2010
AsiA PAcific
strAtegy
for emerging
DiseAses
2010
AsiA PAcific
strAtegy
for emerging
DiseAses
WHO Library Cataloguing in Publicaion Data
Asia Paciic Strategy for emerging diseases : 2010
1. Communicable diseases, Emerging – prevenion and control. I. World Health Organizaion. Regional Oice for the Western Paciic. II. World Health Organizaion. Regional Oice for South-East Asia.
ISBN 978 92 9061 504 0 (NLM Classiicaion: WA 110 )
© World Health Organizaion 2011
All rights reserved. Publicaions of the World Health Organizaion can be obtained from WHO Press, World Health Organizaion, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publicaions – whether for sale or for noncommercial distribuion – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). For WHO Western Paciic Regional Publicaions, request for permission to reproduce should be addressed to the Publicaions Oice, World Health Organizaion, Regional Oice for the Western Paciic, P.O. Box 2932, 1000, Manila, Philippines (fax +63 2 521 1036; e-mail: [email protected]).
The designaions employed and the presentaion of the material in this publicaion do not imply the expression of any opinion whatsoever on the part of the World Health Organizaion concerning the legal status of any country, territory, city or area or of its authoriies, or concerning the delimitaion of its froniers or boundaries. Doted lines on maps represent approximate border lines for which there may not yet be full agreement.
The menion of speciic companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organizaion in preference to others of a similar nature that are not menioned. Errors and omissions excepted, the names of proprietary products are disinguished by iniial capital leters.
Table of ConTenTs 3 5 7 9 10 10 11 11 12 13 13 14 14 14 15 16 18 20 22 23 26 33 34 37 39 39 41 42 43 48 49
Foreword . . . .
Execuive Summary . . . .
SECTION 1: Introducing the Strategy . . . .
1.1 Scope . . . . 1.2 Intended audiences . . . . 1.3 Guiding principles . . . . 1.4 Use of the Strategy . . . . 1.5 Time frame and targeted outcomes . . . .
SECTION 2: Vision, Goal and Objecives . . . .
2.1 Vision . . . . 2.2 Goal . . . . 2.3 Objecives . . . . 2.4 Focus areas . . . .
SECTION 3: Focus Areas and Acions . . . .
3.1 Surveillance, risk assessment and response . . . . 3.2 Laboratory . . . . 3.3 Zoonoses . . . . 3.4 Infecion prevenion and control . . . . 3.5 Risk communicaions . . . . 3.6 Public health emergency preparedness . . . . 3.7 Regional preparedness, alert and response . . . . 3.8 Monitoring and evaluaion . . . .
SECTION 4: Special Situaions and Approaches . . . .
SECTION 5: Implemening the Strategy . . . .
5.1 Regional coordinaion and management model . . . . 5.2 Naional-level mechanisms . . . . 5.3 Financial resource mobilizaion . . . .
ANNEX 1: Process of Developing APSED (2010) . . . .
ANNEX 2: Glossary of Selected Terms . . . .
ANNEX 3: Important Reference Documents . . . .
ABBREVIATIONS AND ACRONYMS
APSED Asia Paciic Strategy for Emerging Diseases
CBRN chemical, biological, radiological and nuclear
EBS event-based surveillance
EIS (IHR) Event Informaion Site
EQA external quality assurance
FET ield epidemiology training
GOARN Global Outbreak Alert and Response Network
IBS indicator-based surveillance
IHR Internaional Health Regulaions
INFOSAN Internaional Food Safety Authoriies Network
IPC infecion prevenion and control
IQC internal quality control
M&E monitoring and evaluaion
NFP Naional IHR Focal Point
PHEIC public health emergency of internaional concern
POE points of entry
PPE personal protecive equipment
RRT rapid response team
TAG Technical Advisory Group
foRewoRd 55
Foreword
The Asia Paciic Strategy for Emerging Diseases (APSED) was developed in 2005 to meet the challenges of emerging diseases that pose serious threats to regional and global health security. It provided a common framework to strengthen naional and regional capaciies to manage emerging diseases, improve pandemic preparedness and comply with the core capacity requirements of the Internaional Health Regulaions (2005).
Implementaion of APSED over the past ive years in the 11 countries that comprise the WHO South-East Asia Region and 37 countries and areas that make up the WHO Western Paciic Region provided important lessons in pandemic response and demonstrated the need to further strengthen public health emergency preparedness and improve monitoring and evaluaion.
The Asia Paciic Technical Advisory Group on Emerging Infecious Diseases, at its fourth annual meeing in July 2009, reviewed the signiicant achievements obtained in the ive priority areas ideniied in the original strategy: surveillance and response; laboratory; zoonoses; infecion control; and risk communicaions. The Technical Advisory Group recommended that APSED be updated to enhance the gains already achieved in the original ive priority areas and use the achievements as a foundaion to address a wider range of acute public health threats.
The recommendaion of the Technical Advisory Group led to a series of intensive country-level assessments and discussions, as well as a biregional consultaion that brought together regional and global experts, along with public health oicials from various Member States. Those assessments and consultaions led to a drat APSED (2010) in which three new focus areas have been added: public health emergency preparedness; regional preparedness, alert and response; and monitoring and evaluaion. The drat APSED (2010) was reviewed and endorsed by the Technical Advisory Group at its ith annual meeing in July 2010.
The development of the original APSED in 2005 was greatly inluenced by several events in the Asia Paciic Region, including the emergence of severe acute respiratory syndrome (SARS) and avian inluenza A(H5N1), and also by the adopion of the Internaional Health Regulaions (2005).
The past ive years have also led to a greater appreciaion of the need to acknowledge and strengthen links among agencies responsible for confroning acute public health threats. These include animal health authoriies, departments concerned with the response to humanitarian emergencies, and those tasked with food, chemical and radiological safety. APSED (2010) aims to establish stronger links among these related public health programmes, thereby ensuring a joint approach to preparedness and response to all public health emergencies.
We all recognize that regional and global public health security cannot be achieved without strong mechanisms for internaional cooperaion. One of the great successes of APSED and its alignment with the Internaional Health Regulaions (2005) has been the ability to draw together a wide range of partners, including Member States, donors, mulilateral organizaions and technical agencies. By engaging with all partners in this way and working towards a common vision, we also build regional solidarity, resilience and self-reliance.
We coninue this journey in the atermath of pandemic inluenza (H1N1) 2009, which although not as severe as iniially feared, tested public health and health care systems, revealing strengths and weaknesses but also providing opportuniies to learn lessons and to improve our preparedness for future pandemic threats.
We certainly will coninue to face new challenges as we move forward. But we can do so knowing that a strong foundaion has been established, and that, thanks to the updated Asia Paciic Strategy for Emerging Diseases, we have a clear direcion for the future.
Samlee Plianbangchang, M.D., Dr.P.H. Shin Young-soo, M.D., Ph.D.
