsy revealed
no
difference
of
meanvalues
of initial
storage,i.e. 5.4 for GTC
and5.3
for
CP
(Table
6).
However, there was significant
dif-ference
in
the storage/retrieval (S/R) ratio,
with
CP seizures 0.5or
less andGTC
more than 0.5(Figure
3). So weconclude
thatinitial
storage occured ealier in theCP
group.
Table
6.
Storage/Retrieval (S/R) ratio of both epilepsy types with poor retrieval.No Storage
GTC
Retrieval
S/R ratio No StorageCP
Retrieval S/R ratio
0,47 0,6't 0,87 0,50 0,67 0,80 0,60 0,s7 0,83 0,50 0,57 0,42 0,67 1,00 0,80 0,71 0,67 0,45 0,33 0,75 0,75 0,85 0,27 1,00 0,21 0,30 0,40 0,27 1,00 0,50 1,00 0,50 0,50 aaa aaa a a a a aa oa t
a a aa
a ao aaa a a a o
I
2 3 4 5 6 7 8 9 10 11 12l3
t4
l5
l6
17l8
t9 20 21 22 23 7 6 't 5 6t2
3 8 5 5 4 J 4 6 4 5 4 5 5 6 6 6 4l5
9 8 10 9l5
5t4
6l0
7 7 6 6 5 7 6 l1 15 8 8 .| 15 I 2 J 4 5 6 7 8 9 t0 t5 J J 6 4 5 4 6 4 3 15 14 10l5
l5
5 8 6 8 6 a a a aCP
GTC
Figure 3. Storage/Retrieval ratio ofboth types
[image:5.595.57.296.100.258.2] [image:5.595.61.553.396.802.2]Vol 5, No 4, October - December 1996
Results
of this study
showed that patientswith CP
andGTC
seizures had
the
distur-bance. Studies by
Loise
ted thesame
results. Other
i
stein,sGlowinski,l2
Mungas,
d
that
patients
with
CP
seizures
were
at
greater
risk
for
memory
difficulties
compared
to
patients
with
GTC
seizures.Meanwhile Matthews
andKlove
demonstrat-ed on the
contrary.l4
Inconsistent findings
seem
to
be influenced
by
dif-ferences
in
the patient population. Thompson
pre-sumedthat memory
impairment in
patients
with
GTC
was greater
than
patients
with
CP
when the
patientsstudied
hadless
severe seizuredisorders.l5 However,
in
our
opinion
ambulatory epilepsy
patients cangive
aclearer picture
of
memory impairment
in
epilepsy.
Hospitalized
patientsusually
have severe andfrequent
seizures, consequently
there
is
permanent brain
damage thatcan iggravatethe memory difficulties.T'15
Also in
patients
with
intractable
seizuresit
is
difficult
to
decide when
to
do the test, due
to
the
frequent
selzures.Another explanation
is
that every
disturbance
in
theCNS,
like
epileptic
seizures
or
anoxia,
causes
therelease of high
concentrations
of the
neurotransmitter
glutamate.
The
NMDA
(N-Methyl-D-Aspartate)
receptor, one of the glutamate receptors, residesmostly
in
the CA1 areaof
thehippocampus
and is also presentin
the
dentate
gyrus and neocortex. Glutamate can
destroy neuronsin
minutes,resulting
in thedestruction
of
the
CAI
area. TheCAl
areaof
the hippocampus
plays a
great
role
in
long term potentiation, which is
the basisof
learning or long term
memory.16This fact
wasrecognized since
1967 byGlaser who
discoveredthat the
limbic
structure was
very
susceptible
to
pathologic
processesincludin
g_i schaemia,encephalitis
and metabolic disturbances.t'
In
conclusion
every
seizure can causedestruction of
CAl
cells resulting
in
memory
impairments. Furthermore,
in
GTC seizures
there
areepisodes
of
hypoxia that
can
aggravate thecondition.
In
clinical
practice poor memory
was moreoften
com-plained
bypatients
with
complex partial
seizures.This
could
be
caused
either
by
the
seizure
itself
or
by
depression.Patientswith
temporal lobe epilepsy often
havepsychiatric
disturbanceslike depression.
