DOI: 10.1542/peds.2009-0326
2009;124;e547-e556; originally published online Sep 7, 2009;
Pediatrics
Filomena Fortinguerra, Antonio Clavenna and Maurizio Bonati
Psychotropic Drug Use During Breastfeeding: A Review of the Evidence
http://www.pediatrics.org/cgi/content/full/124/4/e547
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Psychotropic Drug Use During Breastfeeding: A
Review of the Evidence
WHAT’S KNOWN ON THIS SUBJECT: The evidence on
psychotropic medication use during breastfeeding is limited for many drugs, in particular for antipsychotics, hypnotics, and anxiolytics. This lack of data makes it difficult to formulate any generalizations regarding the safety of these medications.
WHAT THIS STUDY ADDS: We systematically collected and evaluated the available information on the safety of psychotropic medication use during breastfeeding to provide physicians with updated and evidence-based information for current problems in daily clinical practice.
abstract
OBJECTIVE:The objective of this study was to review the existing liter-ature on the use of various classes of psychotropic medications during breastfeeding to provide information about infant exposure levels and reported adverse events in breastfed infants.
METHODS:A bibliographic search in the Medline (1967 through July 2008), Embase (1975 through July 2008), and PsycINFO (1967 through July 2008) databases was conducted for studies on breastfeeding and psychotropic medications for a total of 96 drugs. References of re-trieved articles, reference books, and dedicated Web sites were also checked. The manufacturers were contacted for drugs without pub-lished information. Original articles and review articles that provide pharmacokinetic data on drug excretion in breast milk and infant safety data were considered, to estimate the “compatibility level” of each drug with breastfeeding.
RESULTS:A total of 183 original articles were eligible for analysis. Documentation was retrieved for 62 (65%) drugs. In all, 19 (31%) psy-chotropic drugs can be used during lactation according to an evidence-based approach. For 28 drugs, the available data do not permit an evaluation of the drug’s safety profile during breastfeeding and, for an additional 15 drugs, the exposure dose or observed adverse effects make their use unsafe.
CONCLUSIONS:Although most drugs are considered safe during breastfeeding, compatibility with breastfeeding has not been estab-lished for all psychotropic drugs. There is a need for additional re-search and accumulation of experience to guarantee a more rational use of psychotropic drugs during breastfeeding.Pediatrics2009;124: e547–e556
AUTHORS:Filomena Fortinguerra, PharmD, Antonio Clavenna, MD, and Maurizio Bonati, MD
Laboratory for Mother and Child Health, Public Health Department, Mario Negri Institute for Pharmacological Research, Milan, Italy
KEY WORDS
breastfeeding, psychotropic drugs, drug therapy, adverse effects, human, systematic review
ABBREVIATION
SSRI—selective serotonin reuptake inhibitor www.pediatrics.org/cgi/doi/10.1542/peds.2009-0326 doi:10.1542/peds.2009-0326
Accepted for publication Apr 23, 2009
Address correspondence to Filomena Fortinguerra, PharmD, Public Health Department, Laboratory for Mother and Child Health, “Mario Negri” Institute for Pharmacological Research, Via Giuseppe La Masa 19, 20156 Milan, Italy. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2009 by the American Academy of Pediatrics
Breastfeeding is essential for the phys-ical and psychologphys-ical health of both mother and child, and its benefits are well documented.1–6The World Health Organization recommends exclusive breastfeeding for at least the first 4 to 6 months of life and its continuation for 1 to 2 years thereafter.7,8In the past few years, several initiatives have been launched to promote breastfeeding, which have led to an increase in this first-choice form of nutrition world-wide. Despite the increased attention toward breastfeeding, however, infor-mation on breast milk drug excretion and knowledge of the adverse effects on the infant are often unavailable or still limited for many drugs that fre-quently are used by women of child-bearing age, and misinformation abounds.9
Worldwide, more than half of breast-feeding women take some type of drug,10and the concern about poten-tial harm to the nursing infant from maternal medications is often cited as a reason to stop lactation,11even if dis-continuing breastfeeding is often the wrong decision. The Summary of Prod-uct Characteristics should not be con-sidered a reliable source of breast-feeding information; it often indicates that a drug is not recommended dur-ing lactation, suggestdur-ing that it be avoided or that breastfeeding be inter-rupted. The warnings are not neces-sarily related to observed or reported adverse effects; they are often used as a defensive measure on the part of the manufacturer when the drug’s safety information is not available.
It is important that women be in-formed as to whether they can safely breastfeed while taking their medica-tion.12Information on how to deal with drugs in lactation therefore seems in-dispensable in efforts to promote breastfeeding.13Concerns that also at-tributable to a scarcity of available knowledge about drug safety during
lactation are common for all drugs,14 but for a few therapeutic classes such as psychotropic agents, they are relevant.15
Psychiatric disorders represent a con-siderable public health problem that affects a significant number of preg-nant and lactating women and can have substantial negative physical and psychological sequelae for mother and child. Because of these serious conse-quences, early diagnosis and treat-ment interventions are imperative for the health and well-being of the mother and the child.16
Given the prevalence of psychiatric dis-orders in the perinatal period, a signif-icant number of women may require pharmacologic treatment.17–19 It has been estimated that, each year, more than 500 000 pregnancies in the United States are complicated by psychiatric disorders such as depression, anxiety, and psychosis, which often develop, re-cur, and/or worsen during and after pregnancy. Furthermore, 13% of all psychiatric hospital admissions for women occur during the first postpar-tum year.20
Depression is the most frequent men-tal disorder in the perinamen-tal period:
⬃10% to 16% of pregnant women ful-fill diagnostic criteria for major or mi-nor depression, but up to 70% report symptoms of depression.21 Further-more,⬃7% to 20% of women receive a diagnosis of postpartum depression in the first year after delivery.22 Un-treated depression and anxiety can have a negative impact on pregnancy,23 and adverse short-term and long-term effects can have a negative impact on the developing infant and child.24,25
The evidence on psychotropic medica-tion use in breastfeeding mothers is limited: for many drugs only case re-ports or very small studies are avail-able (often only pharmacokinetic data and not with respect to safety), whereas for other drugs on which
more information is available, the re-views are not complete and updated. This lack of data makes it difficult to formulate any generalizations regard-ing the safety of these medications26–29; therefore, there is a need to collect and evaluate systematically the available information on the risks of psychotropic drugs during breast-feeding. This article reviews the liter-ature to provide more complete and updated information on infant expo-sure levels and reported adverse events in the various psychotropic medication classes.