Regional Director Regional Director South-East Asia Region Western Paciic Region
exeCUTIve sUmmaRy 77
Executive Summary
In recent years, the Asia Paciic region has been an epicentre for emerging diseases, resuling in signiicant impacts on health, social and economic development. Protecing the region from acute public health threats is, therefore, a top priority. The Asia Paciic Strategy for Emerging Diseases (APSED) was launched in 2005 as a common strategic framework for countries and areas of the region to strengthen their capacity to manage and respond to emerging disease threats, including inluenza pandemics. In June 2007, the revised Internaional Health Regulaions (2005), known as IHR (2005), entered into force, calling upon countries and the World Health Organizaion (WHO) to strengthen their core capaciies to detect, report and respond to acute public health events in order to build a global public health defence system. APSED serves as a road map to guide all countries in the region towards meeing the IHR (2005) core capacity requirements, thus ensuring regional and global health security.
Over the past ive years, considerable progress has been made in the development and strengthening of the required core capaciies. Incorporaing recommendaions from Member States and learning from experiences in implemening the original Asia Paciic Strategy for Emerging Diseases, which was jointly developed by the WHO South-East Asia Region and the WHO Western Paciic Region, as well as the response to pandemic inluenza (H1N1) 2009, an updated strategy, APSED (2010), has been developed. APSED (2010) will be implemented by building on the achievements of the original APSED, while recognizing variaions in exising capacity levels across countries. It is intended that APSED (2010) will further support progress towards meeing IHR (2005) obligaions and consolidate gains already made in establishing collecive regional public health security. While APSED (2010) coninues to focus on emerging diseases, it also seeks to maximize the beneits already achieved by widening its scope to include other acute public health threats and by idenifying addiional areas of synergy and special situaions to which the Strategy can make important contribuions.
APSED (2010) has expanded its scope to include eight “focus areas”: (1) surveillance, risk assessment and response;
(2) laboratories; (3) zoonoses;
(4) infecion prevenion and control; (5) risk communicaions;
(7) regional preparedness, alert and response; and (8) monitoring and evaluaion.
Focus areas 1 to 6 concentrate on naional and local capacity-building, focus area 7 addresses WHO regional capacity, and focus area 8 covers both naional and regional monitoring and evaluaion of APSED (2010) implementaion.
While APSED (2010) is a common framework for all countries and areas, the individual situaion and context in each of the 48 countries and areas of the Asia Paciic region must be considered when implemening the Strategy. This will require countries to develop individual APSED implementaion plans to suit their own context and needs.
The intended audience for APSED (2010) is expected to be ministries of health, agencies working on emerging diseases in animal health sectors, food safety authoriies and departments concerned with the management of other public health emergencies. Development agencies, donors and other partners are also strongly encouraged to use this framework to prioriize support to countries and thus maximize eicient use of resources.
In considering how APSED (2010) will be implemented, the collecive and coordinated acions of Member States, technical experts, WHO and partners will be essenial in ensuring that the goals and objecives are achieved. A mulisectoral approach is most likely to enhance coordinaion, collaboraion and harmonizaion among muliple naional and regional stakeholders. It is of criical importance that capacity-building is supported by sustainable inancing mechanisms and adequate human resources. Thus, countries and partners will be requested to develop and support a strategic approach to mobilizing the necessary resources to implement the Strategy at country and regional levels.
seCTIon 1: InTRodUCInG THe sTRaTeGy 99
SECTION 1: Introducing the Strategy
The Asia Paciic region is home to about 3.4 billion people, more than half of the world’s populaion. With 48 countries and areas, the region is one of the most diverse in terms of culture, socioeconomic and development status, climate and geography. In recent years, the region has been an epicentre of signiicant disease outbreaks and public health events that have impacted not only health but also society, human security and economic growth. Protecing the region from acute public health threats is thus a top priority.
Public health events regularly occur in the Asia Paciic region, with about one public health event every two to three days detected and monitored by regional surveillance systems. With increasing travel, trade and mobility of people worldwide, emerging diseases and public health threats can easily cross internaional borders, moving from one populaion to another. Thus, truly efecive regional public health security can only be achieved if collecive acions are in place in the region. The unpredictable nature of outbreak-prone diseases and the need for a collecive approach has clearly been demonstrated by severe acute respiratory syndrome (SARS), avian inluenza and more recently pandemic inluenza (H1N1) 2009.
The Asia Paciic Strategy for Emerging Diseases (APSED) was launched in 2005 as a common strategic framework for countries and areas of the region to strengthen their capacity to manage and respond to emerging diseases including epidemic-prone diseases. In June 2007, the revised Internaional Health Regulaions (2005), known as IHR (2005), entered into force and called upon countries and WHO to strengthen their capaciies to detect, report and respond to acute public health events in order to build a global public health defence system. APSED serves as a road map to guide all countries in the region towards meeing the IHR (2005) core capacity requirements, thus ensuring regional and global health security.
while recognizing variaions in exising capacity levels across countries. It is intended that APSED (2010) will further support progress made towards meeing IHR (2005) obligaions and ensuring collecive regional public health security by miigaing the health, economic and social impact of emerging diseases and public health emergencies in the region.
1.1 Scope
IHR (2005) provides WHO Member States and the WHO Secretariat with a legally binding framework within which they can address issues of preparedness for, recogniion of and response to acute public health risks. Member States are required to develop, strengthen and maintain the core capaciies required under IHR (2005) by June 2012. While emerging diseases including epidemic-prone diseases are an obvious and principal focus, IHR (2005) is also applicable to any acute public health event that may have internaional impact—thus including a broader range of public health threats posed by non-infecious disease events, such as food contaminaion due to chemicals.
The original APSED focused on building capacity for emerging diseases. However, detecion and invesigaion of emerging infecious disease outbreaks has much in common with surveillance and assessment of other acute public health events, as required of countries under IHR (2005). Progress made in the ive APSED focus areas, and the experience gained with pandemic response now provides a good foundaion for countries to expand the scope of APSED aciviies. Moving forward, APSED (2010) coninues to focus on emerging diseases, but it also seeks to build on this common approach and maximize the beneits achieved in the past ive years by widening its scope to include other acute public health threats. Addiionally, the Strategy will idenify new areas of synergy and special situaions to which the Strategy can make important contribuions.
1.2 Intended audiences
APSED (2010) seeks to provide a common framework for countries, WHO and partners to work together to enhance regional defence against public health threats.
seCTIon 1: InTRodUCInG THe sTRaTeGy 1111
1.3 Guiding principles
The following key guiding principles have been considered to shape APSED (2010) and will be used to guide APSED (2010) implementaion.
• The primary focus of the Strategy should be on country aciviies, supported by partnerships at naional, regional and global levels. Country aciviies, such as those related to the naional surveillance systems, should be connected at the regional level.