Depres-sion
in
thesepatient can be
causedby social stigma,
and also
due
to
lesions
in
the
limbic
system
which
controls
emotion.lT
Retrteval in
Epilepsy
247Both
groups
hadpoor retrieval
scores(more than
4),i.e.7.77 in
the
GTC
group
and8.36
in
the CP
group.This
fact conforms
with
the
studiesbv Matthews
andKlove,l4
Loiseau
et al3 andSmith et
al,8which found
that
memory impairment was greater
in
epileptic
patients
thannormal control.
Memory impairment could
also
be
caused
by
anti-epileptic
drugs, i.e. phenobarbital. Phenobarbital
wasknown to
have deleterious
effects on the memory
of
patients
with epilepsy.ls'19
It
wasproved
thatmemory
impairment
was greater in patients usingphenobarbital
compared toother
drugs,although they
had lowblood
leveis
of phenobarbitai.
19In
this
study most patients
(74Eo)had
poor
retrieval,
both
in
patients
with
frequent
seizures(7lVo)
and lowseizure frequency
(68Vo).
Other investigators had
found the
sameresults,,that
seizurefrequency did
not
influence -"rno.y.3'4'ls'20 As
indicated
by Dodrill,
it
may be the total lifetime number
of
seizures (rather
than seizure frequency)
which
is
the
crucial
vari-able.15'20
The severity
of
the
attack
may
also
be
animportant factor. However,
it
must
always be bornein
mind
that seizurefrequency
orseverity
mayreflect
theextent
and natureof iny
underlying
biain
pathology.l5
ea
Y.ess
;4ofi
n-sequently
even inpatients
with low seizure
frequency
the destructive
process
goes
on,
resulting
in
brain
damagewhich may influence memory functions.
In this
studymemory impairment
was morefrequently
found
in
epilepsy
with
early
age
at
onset
(under
l0
years).
This conforms with Dikmen et al which
alsofound
the
same thing.22Meanwhile
Loiseau et al
dis-coveredmore frequent memory
impairment in
ep!l_ep-sy with onset during adolescence
(10-17
years).r'r)
An early age at onset
is
arecognized deleterious
fac-tor.4
This fact
isnot surprising,
becausechildhood is
avery important period
for
learning,
a period
during
which
one learnshow to
learn.Meanwhile
epilepsy
isa chronic
pr
in
bloodflowzl-
ge,po"u*por.23
stu248
Tedjasuknanaetal.Several
anti-epileptic
drug
cancontribute to
disordersof
memory, including
phenobarbital
which
was used
in
this studr.ls'ta
Th"isstudy
revealed
poor
retrieval
scores
in
most patients,
both
in
the
low
dose and thehigh
dosegroup. Meanwhile Camfield
discoveredthat
barbital
concentration influenced
other investigators could not prove
the 4In
general,
themost dramatic effects
of
anti-epileptic
drugs have been
reported in patie_qts
onpolytherapy or
with
high levels
of
medication.rt'to
This study
usedsubjects
receiving therapeutic dose
ofonly
onekind
of
drug,
although
without
serum
drug
concentration
monitoring. And
theresults
showed thatdrug dose
did
not
influence retrieval
scores.On the effects
of phenobarbital
on memory there isstill
controversy,
in
generalpenobarbital
has worseeffects
compared
to
other drugs but the difference may
besubtL.3'ls'26
It
was proved
that
phenobarbital
in-fuenced
shortterm memory,
and had noeffect
onlong
term memory.
The
Selective Reminding Test
usedin
this study
evaluatedretrieval
from
long term memory,
consequently phenobarbital
hadlittle
effect
on the testscores.
Finally it
has to be bornein mind
thatinterpret-ing investigations
of
this kind
is difficult,
since
anynegarive
drug effects would
bg_expectedto
beoffset
by improved
seizurecontrol.IJ'zu
Soit
wasnot
unex-pected
that we found
no
infuence
of
drug
dose
onmemory disturbance.
The
advantageof
using
theSelective Reminding Test
is
that
wecan
analyze the partsof
thememory
proces-ses impaired.
Until
recently
the
parts
of
memory
processes
impaired
by
epilepsy
arenot well
defined.aWith this
test
we
can evaluate
llorage, retention
andretrieval in
disordered
memory." This information
isimportant
to
enhanceour knowledge
in
the
fields of
memory
andepilepsy.