METHODS
Original articles and review articles on breastfeeding and mother and newborn infant exposure to 96 psychotropic drugs were considered. The drugs were classified according to the International Anatomic Therapeutical Classification system in antipsychotics (N05A), anxio-lytics (N05B), hypnotics and sedatives (N05C), antidepressants (N06A), psycho-stimulants (N06B), and antiepileptics (N03; Table 1). Drug combinations and drugs without indications for women of childbearing age were excluded.
A bibliographic search in the Medline (1967 through July 2008), Embase (1975 through July 2008), and PsycINFO (1967 through July 2008) databases was performed. The searches per-formed were as follows: [drug name] and [breastfeeding or lactation or breast milk or drug milk level], limiting to [human].
To make the search more complete, the terms were searched for in the da-tabases’ dictionaries as well as through a free text search of the key words in the articles’ titles and ab-stracts. Manual searches of bibliogra-phies were also conducted to identify additional pertinent studies. All of the references were then analyzed.
ded-icated Web sites (eg, LactMed, The MotherRisk Program–Hospital for Sick Children, American Academy of Pediat-rics, Martindale, Meyler’s Side Effects of Drugs) were consulted. Other infor-mation was found in the DRUGDEX da-tabase (Micromedex), a Web site that reports data on drugs from the medi-cal literature, and REPROTOX (Repro-ductive Toxicology Center, Columbia Hospital for Women Medical Center, Washington, DC), a database of refer-ences on reproductive risk that also contains a section with studies related to drug use during breastfeeding. For drugs for which no studies were iden-tified through the procedures de-scribed, the manufacturers were con-tacted directly. The references retrieved were collected and analyzed using the software program Reference Manager 11 (Institute for Scientific Information, Berkeley, CA).
Study Selection
To fit the selection criteria, studies had to provide 2 types of information:
● pharmacokinetic data on drug ex-cretion in breast milk and
● adverse effects reported in breast-fed infants who were exposed to the drug through maternal breast milk.
Data Extraction
The following data were extracted and tabulated from each study:
1. Maternal dosage: the treatment dosage was usually specified in
mg/d. When the treatment dose was specified in mg/kg per day, the value was multiplied by 60 kg, the standard weight of an adult wom-an.30When the studies involved sev-eral patients who were taking dif-ferent therapeutic dosages, the range between the minimum and the maximum was reported in a table.
2. Number of mother–infant pairs for which pharmacokinetic data on drug excretion in breast milk were available was also reported.
3. Milk-to-plasma ratio (M/P): the con-centration of the drug in the moth-er’s milk divided by the concentra-tion of the drug in the mother’s plasma measured at the same mo-ment: milk concentration/plasma concentration⫽Cm/Cp. Table 1 re-ports the range between the mini-mum and maximini-mum M/P. When the studies reported the average con-centration of the drug in plasma and milk only or when a single de-termination of the drug was con-ducted, Table 1 indicates a single value.
4. Relative infant dosage (% dose): the daily dosage of drug received by an infant through breast milk, ex-pressed as a percentage of the weight-adjusted maternal daily dosage. It is calculated as follows30: (Cm[mg/mL]⫻900)/maternal daily dose (mg/kg)⫽%. When possible,
the percentage of drug received by the infant relative to the maternal dosage, as an interval between a minimum and maximum of the cal-culated values, was reported. When the study reported the average con-centration of the drug in milk or when a single determination of the drug in milk was conducted, a sin-gle value was indicated. When the study also reported the concentra-tion of the active metabolite(s) in milk, the values for drug and metab-olite(s) were added together in the equation.
5. Infant safety data: the incidence of adverse effects reported in breast-fed infants who were exposed to the drug through maternal breast milk, expressed as a ratio of number of breastfed infants, and the type of the observed effects.
Estimation of the Compatibility Level
The “compatibility level” of each drug with breastfeeding was estimated tak-ing into account the followtak-ing:
1. pharmacokinetic characteristics of the drug;
2. data on drug excretion in breast milk;
3. number of treatment days at sam-pling, according to acute and chronic administration; and
4. incidence and type of adverse ef-fects reported in breastfed infants.
Each drug was considered as follows:
● Compatible: the drug’s use during breastfeeding is considered safe because the relative infant dosage is ⬍10% of the maternal dosage30 and no relevant adverse effects were reported in breastfed infants.