• The acions taken should include advocacy and aciviies aimed at systemaically strengthening insituional and human capacity in order to ensure sustainability of emerging disease programmes. Plans for capacity- building should be feasible and based on detailed local needs assessments.
• The acions taken through APSED (2010) should build on achievements of the original APSED at country and regional levels and contribute to health systems strengthening.
• The aciviies, policies and pracices implemented through the Strategy should be based on evidence and consider gender, research and ethics aspects wherever possible and feasible, but they should be applied using local knowledge and experise.
• Agencies responsible for the formulaion and implementaion of iniiaives on emerging diseases should seek to idenify synergies and strengthen links with other relevant programmes, such as those concerned with food safety or responsible for humanitarian emergencies.
• Collecive eforts and acions using a common framework are emphasized to achieve the common goal of regional health security.
1.4 Use of the Strategy
It is highly recommended that the Strategy be used in the following ways:
• as a common framework to idenify capacity gaps, agree on priority aciviies, and guide the building and strengthening of naional and local capaciies required for managing emerging diseases and other public health emergencies; • as a mechanism to promote collecive regional health security by establishing
IHR (2005) core capaciies for surveillance, risk assessment and response in all countries and areas of the Asia Paciic region;
• as a common framework to facilitate coordinaion of external support and to maximize mulisectoral collaboraion at naional and regional levels; and • as a strategic document to advocate for and mobilize inancial and technical
1.5 Time frame and targeted outcomes
It is anicipated that the implementaion ime frame for APSED (2010) will be ive years (2011–2015).
When efecively implemented, the Strategy will ensure that countries of the Asia Paciic region have:
• core capaciies to prevent, detect, characterize and respond to emerging disease threats and other acute public health emergencies of naional and internaional concern; and
seCTIon 2: vIsIon, Goal and objeCTIves 13
2.1 Vision
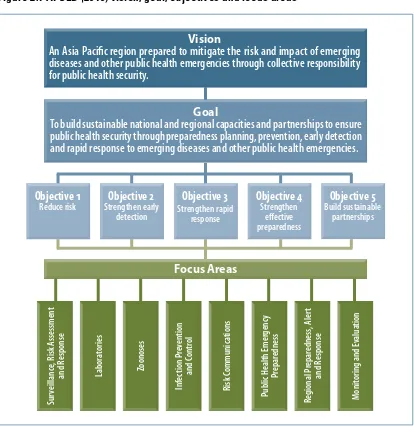
An Asia Paciic region prepared to miigate the risk and impact of emerging diseases and other public health emergencies through collecive responsibility for public health security.
Vision
an asia Paciic region prepared to mitigate the risk and impact of emerging diseases and other public health emergencies through collective responsibility for public health security.
Objective 1 Reduce risk Objective 2 strengthen early detection Objective 3 strengthenrapid response Objective 4 strengthen efective preparedness Objective 5 build sustainable partnerships Goal
To build sustainable national and regional capacities and partnerships to ensure public health security through preparedness planning, prevention, early detection and rapid response to emerging diseases and other public health emergencies.
Focus Areas sur veillanc e, R isk a ssessmen t and Response sur veillanc e, R isk a ssessmen t
and Response labora
tories labora tories ZoonosesZoonoses Inf ec tion P re ven tion and C on tr ol Inf ec tion P re ven tion and C on tr ol Risk C ommunic ations Risk C ommunic ations Public H ealth emer genc y Pr epar edness Public H ealth emer genc y Pr epar edness Regional P repar edness , aler t and Response Regional P repar edness , aler t and Response monit
oring and e
valua
tion
monit
oring and e
valua
tion
Figure 2.1 APSED (2010) vision, goal, objectives and focus areas
2.2 Goal
To build sustainable naional and regional capaciies and partnerships to ensure public health security through preparedness planning, prevenion, early detecion and rapid response to emerging diseases and other public health emergencies.
2.3 Objectives
To achieve the goal, ive interrelated objecives have been ideniied.
• Objecive 1: Reduce the risk of emerging diseases.
• Objecive 2: Strengthen early detecion of outbreaks of emerging diseases and
public health emergencies.
• Objecive 3: Strengthen rapid response to emerging diseases and public health
emergencies.
• Objecive 4: Strengthen efecive preparedness for emerging diseases and
public health emergencies.
• Objecive 5: Build sustainable technical collaboraion and partnership in the
Asia Paciic region.
2.4 Focus areas
To provide a focus for operaional programme work and to achieve the goal and objecives of the Strategy, the following focus areas have been ideniied:
(1) surveillance, risk assessment and response; (2) laboratories;
(3) zoonoses;
(4) infecion prevenion and control; (5) risk communicaions;
(6) public health emergency preparedness;
(7) regional preparedness, alert and response; and (8) monitoring and evaluaion.
seCTIon 3: foCUs aReas and aCTIons 15
This secion describes each focus area, including its key components and proposed strategic acions that should be implemented for systemaic capacity-strengthening.
Table 3.1 APSED (2010) focus areas and key components
Focus area Key components
1. Surveillance, risk assessment and response
Event-based surveillance
Indicator-based surveillance
Risk assessment capacity
Rapid response capacity
Field epidemiology training
2. Laboratories Accurate laboratory diagnosis
Laboratory support for surveillance and response
Coordination and laboratory networking
Biosafety
3. Zoonoses Coordination mechanism for:
{ sharing of surveillance information
{ coordinated response
{ risk reduction { research
4. Infection prevention and control National infection prevention and control (IPC) structure
IPC policy and technical guidelines
Enabling environment (e.g. facilities, equipment and supplies)
Supporting compliance with IPC practices
5. Risk communications Health emergency communications
Operation communications
Behaviour change communications
6. Public health emergency preparedness
Public health emergency planning
National IHR Focal Point functions
Points-of-entry preparedness
Response logistics
Clinical case management
Health care facility preparedness and response
7. Regional preparedness, alert and response
Regional surveillance and risk assessment
Regional information-sharing system
Regional preparedness and response
8. Monitoring and evaluation Country-level monitoring (including workplan and APSED/IHR indicators)
Regional-level monitoring: Technical Advisory Group
Evaluation
3.1 Surveillance, risk assessment and response
Surveillance, risk assessment and outbreak response capacity is a prerequisite for efecive management of emerging disease outbreaks and other acute public health events. Efecive naional surveillance systems generate reliable informaion for imely risk assessment that informs rapid public health acions.
3.1.1 Key components
The key components required for an efecive system of surveillance, risk assessment and response at the naional and local levels are:
• event-based surveillance (EBS); • indicator-based surveillance (IBS); • risk assessment capacity;
• rapid response capacity;
• ield epidemiology training (FET).