In
this study both epilepsy groups
had the same meanof
initial
storage,but
different
storage,/retrieval
(S/R)
ratio.
The S/Rratio of
mostof
the CP group was 0.5or
less,
only 3
subjects the
ratio was
1.Further
analysisof
the CP group
showed
(Table 6) only
one
subject(subject
no.1)
hadvery poor retrieval
(score
15), andthe other
2
subjects (no.
6
and8)
hadrelatively
goodretrieval
(score 5 and 6).Meanwhile
in
the GTC groupmore than
50%
subjects the S/R
ratio
wasmore
than 0.5.From
thesefacts
we
can conclude that
initial
storageoccured
earlier
in
CP epilepsy, and
difficulties
in
Med J Indones
recalling
items
was causedby retrieval
disturbance
of
items
in
storage.Meanwhile in GTC
epilepsy
thedis-turbance
is
in initial
storage,
difficulties
in
recalling
items are caused
by retrieval impairment
and itemsnot
yet
in
storage.ltems
can enterlong (erm
storagewhen
ihere
is
atiention.2s'2eParients
iho
huu"
difficulty
maintaining
attention
will
have
difficulty
in
learning.
There is some evidence that
attentional
difficulties
can befound in
some subgroupsof
patients
with
epilepsy
and
that individuals
with
generalized seizures are at
most
risk.ls This fact
couù
explain
the
difference in
initial
storagein
both epilepsy
groups.CONCLUSION
In
this
study most
casesof
epilepsy
(75Eo)had poor
retrieval,
andretrieval
was
not influenced by
seizuretype,
seizure
frequency
or
anti-epileptic
drug
dose.Although
it
wasstatistically
not
significant,
therewas-a
tendency
of
greater
retrieval
difficulties in
in-dividuals
with
early age at onset.
It
was also discoveredthat
in GTC
epilepsy there was greater
difficulties in
intial
storage comparedto
cP
epilepsy.
In conclusion,
there ismemory
disturbance inepileptic
patients,
but this
study
could
not
find
the factors that
influence
it.
If
considered
individually, none
of
thefactors concidered
accountedfor
this impairment.
Thememory disturbance
in
epilepsy
is probably
amulti-factorial
disability.
Besides thatepilepsy
is an ongoing
process
even interictally, resulting
in
brain
damagethough
thepatient
appearsnormal.
Memory
disturbance
in
epileptic
patients
merits
spe-cial
attention, since
it
can disturb
their lives.
To
evaluate
memory
deficit
in
epilepsy
the
Selective
Reminding
Test
canbe used.Other factors
like
atten-tion
disturbance,
concentration and emotion (i.e.
depression)
in
patients
with
epilepsy need special
at-tention;
because they can alsoinfluence memory.
Fur-ther studies are neededwith
greater sample size and onpatients
not
on medication
to
exclude drug effects
onmemory.
REFERENCES
l.Porter RJ. Classification of epileptic seizures and epileptic syndromes. In: Laidlaw J, Richens A, Chadwick D, eds. A Textbook
of
Epilepsy.4th
ed. Edinburg:Churchill
Li-vingstone, 1993:1-22.Vol 5, No 4, October - December 1996
3. Loiseau P, Strube E, Broustet D, Battellochi S, Gomeni C,
Morselli PL.
Leaming impairmentin
epileptic patients. Epilepsia 1983 ; 24: 183 -92.4. Loiseau P, Strube E, Signoret JL. Memory and epilepsy. In: Trimble MR, Reynolds EH, eds. Epilepsy, Behaviour and Cognitive
Function.
Stratford-upon-Avon Symposium, November 1987. Chichester: John Wiley and Sons, 1988: 165-73.5. Bornstein RA, Pakalnis A, Drake ME, Suga LJ. Effects
of
seizure type and waveform abnormality on memory and attention. Arch Neurol 1988;45: 884-7.6. Dodrill CB. Neuropsyhology of epilepsy. In: Filskov SB and Boll TJ, eds. Handbook of Clinical Neuropsychology. New York: John Wiley
&
Sons, 198 I : 287 -319 .7. Loiseau P, Strube E, Signoret JL. Memory and epilepsy. In: Trimble MR, Reynolds EH, eds. Epilepsy, Behaviour and
Cognitive
Function.