● To be used with caution: the avail-able data do not allow an evaluation of the safety profile of the use of the drug during breastfeeding (eg, small number of mother–infant
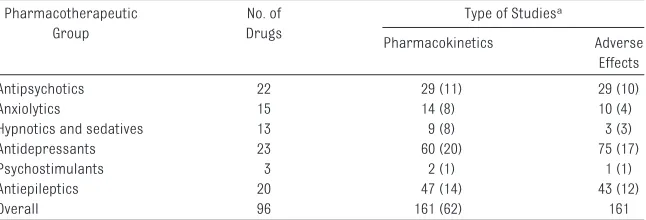
TABLE 1 Number of Articles Retrieved for Each Drug Group and Type of Information Pharmacotherapeutic
Group
No. of Drugs
Type of Studiesa
Pharmacokinetics Adverse Effects
Antipsychotics 22 29 (11) 29 (10)
Anxiolytics 15 14 (8) 10 (4)
Hypnotics and sedatives 13 9 (8) 3 (3)
Antidepressants 23 60 (20) 75 (17)
Psychostimulants 3 2 (1) 1 (1)
Antiepileptics 20 47 (14) 43 (12)
Overall 96 161 (62) 161
aThe total is⬎183 because some studies were both pharmacokinetic and adverse effects studies. Numbers in parentheses
pairs, relevant infant adverse ef-fects) or because of the possible ac-cumulation of the drug with pro-longed use (eg, benzodiazepines).
● Contraindicated: the drug’s use dur-ing breastfeeddur-ing is contraindi-cated because the relative infant dosage is ⬎10% of the maternal dosage and relevant adverse effects were reported in breastfed infants.
RESULTS
The bibliographic search produced 183 original articles that were eligible for analysis (Table 1). Documentation was available for 62 (65%) of 96 drugs; for the remaining 34 (35%) drugs, even the manufacturer was unable to pro-vide information on use during breast-feeding (Table 2). Twelve drugs re-sulted in exposure levels in breastfed infants that were higher than 10% of the maternal therapeutic dosages, and their use is therefore contraindicated (Table 3). These drugs were antiepilep-tics (7 of 14), anxiolyantiepilep-tics (1 of 8), selective serotonin reuptake inhibi-tors (SSRIs; 2 of 6), and antipsychotics (2 of 11). Adverse effects among breastfed infants were reported for 21 (34%) of 62 drugs (Table 4). Thus, for 34 psychotropic drugs, the informa-tion is unavailable, and for an addi-tional 15, their use is unsafe because of exposure dosage or observed ad-verse effects. A total of 19 (31%) psych-otropic drugs can be used during lac-tation according to an evidence-based
approach, whereas for 28 drugs, the available data do not allow an evalua-tion of their safety profile during breastfeeding.
Antidepressants
Among the drugs with available stud-ies on breastfeeding, antidepressants had a greater number of studies (SSRIs more than tricyclic antidepres-sant). For 20 (87%) of the 23 antide-pressants considered, 60 pharmacoki-netic studies (concerning a total of 342 mother–infant pairs) and 75 articles that reported infant adverse effects (31 reported of 612 monitored) were found. Data on use during breastfeed-ing were unavailable only for ademe-thionine, oxytriptan, and trimipramine.
In particular, among the antidepres-sants, sertraline, paroxetine, and flu-voxamine are the first-choice drugs for treatment of depression in breastfeed-ing mothers because they have the lowest degree of excretion into human breast milk. Considering the high rela-tive infant dosage, their long half-life, and the reported adverse effects in in-fants, the use of citalopram, escitalo-pram, and fluoxetine are contraindi-cated during breastfeeding.
SSRIs were better documented than tricyclic antidepressants, especially regarding their safety profile in breastfed infants; however, the major concern with exposing infants to SSRIs through breast milk is whether
long-term exposure to low dosages of these medications may have long-term neu-robehavioral effects. Most of the con-sidered studies were short-term stud-ies; there have been no studies on infants’ long-term exposure to very low dosages of antidepressants. Some studies, however, showed that the platelet serotonin uptake was not de-creased in breastfed infants who were exposed to sertraline or fluoxetine through breast milk. By inference, breastfeeding exposure to these drugs therefore should not affect serotonin metabolism in the infant brain; how-ever, this aspect needs additional in-vestigation.31,32In any case, if a mother wishes to breastfeed her infant while taking an SSRI, then she should be ad-vised to monitor the infant and to in-form the pediatricians promptly if the infant experiences sedation, nausea, reduced suckling, or other sign of drug toxicity.
Antipsychotics
Antipsychotics are the class with the smallest number of studies concern-ing use durconcern-ing breastfeedconcern-ing. For 11 (50%) of the 22 antipsychotics con-sidered, 29 pharmacokinetic studies (concerning a total of 146 mother– infant pairs) and 29 articles on infant adverse effects (11 reported of 162 monitored) were found.