EBS is the organized and rapid capture of informaion about events that are a potenial risk to public health. Informaion may be found in internet-accessible informaion sources such as news media sites, disease reporing networks, and other ad hoc reports transmited through formal and informal channels. EBS can provide near real-ime data on potenial and conirmed disease outbreaks and other public health events, including events related to the occurrence of disease in humans, such as clusters of cases of disease and events related to potenial human exposure (e.g. diseases and deaths in animals, contaminated food or water, and environmental hazards, including chemical, radiological and nuclear events).
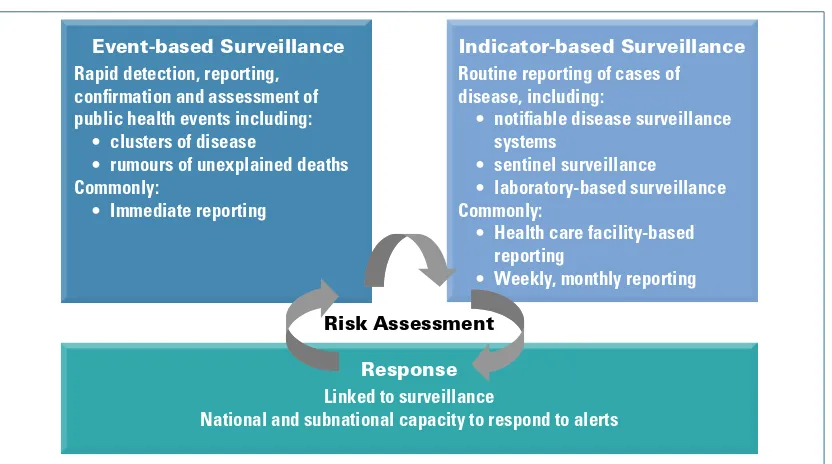
Figure 3.1 Surveillance, risk assessment and response framework
Indicator-based Surveillance
Routine reporting of cases of disease, including:
• notiiable disease surveillance systems
• sentinel surveillance
• laboratory-based surveillance Commonly:
• Health care facility-based reporting
• Weekly, monthly reporting
Indicator-based Surveillance
Routine reporting of cases of disease, including:
• notiiable disease surveillance systems
• sentinel surveillance
• laboratory-based surveillance Commonly:
• Health care facility-based reporting
• Weekly, monthly reporting
Event-based Surveillance
Rapid detection, reporting, conirmation and assessment of public health events including:
• clusters of disease
• rumours of unexplained deaths Commonly:
• Immediate reporting
Event-based Surveillance
Rapid detection, reporting, conirmation and assessment of public health events including:
• clusters of disease
• rumours of unexplained deaths Commonly:
• Immediate reporting
Response
Linked to surveillance
National and subnational capacity to respond to alerts
Response
Linked to surveillance
seCTIon 3: foCUs aReas and aCTIons 17
IBS is the systemaic collecion and analysis of imely, reliable and appropriate data on priority diseases, syndromes and condiions. Data collecion follows a predeined format and includes speciic case or syndrome deiniions. Data reporing and analysis occur regularly, typically once a week, and alert or epidemic thresholds are oten used to idenify outbreaks. IBS aims at outbreak detecion, monitoring of disease trends and disease control programmes and programme planning. Use of appropriate informaion and communicaion technology (ICT) tools may aid in improving the quality of collecion and collaion of surveillance data at the naional and local levels.
Risk assessment is a systemaic process for gathering, assessing and documening informaion to assign a level of risk for a potenial public health event. This enables objecive evidence-based decisions while giving consideraion to the uncertainies and limitaions of the informaion available at a paricular point in ime. It involves understanding the idenity and character of a hazard and evaluaing the risk of an adverse outcome in a populaion following exposure to that hazard. The process can also assess the risk associated with potenial intervenion measures. During an event, risk assessment is an ongoing process, not a one-ime acivity.
Rapid response capacity in this context refers to the ability to mobilize a rouine and rapid invesigaion of and response to public health events at naional and local levels. This includes development and deployment of rapid response teams (RRTs) to any level in the public health sector.
IBS and EBS are complementary and both are essenial components of naional surveillance systems. Surveillance informaion is used to help risk assessment, which in turn informs public health acions. Surveillance, risk assessment and response oten require efecive mulilevel, mulidisciplinary and mulisectoral coordinaion. APSED (2010) provides a framework for Member States to create a robust system of surveillance, risk assessment and response that includes the above interlinked components, as described in Figure 3.1.
The surveillance and response system should be sensiive and broad enough to allow detecion of other public health events, including non-infecious disease events (e.g. chemical and food safety-related events) and lexible enough to be adapted to special situaions (e.g. mass gatherings, natural disasters). The surveillance and response prioriies of each country should be informed through risk mapping so that any ideniied needs can be met.
FET has proved invaluable in establishing naional capaciies for early detecion, prompt invesigaion and efecive response to public health events. FET focuses on learning by doing in a work seing and building competencies applicable to emerging disease outbreaks and other public health events.
3.1.2 Strategic actions
• Expand the scope of training of RRTs to support an all-hazards approach, with a speciic focus on the iniial assessment of events.
• Strengthen risk assessment capacity at all levels.
• Conduct naional risk and vulnerability mapping to idenify threats to public health, exposure factors, and the risk and protecive factors that increase or decrease the adverse impact of an outbreak or other acute public health event on the populaion at risk.
• Build on exising mechanisms to promote and strengthen mulidisciplinary and interagency coordinaion for surveillance, risk assessment and response. • Consider the use of appropriate informaion and communicaion technology
tools to support surveillance, risk assessment, and response aciviies. • Strengthen ield epidemiology training.
3.2 Laboratory
Eicient and reliable public health laboratory services are an essenial component of any public health system that aims to efecively respond to emerging diseases.
Timely, accurate laboratory diagnosis in a safe environment is a cornerstone of any surveillance and response system for emerging diseases and other public health events. Strengthening naional and regional capacity for accurate laboratory diagnosis, laboratory-based surveillance and networking, and biosafety is therefore an essenial component of eforts to ensure regional health security. Public health laboratory capacity-building will coninue to focus on emerging diseases under APSED (2010), and these aciviies need to be coordinated with the WHO Asia Paciic Strategy for Strengthening Health Laboratory Services (2010–2015) and disinct regional strategies on the prevenion and containment of animicrobial resistance.
3.2.1 Key components
The key components of laboratory capacity-building to support emerging disease management are:
• accurate laboratory diagnosis;
• laboratory support for surveillance and response; • coordinaion and laboratory networking;
• biosafety.
seCTIon 3: foCUs aReas and aCTIons 19
reduce risk and miigate the impact of disease outbreaks. Laboratory capacity needs to be established in all countries for the diagnosis of potenial emerging diseases. This involves ensuring that internal quality control (IQC) and external quality assurance (EQA) are in place. In addiion, links with reference laboratories will further enhance the capacity of public health laboratories and help with ideniicaion of unusual or new pathogens.