Stratford-upon-Avon Symposium, November 1987. Chichester: John Wiley and Sons, 1988: 165-73.8. Smith DB, Craft BR, Collins J, et al. Behavioral charac-teristics of epilepsy patients compared with normal controls. Epilepsia 1986; 27 (6): 7 60-8.
9. Buschke H. Spontaneous remembering after recall failure. Science 197 4; 184: 579-81.
10. Yunus MS. Gangguan Memori Pada Penderita Pasca Cedera Kepala; Suatu Evaluasi Dengan Pengingatan Selektif. Tesis.Fakultas Pasca Sarj ana Universitas Indonesia, I 987. 11. Dodrill CB. Neuropsyhology of epilepsy. In: Filskov SB and
Boll TJ, eds. Handbook of Clinical Neuropsychology. New York: John Wiley
& Sons,
1981: 287-319.12. Glowinski H. Cognitive deficits in temporal lobe epilepsy. An investigation of memory functioning. J Nerv Ment Dis 1973; 157: 129-37 .
13. Mungas D, Ehlers C, Walton
N,
McCutchen CB. Verbal learning differences in epileptic patients with left and right temporal obe foci. Epilepsia 1985 ; 26(4): 340-5.14. Matthews CG, Klove H. Differential psyhological perfor-mânces
in
major motor, psy- chomotor and mixed seizure classifications of known and unknown etiology. J Nerv MentDis 1973; 157:129-37.
15. Thompson PJ. Memory function in patients with epilepsy.
In:
SmithD,
TreimanD,
TrimbleM,
eds. Advances in Neurology. Vol 55. New York: Raven Press,l99l:
369-84.Retieval in
Epilepsy
24916. Carlson NR. Physiology of Behavior. 4ed ed. Boston: Allyn and Bacon, 1991: 434-510.
17. Trimble MR. The Psychoses of Epilepsy. New York: Raven Press,
l99l:
l4-23.18. Camfield CS, Chaplin S, Doyle AB, Shapiro SH, Cummings C, Camfield PR. Side effects of phenobarbital in toddlers; behavioral and cognitive aspects. J Pediatr 1979 95l. 361-5. 19. Meador KJ, Loring DW, Huh K, Gallagher BB, King DW. Comparative
effects
of
anti-
convulsants. Neurology 1990;40:391-4.20. Dodrill CB. Neuropsyhology of epilepsy. In: Filskov SB and Boll TJ, eds. Handbook ofClinical Neuropsychology. New York: John Wiley
& Sons,
1981 : 287 -319.21. Homan RW, Paulman RG, Devous MD, Walker P, Jennings
LW,
Bonte FJ. Cognitive function and regional cerebral blood flow in partial seizures. Arch Neurol 1989',46:964-70.22. Dikmen S, Matthews CG, Harley JP. The effect
of
early versus late onset of major motor epilepsy uponcognitive-in-tel ectual performance. Epilepsia 197 5 ; 1 6: 7 3 -81.
23. Sass KJ, Spencer DD, Kim JH, Westerveld M, Novelly RA,
Lencz^1. Verbal memory impairment correlates with hip-pocampal pyramidal cell density. Neurology l99O; 40:
1694-7.
24. Mac Leod C, Dekaban AS, Hunt E. Memory impairment in epileptic patients: Selective effects
of
phenobarbital con-centration. Science 1978; 202: 1102-4.25. Matthews CG, Harley JP. Cognitive and motor-sensory per-formances in toxic and non- toxic epileptic subjects. Neurol-ogy 1975;25:184-8.
26. Meador KJ, Loring
DW, Allen ME, et al.
Comparative cognitive effects ofcarbamaze- pine and phenytoin in heal-thy adults. Neurology 1991;41: 143'7-540.27. Buschke
H,
Altman P. Evaluating storage, retention andritrieval
in
disordered memory and learning. Neurology 1974;24: 1019-25.28. Lavine
RA.
Neurophysiology: The Fundamentals. Lexi-ngton: The Collamore Press, 1983:l5l-5.