Chlorpromazine and olanzapine could be considered the first-choice drugs for treatment of psychotic disorders in
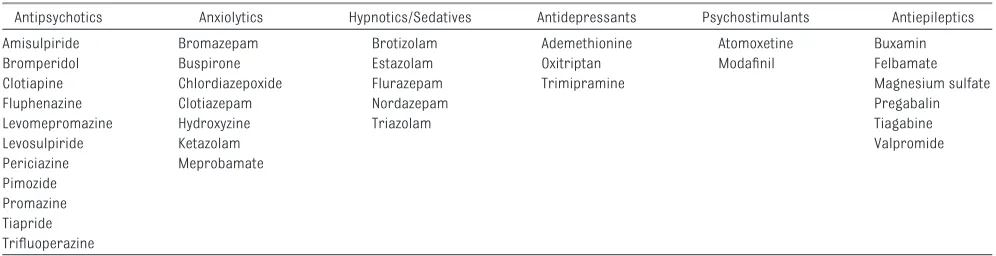
TABLE 2 Psychotropic Drugs Without Documentation on Their Profile During Breastfeeding
Antipsychotics Anxiolytics Hypnotics/Sedatives Antidepressants Psychostimulants Antiepileptics Amisulpiride Bromazepam Brotizolam Ademethionine Atomoxetine Buxamin
Bromperidol Buspirone Estazolam Oxitriptan Modafinil Felbamate
Clotiapine Chlordiazepoxide Flurazepam Trimipramine Magnesium sulfate
Fluphenazine Clotiazepam Nordazepam Pregabalin
Levomepromazine Hydroxyzine Triazolam Tiagabine
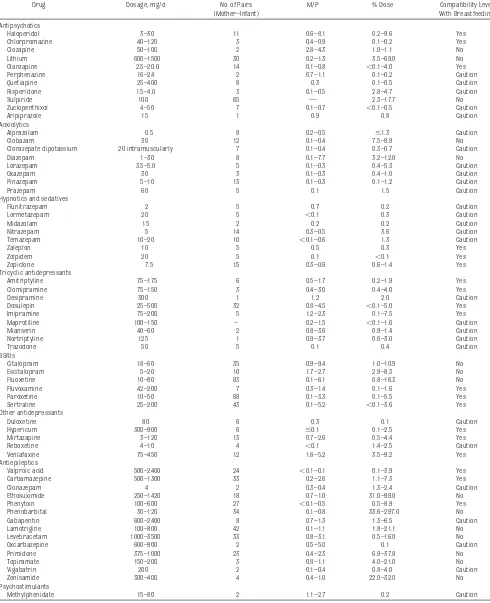
TABLE 3 Drug Excretion Into Breast Milk
Drug Dosage, mg/d No. of Pairs
(Mother–Infant)
M/P % Dose Compatibility Level
With Breastfeeding
Antipsychotics
Haloperidol 3–30 11 0.6–8.1 0.2–9.6 Yes
Chlorpromazine 40–120 3 0.4–0.9 0.1–0.2 Yes
Clozapine 50–100 2 2.8–4.3 1.0–1.1 No
Lithium 600–1500 30 0.2–1.3 3.5–69.0 No
Olanzapine 2.5–20.0 14 0.1–0.8 ⬍0.1–4.0 Yes
Perphenazine 16–24 2 0.7–1.1 0.1–0.2 Caution
Quetiapine 25–400 8 0.3 0.1–0.5 Caution
Risperidone 1.5–4.0 3 0.1–0.5 2.8–4.7 Caution
Sulpiride 100 65 — 2.3–17.7 No
Zuclopenthixol 4–50 7 0.1–0.7 ⬍0.1–0.5 Caution
Aripiprazole 15 1 0.9 0.8 Caution
Anxiolytics
Alprazolam 0.5 8 0.2–0.5 ⱕ1.3 Caution
Clobazam 30 12 0.1–0.4 7.5–9.9 No
Clorazepate dipotassium 20 intramuscularly 7 0.1–0.4 0.3–0.7 Caution
Diazepam 1–30 8 0.1–7.7 3.2–12.0 No
Lorazepam 3.5–5.0 5 0.1–0.3 0.4–5.3 Caution
Oxazepam 30 3 0.1–0.3 0.4–1.0 Caution
Pinazepam 5–10 13 0.1–0.3 0.1–1.2 Caution
Prazepam 60 5 0.1 1.5 Caution
Hypnotics and sedatives
Flunitrazepam 2 5 0.7 0.2 Caution
Lormetazepam 20 5 ⬍0.1 0.3 Caution
Midazolam 15 2 0.2 0.2 Caution
Nitrazepam 5 14 0.3–0.5 3.6 Caution
Temazepam 10–20 10 ⬍0.1–0.6 1.3 Caution
Zaleplon 10 5 0.5 0.3 Yes
Zolpidem 20 5 0.1 ⬍0.1 Yes
Zopiclone 7.5 15 0.3–0.6 0.6–1.4 Yes
Tricyclic antidepressants
Amitriptyline 75–175 6 0.5–1.7 0.2–1.9 Yes
Clomipramine 75–150 3 0.4–3.0 0.4–4.0 Yes
Desipramine 300 1 1.2 2.0 Caution
Dosulepin 25–500 32 0.8–4.5 ⬍0.1–5.0 Yes
Imipramine 75–200 5 1.2–2.3 0.1–7.5 Yes
Maprotiline 100–150 – 0.2–1.5 ⬍0.1–1.6 Caution
Mianserin 40–60 2 0.8–3.6 0.9–1.4 Caution
Nortriptyline 125 1 0.9–3.7 0.6–3.0 Caution
Trazodone 50 5 0.1 0.4 Caution
SSRIs
Citalopram 18–60 35 0.9–9.4 1.0–10.9 No
Escitalopram 5–20 10 1.7–2.7 2.9–8.3 No
Fluoxetine 10–80 83 0.1–6.1 0.8–16.3 No
Fluvoxamine 42–200 7 0.3–1.4 0.1–1.6 Yes
Paroxetine 10–50 68 0.1–3.3 0.1–5.5 Yes
Sertraline 25–200 43 0.1–5.2 ⬍0.1–3.6 Yes
Other antidepressants
Duloxetine 80 6 0.3 0.1 Caution
Hypericum 300–900 6 ⱕ0.1 0.1–2.5 Yes
Mirtazapine 3–120 13 0.7–2.6 0.5–4.4 Yes
Reboxetine 4–10 4 ⬍0.1 1.4–2.5 Caution
Venlafaxine 75–450 12 1.6–5.2 3.5–9.2 Yes
Antiepileptics
Valproic acid 500–2400 24 ⬍0.1–0.1 0.1–3.9 Yes
Carbamazepine 500–1300 33 0.2–2.6 1.1–7.3 Yes
Clonazepam 4 2 0.3–0.4 1.3–2.4 Caution
Ethosuximide 250–1420 18 0.7–1.0 31.0–99.0 No
Phenytoin 100–600 27 ⬍0.1–0.5 0.5–8.9 Yes
Phenobarbital 30–120 34 0.1–0.8 33.6–297.0 No
Gabapentin 600–2400 8 0.7–1.3 1.3–6.5 Caution
Lamotrigine 100–800 42 0.1–1.1 1.8–21.1 No
Levetiracetam 1000–3500 33 0.8–3.1 0.5–16.0 No
Oxcarbazepine 600–900 2 0.5–5.0 0.1 Caution
Primidone 375–1000 23 0.4–2.3 6.9–37.8 No
Topiramate 150–200 3 0.8–1.1 4.0–21.0 No
Vigabatrin 200 2 0.1–0.4 0.8–4.0 Caution
Zonisamide 300–400 4 0.4–1.0 22.0–32.0 No
Psychostimulants
Methylphenidate 15–80 2 1.1–2.7 0.2 Caution
breastfeeding mothers because they have the lowest degree of excretion into human breast milk and scant ad-verse effects in breastfed infants. Con-sidering the high relative infant dos-age and the reported adverse effects in infants, the use of clozapine, lithium, and sulpiride is contraindicated dur-ing breastfeeddur-ing.