Support should be given to strengthen or establish links between public health laboratories and other laboratories that may need to be involved in surveillance, risk assessment and response aciviies, including clinical, veterinary and research laboratories. It is also important to strengthen laboratory capaciies at the local level to support early detecion of disease events and more rouine surveillance aciviies. There is a need to provide incenives to recruit and retain skilled laboratory staf at the local level (e.g. provincial and district levels).
Because laboratory capacity varies within and between countries—and experience in dealing with diferent infecious agents is similarly uneven—naional, regional and global laboratory networks are vital to support public health surveillance and responses. Laboratory networking between local and naional reference laboratories needs to be strengthened and coordinaion among public health, clinical, food, veterinary and other laboratories ensured. Links should also be established with regional and global reference laboratories that provide highly specialized services. For example, chemical analysis and toxicology are unavailable or unobtainable in many countries. There is also a need to advocate for the formulaion of policies and agreed procedures to facilitate seamless sharing of samples, reagents, training materials, guidelines and the experiences of laboratory management between naional and regional reference laboratories.
Safe laboratory environments and safe pracices are required to avoid staf members and other people from becoming infected by the hazardous agents they are handling or if there is an accidental release of the agent. Laboratory biosafety is best addressed by strengthening programmes through policy development, promoion of best pracices through training and quality improvement aciviies, and ensuring that levels of biosecurity applied to every laboratory are matched to levels of assessed risk (i.e. according to the agent handled).
3.2.2 Strategic actions
• Strengthen accurate laboratory diagnosic capacity for priority emerging diseases through naional IQC and EQA.
• Ensure efecive laboratory referral systems through strengthening naional, regional and internaional laboratory networking and coordinaion with other laboratory services (such as animal and food laboratories) and highly specialized laboratory services.
• Strengthen laboratory biosafety aciviies to ensure diagnoses of emerging diseases are conducted in safe environments.
3.3 Zoonoses
Zoonoic diseases (i.e. zoonoses) are described as diseases or infecions that are naturally transmissible from vertebrate animals to humans and vice versa. Recent evidence has shown that approximately 60% of all human diseases currently recognized and about 75% of emerging diseases that have afected humans over the last three decades have originated from animals. Prevenion, detecion and control of zoonoic diseases are therefore essenial components of any naional emerging diseases programme. Regionally and globally, the importance of zoonoic diseases has been recognized with the Food and Agriculture Organizaion of the United Naions (FAO), the World Organisaion for Animal Health (OIE), and WHO working in collaboraion with each other and with other partners to contribute to the concept of “One Health”.
Strengthening generic capacity in naional surveillance, risk assessment and response systems, as well as other APSED focus areas such as risk communicaions and laboratory services, will help to ensure early recogniion of, rapid response to, and prevenion and control of zoonoic diseases.
Given the unique nature of zoonoic diseases, ensuring sustainable and efecive coordinaion and collaboraion mechanisms between the human and animal health sectors is vitally important and needs to be further strengthened. In addiion, reducing the risk of transmission of zoonoic diseases from animals to humans oten requires close collaboraion and links with the food safety, environment and wildlife sectors. Experiences and lessons learned from avian inluenza A (H5N1) in the region over the past few years provide a good foundaion to consolidate and strengthen naional and regional coordinaion mechanisms for surveillance informaion-sharing and coordinated responses by human and animal heath sectors.
3.3.1 Key components
The key components of zoonoses coordinaion and collaboraion are: • sharing of surveillance informaion;
seCTIon 3: foCUs aReas and aCTIons 21
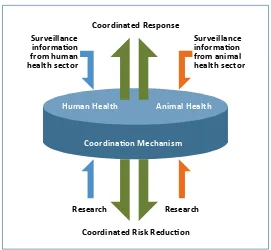
Timely sharing of data collected through human health, animal health and food safety surveillance networks is criical to facilitate early reporing of zoonoses of public health importance. Coordinaion between human health, animal health, wildlife and other sectors will facilitate rapid epidemiological invesigaion and risk assessment of events and implementaion of any required control measures. Advocacy is required to explore ways to consolidate, improve and sustain such coordinaion and collaboraion mechanisms.
Reducing the risk of disease transmission at the human–animal interface is key to zoonoses prevenion. In the past, it has occasionally been necessary to apply urgent intervenions in a somewhat ad hoc manner because good evidence on risk-reducion measures was unavailable. A greater efort is therefore required to further idenify and implement evidence-based measures to reduce the risk of animal-to-human transmission in a more sustainable way.
This will require collaboraive research on zoonoic diseases in order to provide evidence for intervenion and policy formulaion. Strengthening operaional research aciviies will require investment by both the animal and human health sectors.
Figure 3.2 Zoonoses coordination mechanism
Coordinated Response
Coordinated Risk Reducion
Surveillance informaion from animal health sector
Human Health Animal Health
Coordinaion Mechanism
Surveillance informaion from human health sector
Research Research
3.3.2 Strategic actions
• Determine long-term risk-reducion measures for priority zoonoses and implement sustainable risk-reducion aciviies through promoing best pracices at the human–animal interface, collaboraing with food safety programmes and implemening appropriate risk communicaions aciviies.
• Idenify and strengthen collaboraive operaional research on zoonoses and share research indings and lessons learnt in a imely manner to inform public health acion, whenever appropriate.
3.4 Infection prevention and control
Establishing efecive infecion prevenion and control (IPC) pracices in health care seings is essenial to reduce the risk of transmission of emerging diseases to health care workers, paients, their families and the community. Systemaic establishment of good IPC pracices is a challenge, and there is room for signiicant improvement in many hospitals and other health care faciliies in the region. IPC is not always considered a priority in many countries when compared with other aciviies required for responding to an outbreak.
Good IPC pracices are especially important in health care faciliies when outbreaks occur because of the risk that faciliies will become epicentres for the spread of infecion. In addiion, infecions in staf can criically afect delivery of health care services and provision of surge capacity when it is most needed.
It is important to acknowledge that IPC measures applied during an outbreak should be built on a solid foundaion of good daily pracice, i.e. that high-quality IPC pracice in hospitals and other health care faciliies are a prerequisite for efecive outbreak response. There is now widespread consensus on the infrastructure and policies that should be established to underpin good IPC pracice. Much remains to be done, including advocacy for implementaion. Local IPC experts should be supported to be efecive praciioners, trainers and advocates. Similarly, naional centres of excellence should be ideniied, acknowledged and supported to eventually become IPC resources for countries and the region.
3.4.1 Key components
The following components have been ideniied as prioriies under the Strategy: • naional IPC structure;
• IPC policy and technical guidelines;
seCTIon 3: foCUs aReas and aCTIons 23
The establishment of efecive IPC pracice is best achieved by establishing strong IPC programmes, staring with health care faciliies at the naional level. These programmes should be led by mulidisciplinary IPC commitees and underpinned by dedicated staf, appropriate surveillance systems and mechanisms for quality improvement.
IPC policies and technical guidelines should be determined at the naional level and adapted for local implementaion.
Efecive IPC pracice also require establishment of safe working environments, including the physical infrastructure of hospitals and other health care faciliies, regular supply of commodiies and good administraive controls (e.g. arrangements for safe and appropriate management of health care waste).
Implementaion of appropriate IPC pracice can be monitored in a number of ways, including surveillance for hospital-acquired infecions and animicrobial resistance. However, standards of pracice are probably ensured most efecively by establishment of programmes for coninuous quality improvement (e.g. audit followed by feedback and support to address any issues ideniied).
3.4.2 Strategic actions
• Conduct IPC needs assessments that are helpful for advocacy, policy development, and monitoring and evaluaion.
• Establish and strengthen organizaional structure of naional IPC programmes, including strengthening naional and local mulidisciplinary IPC commitees, designaing an IPC focal point within the Ministry of Health, and establishing a naional IPC resource centre.
• Develop and implement evidence-based IPC policies and technical guidelines. • Enable a supporive environment for IPC pracice, including faciliies, equipment
and supplies.
• Establish mechanisms to support compliance with IPC pracice.
• Idenify and support naional and regional IPC experts and centres of excellence to become agents of change.
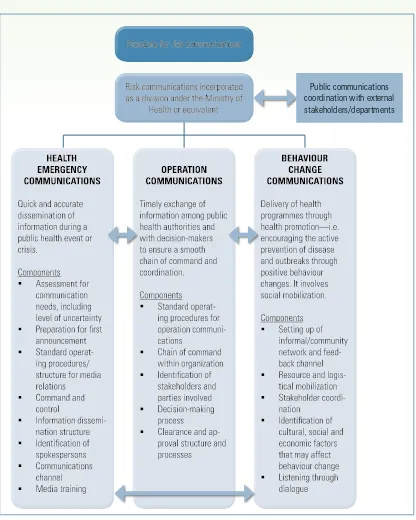
3.5 Risk communications
diseases and other public health threats by informing decision-making, encouraging posiive behaviour change and maintaining public trust.
3.5.1 Key components
The key components of risk communicaions are three interlinked funcional areas that were ideniied during past outbreak responses, namely:
• health emergency communicaions • operaion communicaions
• behaviour change communicaions.
Health emergency communicaions refer to the rapid disseminaion of informaion and health messages to target audiences during a health emergency. The objecives of health emergency communicaions are to build public trust, enable and empower populaions to adopt protecive measures, reduce confusion, and facilitate enhanced disease surveillance. This component includes the iniial announcement and informaion disseminaion through mass media.
Operaion communicaions are the imely exchange of informaion among internal stakeholders including health authoriies, clinicians, laboratories, decision-makers and other disciplines and sectors. Efecive operaion communicaions ensure coordinated response and keep decision-makers informed of the situaion, enabling them to make informed choices on possible next steps and policy changes. In addiion, operaion communicaions should also take into consideraion inter-country communicaions, especially when disease outbreaks or other public health emergencies afect cross-border areas.
Behaviour change communicaions refer to the establishment and implementaion of health promoion programmes for prevenion and control of emerging diseases and other threats to public health, including the promoion of protecive behaviours and social mobilizaion during public health emergencies. Behaviour change communicaions adopt a long-term approach and work closely with communiies.
seCTIon 3: foCUs aReas and aCTIons 25
Public communications coordination with external stakeholders/departments Figure 3.3 Structure of risk communications and corresponding needs
3.5.2 Strategic actions
• Establish and promote risk communicaions concepts and a framework to ensure common understanding, interpretaion and best pracices of risk communicaions.
capacity. Consideraion should also be given to development of ICT infrastructure to improve the speed of communicaions and to keep up to date with developments in social and online networking, which are increasingly becoming popular sources of news.
• Share risk communications best practices by building on real-world experiences, gained through responding to public health emergencies.
3.6 Public health emergency preparedness
Public health emergencies, paricularly those events caused by outbreaks of emerging diseases, pose a serious threat to naional and regional health security. Recent experience has demonstrated that efecive preparedness can ensure a rapid public health emergency response and minimize negaive health, economic and social impacts.
Building on lessons learnt from the pandemic preparedness and response planning under APSED over the past five years and experience gained through responding to pandemic influenza (H1N1) 2009, this focus area addresses the need for preparedness planning for public health emergencies caused by emerging diseases and other acute public health events. Since there are significant commonalities between pandemic preparedness and emergency planning for other acute public health events, APSED (2010) promotes a generic approach to public health emergency preparedness and response planning and threat-specific plans.
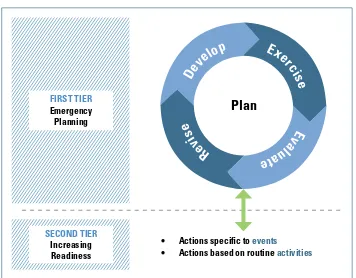
Figure 3.4 Two-tiered approach for public health emergency preparedness
FIRST TIER Emergency Planning SECOND TIER Increasing Readiness
Plan
• Actions speciic to events
• Actions based on routine activities
D
e
v
seCTIon 3: foCUs aReas and aCTIons 27
Through experience and lessons learnt from pandemic preparedness, public health emergency preparedness should involve a two-iered approach, as described below.
• Emergency planning: The first tier is to formulate, exercise, evaluate and
revise a public health emergency response plan. Experience with exercising and revising these plans explicitly highlights the need to ensure a continuous cycle of developing and maintaining up-to-date emergency response plans.
• Increasing readiness: The second tier is to increase readiness and capacity to
activate the plan. This effort can involve strengthening event-specific activities (such as stockpiling essential medicines for treatment and personal protective equipment), and actions related to routine generic capacity-building.
Many rouine aciviies intended to improve readiness (such as strengthening surveillance, risk assessment and response systems, and risk communicaions) have already been described in the document. This focus area describes public health emergency planning with an emphasis on the coninuous planning cycle and some speciic preparedness aciviies that are criical but not yet addressed as separate focus areas under this Strategy, such as the Naional IHR Focal Point funcions, clinical case management and response logisics.
The key components (preparedness aciviies) requiring speciic atenion to ensure efecive public health emergency preparedness and response under this focus area are:
• public health emergency planning; • Naional IHR Focal Point funcions; • points-of-entry preparedness; • response logisics;
• clinical case management; and
• health care facility preparedness and response.
3.6.1 Public health emergency planning
Public health emergency planning involves the formulaion, validaion, evaluaion and revision of public health emergency response plans. This implies that plans should be updated regularly and be lexible enough to adapt to changing needs during a public health emergency response.
Two opions can be considered when formulaing and maintaining such public health emergency response plans within the health sector.