Because psychosis requires long-term treatment and because the data on safety of antipsychotics dur-ing lactation are limited, the benefits of breastfeeding may be weighed against the potential risks of med-ication. All antipsychotic drugs are sedating and have relatively long half-lives, so the infants should be observed for lethargy, sedation, and appropriate development.
Hypnotics and Anxiolytics
The available data regarding the use of hypnotic and anxiolytic agents during breastfeeding are scant. For 16 (57%) of the 28 hypnotics and anxiolytics con-sidered, 23 pharmacokinetic studies (concerning a total of 122 mother– infant pairs) and 13 articles on infant adverse effects (6 reported of 57 mon-itored) were retrieved. The available data suggest that the amounts of these medications to which the nursing in-fant is exposed are not very high; how-ever, they must be used with caution by breastfeeding mothers, taking into account that neonates metabolize ben-zodiazepines more slowly than adults and that these drugs are usually used for long-term periods, so they may ac-cumulate in breastfed infants and pro-duce infant sedation, nausea, and poor feeding.
The use of long-acting benzodiaz-epines, such as diazepam and cloba-zam, is therefore contraindicated in breastfeeding mothers. If a benzodiaz-epine is needed during breastfeeding, then a short-acting one, such as midazolam, oxazepam, pinazepam, or
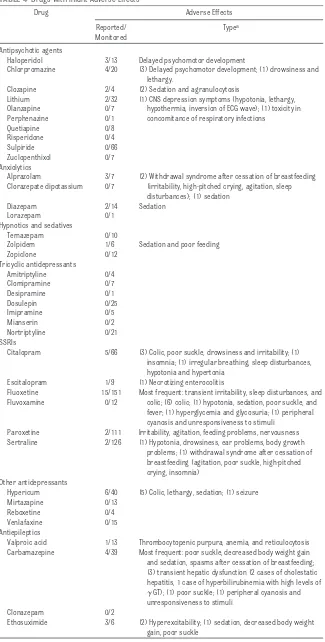
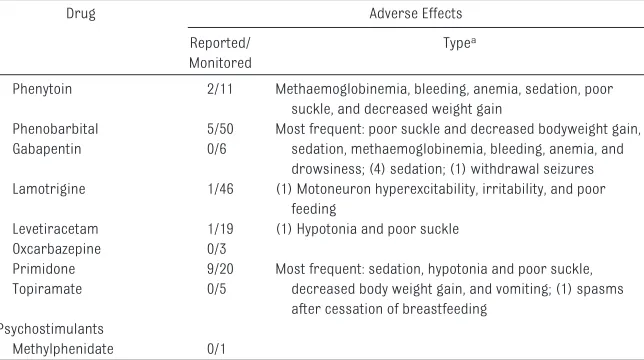
TABLE 4 Drugs With Infant Adverse Effects
Drug Adverse Effects
Reported/ Monitored
Typea
Antipsychotic agents
Haloperidol 3/13 Delayed psychomotor development
Chlorpromazine 4/20 (3) Delayed psychomotor development; (1) drowsiness and lethargy.