• A step-by-step approach to formulate an overarching generic public health emergency preparedness and response plan. Building on the experience of developing a naional pandemic preparedness and response plan, a generic preparedness and response plan for all emerging diseases can be developed. Such a plan can then link to or expand to cover other public health events, such as food safety events. Links may also be established with emergency response plans for other events, including natural disasters and humanitarian emergencies.
• Speciic plans can be formulated for a disease or event (e.g. an inluenza pandemic response plan, a food safety emergency response plan).
APSED recommends that its focus areas are addressed and that streamlined coordinaion mechanisms be fully used to idenify synergies while maximizing use of limited resources and infrastructure.
The key acions are:
• integrate the naional pandemic preparedness and response plan into a public health emergency plan for all emerging diseases;
• formulate a generic public health emergency preparedness and response plan to address emerging diseases and other acute public health events (e.g. food safety events) for which the health sector is primarily responsible, and where appropriate, link with other emergency response plans;
• test and update the plan through regular exercises (e.g. table-top and ield simulaions); and
• establish tools, mechanisms and processes for mulidisciplinary risk assessment and decision-making for signiicant public health emergencies.
3.6.2 National IHR Focal Point functions
seCTIon 3: foCUs aReas and aCTIons 29
role performed by the NFP is and that the NFP should be part of naional structures for public health emergency preparedness and response. Mandatory funcions of the NFP under IHR (2005) include:
• sending urgent communicaions concerning IHR (2005) implementaion to the WHO IHR Contact Point, in paricular those communicaions related to event noiicaion, reporing, consultaion, veriicaion, providing informaion, and determining whether an event is a public health emergency of internaional concern (PHEIC); and
• disseminaing to and consolidaing informaion from relevant government departments and other sectors within the country, including those eniies responsible for surveillance and response, points of entry (POE), public health services and hospitals.
Although the funcions of the NFP are well deined, the departments or units designated by countries to undertake these funcions vary considerable in terms of their locaion, roles and capaciies. While the NFP role in many countries is based in a communicable disease unit or in an emergency response unit, the NFP task is also carried out by diferent oices in other countries. In terms of funcion, while some NFPs carry out both communicaion and coordinaion, others focus primarily on IHR event communicaions.
Three opions are available regarding the roles and responsibiliies of NFPs.
• Primarily serve to facilitate IHR event communicaions for all public health events.
• Facilitate IHR communicaions for all public health events and coordinate IHR-related aciviies only for infecious disease events.
• Facilitate both IHR communicaions and coordinaion for all public health events.
The key acions are:
• establish, update, test and implement standard operaing procedures that address terms of reference, roles and responsibiliies of the NFP, as well as implemening structures, communicaion and/or coordinaion links with naional stakeholders and WHO; and
• strengthen the NFP role in informaion-sharing through the use of the secure IHR Event Informaion Site (EIS) and facilitaing intercountry communicaions, when appropriate.
3.6.3 Points-of-entry preparedness
• from a ixed list of diseases to all public health events and emergencies; • from control of borders to also containment at source; and
• from preset measures to adapted responses.
With this paradigm shit, and as part of the naional and internaional collecive defence system for health security, POE now have a diferent role to play in detecing and responding to acute public health events and emergencies of naional, regional and internaional concern.
The POE role can beter be appreciated if it is placed in the context of the overall naional and internaional systems for managing emerging diseases and public health emergencies. Collecive eforts in managing public health risks and events at POE, efecive POE public health emergency planning, sharing informaion, coordinaion and establishment of consistent border health measures can all contribute to naional and internaional health security.
Strategic approaches to strengthening the POE public health funcion include use of exising tools, guidelines, faciliies and services to strengthen rouine public health funcions at POE; encouraging POE paricipaion in naional and local systems for surveillance and response; emphasis on the importance of pre-arrangements with relevant agencies and service providers to ensure efecive emergency preparedness and response; and encouraging regional collaboraion and networking of POE public health authoriies to ensure coordinated and consistent public health measures at internaional borders, when appropriate.
The key acions are:
• facilitate high-level advocacy and sensiizaion regarding the role of POE under IHR (2005) for both rouine measures and emergency response;
• prioriize POE designaion and build IHR core capacity at designated POE, especially through POE public health emergency planning in the context of the overall naional public health emergency response structure; and
• promote regional and internaional partnership and collaboraion on managing public health events and emergencies at POE.
3.6.4 Response logistics
seCTIon 3: foCUs aReas and aCTIons 31
Response logisics goes beyond rouine supply-procurement processes and applies to situaions in which there is an urgent need to provide rapid logisics support, including deploying human resources, seing up communicaions, ensuring security, and arranging for the collecion and shipment of clinical specimens in a compressed ime frame. Coordinaion is essenial to ensure imely and efecive response logisics support when undertaking these aciviies during a disease outbreak or public health emergency.
The key acions are:
• advocate and promote the importance of response logisics within the heath sector among naional policy-makers, health oicials and others;
• formulate a clear model for response logisics, including coordinaion mechanisms to be used during a public health emergency situaion;
• ensure human resource development (e.g. trained outbreak response logisicians); and
• establish a more comprehensive response logisics system within exising health structures to support outbreak and public health emergency response.
3.6.5 Clinical case management
Delivery of high-quality clinical care is criical to minimize morbidity and mortality during any outbreak of an emerging disease. Although raising overall standards of clinical pracice is beyond the scope of APSED, delivery of high-quality clinical case management for emerging diseases can be strengthened in some key areas.
The diversity of the Asia Paciic region results in signiicant variaions in paterns of infecious diseases. Experience has also shown that these paterns change over ime and that novel diseases emerge and spread, driven by factors including urbanizaion, climate change and internaional travel. It is criical that clinicians in all countries, including criical care specialists, are supported to rapidly idenify and treat infecious disease cases in order to apply appropriate therapeuic and IPC measures. In addiion, a vital need exists to ensure regional mechanisms are in place to facilitate sharing of informaion between clinicians on the features of emerging diseases, as well as diagnosic techniques and modaliies of treatment.
The key acions are:
• establish arrangements to allow mobilizaion of experts in clinical management to provide on-the-ground support if needed through the Global Outbreak Alert and Response Network (GOARN) or local networks;
• facilitate informaion exchanges on clinical management issues by connecing clinicians who have informaion needs to others with disease-speciic experise and specialist knowledge on clinical case management; and
• formulate relevant guidelines and training materials and distribute them in a imely manner during an outbreak.
3.6.6 Health care facility preparedness and response
During an outbreak of an emerging disease, most severely ill paients will be diagnosed and treated in a health care facility. However, during large outbreaks, demand for care can exceed normal delivery capacity, so plans need to be established to deal with this situaion.
Health care facility preparedness and response plans should provide a comprehensive framework for responding to any emerging disease outbreak. They normally will include planning for providing surge capacity (for screening and triage, beds, staf, laboratory tesing and communicaions), prioriizaion of treatment, supplies of consumables, and plans to strengthen clinical management and IPC. Individual facility plans should also be coordinated with the preparedness and response plans of other health care faciliies in the same area in order to use resources in the most eicient way during a large-scale public health event.