Clozapine 2/4 (2) Sedation and agranulocytosis
Lithium 2/32 (1) CNS depression symptoms (hypotonia, lethargy, Olanzapine 0/7 hypothermia, inversion of ECG wave); (1) toxicity in Perphenazine 0/1 concomitance of respiratory infections
Quetiapine 0/8
Risperidone 0/4
Sulpiride 0/66
Zuclopenthixol 0/7 Anxiolytics
Alprazolam 3/7 (2) Withdrawal syndrome after cessation of breastfeeding Clorazepate dipotassium 0/7 (irritability, high-pitched crying, agitation, sleep
disturbances); (1) sedation Diazepam 2/14 Sedation
Lorazepam 0/1
Hypnotics and sedatives
Temazepam 0/10
Zolpidem 1/6 Sedation and poor feeding
Zopiclone 0/12
Citalopram 5/66 (3) Colic, poor suckle, drowsiness and irritability; (1) insomnia; (1) irregular breathing, sleep disturbances, hypotonia and hypertonia
Escitalopram 1/9 (1) Necrotizing enterocolitis
Fluoxetine 15/151 Most frequent: transient irritability, sleep disturbances, and Fluvoxamine 0/12 colic; (6) colic; (1) hypotonia, sedation, poor suckle, and
fever; (1) hyperglycemia and glycosuria; (1) peripheral cyanosis and unresponsiveness to stimuli
Paroxetine 2/111 Irritability, agitation, feeding problems, nervousness Sertraline 2/126 (1) Hypotonia, drowsiness, ear problems, body growth
problems; (1) withdrawal syndrome after cessation of breastfeeding (agitation, poor suckle, high-pitched crying, insomnia)
Other antidepressants
Hypericum 6/40 (5) Colic, lethargy, sedation; (1) seizure Mirtazapine 0/13
Reboxetine 0/4
Venlafaxine 0/15 Antiepileptics
Valproic acid 1/13 Thrombocytopenic purpura, anemia, and reticulocytosis Carbamazepine 4/39 Most frequent: poor suckle, decreased body weight gain and sedation, spasms after cessation of breastfeeding; (3) transient hepatic dysfunction (2 cases of cholestatic hepatitis, 1 case of hyperbilirubinemia with high levels of
␥GT); (1) poor suckle; (1) peripheral cyanosis and unresponsiveness to stimuli
Clonazepam 0/2
lormetazepam, should be used. More-over, the minimum dosage required for symptom relief should be used, and the infant should be monitored regu-larly. If an infant experiences sedation, nausea, reduced suckling, or other signs of toxicity, then breastfeeding should be discontinued. Single doses of benzodiazepines do not require any limitation on breastfeeding.
Antiepileptics
The antiepileptic therapeutic group is the most investigated during breast-feeding. Data are available for 14 (70%) of the 20 drugs considered: 47 pharmacokinetic studies (concerning a total of 255 mother–infant pairs) and 43 articles on infant adverse effects (26 reported of 220 monitored) were found.
Valproic acid and carbamazepine are the first-choice drugs for treatment of mothers with epilepsy during breast-feeding because of their low degree of excretion into human breast milk and limited reported adverse effects in fants. Considering the high relative in-fant dosage and the reported adverse effects in infants, the use of 6 drugs (ethosuximide, phenobarbital, lam-otrigine, primidone, topiramate, and
zonisamide) is contraindicated during breastfeeding.
Because antiepileptics are used in long-term treatment, the most appro-priate therapy in childbearing women with epilepsy should be evaluated be-fore pregnancy and during the breast-feeding period considering the poten-tial harm of the medication on the fetus and breastfed newborn. If the mother is on therapy with 1 of the con-traindicated drugs (eg, phenobarbi-tal), then the infant should be ob-served for lethargy, sedation, and appropriate development. Although the routine monitoring of infant serum drug levels is not warranted, the infant serum can also be assayed to assess actual neonatal exposure to medica-tion more accurately.
Psychostimulants
Studies are available only for methyl-phenidate (2 studies on pharmacoki-netics in 2 pairs and no adverse effects in 1 infant). Methylphenidate shows an M/P that varies from 1.1 to 2.7 and a relative infant dosage that is 0.2% of the maternal dosage; however, the available information is too scant to permit an evaluation of the safety pro-file of the drug.
DISCUSSION
No data are available on the use during breastfeeding of one third of psycho-tropic drugs. For the other two thirds, available information varies widely. Al-though many psychotropic drugs are considered safe during breastfeeding because they are excreted to a low ex-tent into breast milk (relative infant dosage ⬍10% of the therapeutic ma-ternal dosage) and no serious adverse events related to exposure to these medications through breast milk have been reported, there are documented differences between drugs within the same class and there is no class action in relation to breastfeeding. Further-more, for each therapeutic category, there are drugs with minimal infant ex-posure via breastfeeding. For these drugs, the dosage to which the infant is exposed is very low and well below what would be expected to have any significant clinical effects. For this rea-son, they are considered first choice for the treatment of breastfeeding mothers (sertraline, chlorpromazine, lormetazepam, and carbamazepine), whereas a few drugs are contraindi-cated (citalopram, clozapine, diaze-pam, and phenobarbital).
Although antiepileptics and antide-pressants have been studied exten-sively, to date, less information re-garding the use of antipsychotics, anxiolytics and hypnotics, and psycho-stimulants while breastfeeding is available. The existing literature is of-ten limited to a small number of stud-ies based on a few cases or case re-ports, making it difficult to formulate any generalizations regarding their safety profile in lactation.26–29 These drugs are being used more frequently and need additional investigation.
Mothers are increasingly encouraged to nurse, but breastfeeding while tak-ing psychotropic medications is an im-portant issue that has not received the attention that it deserves.29 Women TABLE 4 Continued
Drug Adverse Effects
Reported/ Monitored
Typea
Phenytoin 2/11 Methaemoglobinemia, bleeding, anemia, sedation, poor suckle, and decreased weight gain
Phenobarbital 5/50 Most frequent: poor suckle and decreased bodyweight gain, Gabapentin 0/6 sedation, methaemoglobinemia, bleeding, anemia, and
drowsiness; (4) sedation; (1) withdrawal seizures Lamotrigine 1/46 (1) Motoneuron hyperexcitability, irritability, and poor
feeding
Levetiracetam 1/19 (1) Hypotonia and poor suckle Oxcarbazepine 0/3
Primidone 9/20 Most frequent: sedation, hypotonia and poor suckle, Topiramate 0/5 decreased body weight gain, and vomiting; (1) spasms
after cessation of breastfeeding Psychostimulants
Methylphenidate 0/1
References are available upon request to the corresponding author. CNS indicates central nervous system; ECG, electrocardiogram.
with postpartum psychiatric disorders are understandably anxious about any uncertainties surrounding the safety of their medications in their infants and often face the dilemma of whether to use psychotropic medication while continuing to breastfeed their infants. Quite often, the first reaction is to stop breastfeeding or to stop any psycho-tropic medications entirely. Moreover, many physicians have been hesitant to prescribe psychotropic medication to women who choose to breastfeed. What is easily forgotten are the risks of untreated psychiatric disorders in the postpartum period.33In such cases, it is important to safeguard the mental health of the mother while at the same time optimizing the emotional and physical well-being of the infant.34In general, these medications should not be prescribed without careful consid-eration, but neither should they be au-tomatically avoided.
The decision to prescribe psychotropic agents to breastfeeding mothers should depend on an individual risk/ benefit analysis: the known benefits of breastfeeding and medication use for both mother and infant must be weighed against the risk of untreated maternal illness or the risk of infant exposure to medications through breast milk.35 There are immediate risks (eg, hypersensitivity reactions, adverse central nervous system ef-fects such as lethargy and reduced feeding) and risks of long-term effects on the developing brain.28This analysis requires up-to-date knowledge on safety of psychotropic medication use during breastfeeding.24
The strength of this review is the systematic approach used to collect the available information on psycho-tropic medication use during breast-feeding. The result is a more com-plete, accurate, and updated review of the evidence, and this can repre-sent an important tool for health
pro-fessionals for promoting the rational use of psychotropic drugs in breast-feeding mothers. The major objective of this review is to be a reliable source of evidence-based informa-tion for current problems in daily clin-ical practice, especially for psychia-trists, pediatricians, family physicians, and obstetrician-gynecologists, who often play an important role in wom-en’s decision to start or continue breastfeeding while taking psycho-tropic medications.
If treatment is deemed appropriate, then the smallest number of medica-tions at the lowest possible dosage consistent with control of the mental illness should be prescribed,17and a drug with a proven favorable safety/ efficacy profile should be preferred.24 All psychotropic drugs are excreted into breast milk, but concentrations and effects may vary considerably. The amount of medication to which an in-fant is exposed through lactation de-pends on several factors: the maternal dosage, frequency of dosing, rate of absorption into maternal circulation, diffusion from maternal circulation into breast milk, rate of maternal drug metabolism, and absorption of the drug by the infant. Moreover, the fre-quency and timing of the feedings can influence the amount of drug to which the nursing infant is exposed. By re-stricting breastfeeding to times during which breast milk drug concentra-tions would be at their lowest levels or by taking medication immediately af-ter breastfeeding, the infant exposure to the drug may be reduced. As with all drugs taken while breastfeeding, it is prudent to monitor carefully the clini-cal status of infants for signs of drug-related toxicity and adverse effects (generally sedation; irritability; and changes to sleep, feeding, and growth). It is also essential that moth-ers be properly educated about this matter and advised to discontinue a
medication if their infant develops signs of toxicity or adverse effects.20In this setting, ongoing collaboration with the pediatrician is crucial.
If a mother is on therapy with 1 of the contraindicated drugs because she is affected by postpartum affective ill-ness that responds only to a particular drug (this is common for epilepsy), then it is advisable to keep her on that drug rather than to switch. In addition, the woman should be kept on the low-est possible effective dosage of medi-cation, and the infant should be ob-served for possible adverse effects. Although the routine monitoring of in-fant serum drug levels is not war-ranted, if neonatal toxicity related to drug exposure through breast milk is suspected or when the mother is nurs-ing while taknurs-ing a drug that is contra-indicated during breastfeeding, then infant serum can also be assayed to assess neonatal exposure to medica-tion more accurately.37
CONCLUSIONS
completely free of adverse effects. All psychotropic drugs should be viewed with caution during breastfeeding, tak-ing into account the known benefits of
breastfeeding to mothers and infants as well as the possibility that infant ex-posure to clinically significant levels in breast milk may occur.
ACKNOWLEDGMENT
We thank Dr Benedetta Schiavetti for help with the preparation of this article.
REFERENCES
1. Ip S, Chung M, Raman G, et al. Breastfeeding and maternal and infant health outcomes in devel-oped countries.Evid Rep Technol Assess (Full Rep).2007;(153):1–186
2. Hoddinott P, Tappin D, Wright C. Breast feeding.BMJ.2008;336(7649):881– 887
3. WHO Collaborative Study Team on the Role of Breastfeeding on the Prevention of Infant Mortality. Effect of breastfeeding on infant and child mortality due to infectious diseases in less developed countries: a pooled analysis.Lancet.2000;355(9202):451– 455
4. Horta BL, Bahl R, Martines JC, Victora CG.Evidence on the Long-term Effects of Breastfeeding. Systematic Reviews and Meta-analyses. Geneva, Switzerland: World Health Organization; 2007. Available at: http://libdoc.who.int/publications/2007/9789241595230㛭eng.pdf. Accessed April 8, 2009
5. Melton LJ, Bryant SC, Wahner HW, et al. Influence of breastfeeding and other reproductive factors on bone mass later in life.Osteoporos Int.1993;3(2):76 – 83
6. Danforth KN, Tworoger SS, Hecht JL, Rosner BA, Colditz GA, Hankinson SE. Breastfeeding and risk of ovarian cancer in two prospective cohorts.Cancer Causes Control.2007;18(5):517–523 7. Gartner LM, Morton J, Lawrence RA, et al. Breastfeeding and the use of human milk.Pediatrics.
2005;115(2):496 –506
8. WHO/UNICEF.Global Strategy for Infant and Young Child Feeding. Geneva, Switzerland: World Health Organization; 2003. Available at: www.who.int/nutrition/publications/gs㛭infant㛭feeding㛭
text㛭eng.pdf. Accessed April 8, 2009
9. Ito S. Drug therapy for breast-feeding women.N Engl J Med.2000;343(2):118 –126
10. Stultz EE, Stokes JL, Shaffer ML, Paul IM, Berlin CM. Extent of medication use in breastfeeding women.Breastfeed Med.2007;2(3):145–151
11. Schirm E, Schwagermann MP, Tobi H, de Jong-van den Berg LT. Drug use during breastfeeding: a survey from the Netherlands.Eur J Clin Nutr.2004;58(2):386 –390
12. Spencer JP, Gonzalez LS 3rd, Barnhart DJ. Medications in the Breast-feeding mother.Am Fam Physician.2001;64(1):119 –126
13. Ito S, Liau M, Chan W, Koren G. Maternal drug therapy as a risk factor for shorter duration of breastfeeding.Paediatr Perinat Drug Ther.1999;3(1):44 – 48
14. Bonati M, Addis A. Informing women about drugs they take during pregnancy: promoting consum-ers’ drug information as integral part of care.Pharm World Sci.1998;20(6):236 –237
15. Usher K, Foster K. The use of psychotropic medications with breastfeeding women: applying the available evidence.Contemp Nurse.2006;21(1):94 –102
16. De Las Cuevas C, de la Rosa MA, Troyano JM, Sanz EJ. Are psychotropic drugs used in pregnancy?
Pharmacoepidemiol Drug Saf.2007;16(9):1018 –1023
17. Li D, Liu L, Odouli R. Presence of depressive symptoms during early pregnancy and the risk of preterm delivery: a prospective cohort study.Hum Reprod.2009;24(1):146 –153
18. Dossett EC. Perinatal depression.Obstet Gynecol Clin North Am.2008;35(3):419 – 434, viii 19. Stein A, Malmberg LE, Sylva K, Barnes J, Leach P, FCCC team. The influence of maternal depression,
caregiving, and socioeconomic status in the postnatal year on children’s language development.
Child Care Health Dev.2008;34(5):603– 612
20. Menon SJ. Psychotropic medication during pregnancy and lactation.Arch Gynecol Obstet.2008; 277(1):1–13
21. Musters C, McDonald E, Jones I. Management of postnatal depression.BMJ.2008;337:a736 22. Addis A, Impicciatore P, Miglio D, Colombo F, Bonati M, Da Silva CD. Drug use in pregnancy and
lactation: the work of a regional drug information center.Ann Pharmacother.1995;29(6):632– 633 23. Jain AE, Lacy T. Psychotropic drugs in pregnancy and lactation.J Psychiatr Pract.2005;11(3):
177–191
25. Gavin NI, Gaynes BN, Lohr KN, Meltzer-Brody S, Gartlehner G, Swinson T. Perinatal depression: a systematic review of prevalence and incidence.Obstet Gynecol.2005;106(5 pt 1):1071–1083 26. Usher K, Foster K, McNamara P. Antipsychotic drugs and pregnant or breastfeeding women: the
issues for mental health nurses.J Psychiatr Ment Health Nurs.2005;12(6):713–718
27. Gentile S. Prophylactic treatment of bipolar disorder in pregnancy and breastfeeding: focus on emerging mood stabilizers.Bipolar Disord.2006;8(3):207–220
28. Sivertz K, Kostaras X. The use of psychotropic medications in pregnancy and lactation.B C Med J.
2005;47(3):135–138
29. Kohen D. Psychotropic medication and breastfeeding.Adv Psychiatr Treat.2005;11:371–379 30. Bennett PN. Use of the monograph on drugs. In: Bennett PN.Drugs and Human Lactation.2nd ed.
Amsterdam, Netherlands: Elsevier; 1996:67–74
31. Epperson N, Czarkowski KA, Ward-O’Brien D, Weiss E, Gueorguieva R, Jatlow P, Anderson GM. Maternal sertraline treatment and serotonin transport in breast-feeding mother-infant pairs.
Am J Psychiatry.2001;158(10):1631–1637
32. Epperson N, Jatlow PI, Czarkowski K, Anderson GM. Maternal fluoxetine treatment in the postpar-tum period: effects on platelet serotonin and plasma drug levels in breastfeeding mother-infant pairs.Pediatrics.2003;112(5). Available at: www.pediatrics.org/cgi/content/full/112/5/e425 33. Turner KM, Sharp D, Folkes L, Chew-Graham C. Women’s views and experiences of antidepressants
as a treatment for postnatal depression: a qualitative study.Fam Pract.2008;25(6):450 – 455 34. Rubin ET, Lee A, Ito S. When breastfeeding mothers need CNS-acting drugs.Can J Clin Pharmacol.
2004;11(2):e257– e266
35. Einarson A, Portnoi G, Koren G. Update on motherisk updates: seven years of questions and answers. Can Fam Physician. 2002;48:1301–1304
36. Burt VK, Suri R, Altshuler L, Stowe Z, Hendrick VC, Muntean E. The use of psychotropic medications during breast-feeding.Am J Psychiatry.2001;158(7):1001–1009
DOI: 10.1542/peds.2009-0326
2009;124;e547-e556; originally published online Sep 7, 2009;
Pediatrics
& Services
Updated Information
http://www.pediatrics.org/cgi/content/full/124/4/e547 including high-resolution figures, can be found at:
References
http://www.pediatrics.org/cgi/content/full/124/4/e547#BIBL at:
This article cites 32 articles, 11 of which you can access for free
Subspecialty Collections
logy
http://www.pediatrics.org/cgi/collection/therapeutics_and_toxico Therapeutics & Toxicology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtml tables) or in its entirety can be found online at:
Information about reproducing this article in parts (figures,
Reprints
http://www.pediatrics.org/misc/reprints.shtml