Planning for delivery of health care during a large outbreak also needs to be coordinated at local and naional levels. At the local level, plans for individual health care faciliies should take into account exising “civil society” structures (e.g. health care volunteer organizaions) and there must be coordinaion between health care faciliies (e.g. a common understanding of protocols for transfer of paients). At the naional level, informaion on hospital admissions, use of emergency services and use of consumables should be collected on a daily basis and analysed to ensure the most eicient and equitable delivery and coordinaion of health services.
The key acions are:
• formulate naional guidance and training materials on health care facility preparedness and response planning and support planning process;
seCTIon 3: foCUs aReas and aCTIons 33
• strengthen naional coordinaion and oversight of health care delivery during a large outbreak to address surge capacity and ensure eicient and equitable delivery of health services.
3.7 Regional preparedness, alert and response
Threats to public health, such as emerging diseases, go beyond national borders. IHR (2005) places a requirement on WHO to strengthen regional and global systems and capacity for surveillance, risk assessment and response in order to support countries by ensuring that rapid and appropriate support can be provided for these activities in response to acute public health events.
3.7.1 Key components
The key components of regional preparedness, alert and response are: • regional surveillance and risk assessment;
• regional informaion-sharing system; and • regional preparedness and response
Efecive surveillance and risk assessment at the regional level relies upon having established event-based and indicator-based surveillance systems, as it does at the country level. Regional event-based surveillance involves collecing and analysing informaion about events that may be a potenial risk to regional public health. These data are collected by using informal and formal informaion sources, such as media reports and government statements and oicial IHR communicaions. Regional indicator-based surveillance involves the collaion of rouinely reported naional disease data at the regional level, accompanied by imely analysis and joint risk assessment. Surveillance has the potenial to provide an addiional early warning system for all countries, paricularly for diseases such as dengue that can spread rapidly across the region. Regional risk assessment is conducted to idenify and characterize public health threats and to evaluate any associated risks. Risk assessments are conducted daily by WHO on event-based data and reports on priority diseases in order to ensure that WHO is operaionally ready to support countries at any ime, as required under IHR (2005).
Regional informaion-sharing is an essenial part of an efecive preparedness, alert and response system. Timely and accurate sharing of informaion at the regional level helps inform evidence-based public health acions. Informaion that may be useful in informing opimal public health acion can include immediate informaion on acute public health events, real-ime informaion on evolving public health events, surveillance data, guidelines, reports, examples of best pracices in the control of emerging diseases, and publicaions on regionally relevant epidemiological and other indings.
event, or a release of toxic agents. Ensuring this response capacity, which may include accessing exising networks and regional stockpiles, is an essenial component of regional preparedness.
3.7.2 Strategic actions
• Strengthen regional surveillance and risk assessments by establishing a regional indicator-based surveillance system for priority diseases and rapid feedback mechanisms for surveillance informaion.
• Strengthen the regional surveillance system for public health emergencies. • Strengthen the regional informaion-sharing system to help provide more
relevant and reliable data to inform evidence-based public health acion. • Strengthen comparability of naional data at the regional level through a number
of iniiaives, including drawing up a minimum data set for rapid assessment of novel (previously unknown) diseases.
• Strengthen technical response networks through expanding and using GOARN partners and other experts in the ideniicaion, preparaion and response to acute public health events.
• Build networks of relevant experts and strengthen links between naional and reference laboratories to enable access to specialized laboratory services for emerging diseases and other public health threats.
3.8 Monitoring and evaluation
Monitoring and evaluaion (M&E) are integral components of APSED (2010) and its implementaion. Robust M&E is fundamental to meet two criical management needs: accountability and learning. In the context of this Strategy, accountability can be deined as the ability to demonstrate that the Strategy is efecive in achieving its objecives, that its prioriies are appropriate, and that resources have been used opimally. Similarly, learning (within the context of M&E) can be deined as understanding what is working and what can be done beter, which in turn helps to ensure that decisions are based on evidence, facilitaing coninuing improvement.
3.8.1 Key components
A combinaion of country- and regional-level components is proposed to strengthen the M&E system under the Strategy:
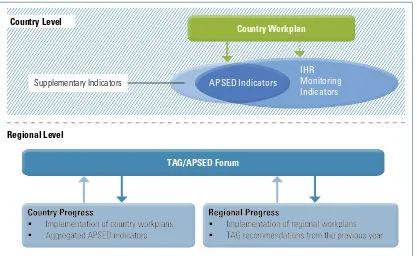
3.8.1.1 Country level
seCTIon 3: foCUs aReas and aCTIons 35
Establishment of naional workplans to achieve APSED (2010) objecives will support a structured approach to capacity-building. Clear imelines and progress indicators to monitor workplan implementaion can then be used to monitor implementaion of APSED, as well as the progress of naional capacity-building towards IHR (2005) compliance, when appropriate. Country workplans enable countries to assess their own progress and idenify needs and opportuniies. This approach may be paricularly useful to facilitate donor coordinaion for resource-limited countries.
A number of APSED indicators will be ideniied and monitored at the regional level. These indicators will be selected from the IHR Monitoring Framework for monitoring progress in the implementaion of IHR core capaciies in State Paries and supplemented, where necessary, by indicators set up for areas requiring speciic consideraion under APSED (2010). Countries also may wish to consider referring to these APSED indicators as the basis for a naional tool to monitor capacity-building. Whenever possible, M&E indicators from relevant exising programmes can be uilized to reduce the burden of data collecion.
3.8.1.2 Regional level
• TAG mechanism (or equivalent)
The annual Technical Advisory Group (TAG) meeing, or its equivalent, also performs a monitoring role by reviewing progress made in the past year and making recommendaions to provide a focus for implementaion in the forthcoming year. It is a unique forum for countries, technical experts and partners to meet and discuss APSED issues and share experiences with counterparts in the Asia Paciic region.
Country Level
Supplementary Indicators
Regional Level
Country Workplan Country Workplan
Figure 3.5 APSED (2010) monitoring and evaluation structure
TAG/APSED Forum TAG/APSED Forum
[image:37.595.92.509.520.776.2]Strengthening M&E aciviies at this level will help idenify naional gaps in M&E and improve each country’s capacity.
External evaluaion will be conducted at the conclusion of the Strategy implementaion period, when appropriate and agreed upon by concerned countries. However, a balance is needed to ensure that M&E helps build country capacity and improve country ownership.
3.8.2 Strategic actions
• Strengthen the capacity of countries to implement M&E tools and systems, including use of the IHR Monitoring Framework.
seCTIon 4: sPeCIal sITUaTIons and aPPRoaCHes 37
There are a number of special situations that may require consideration and modified approaches when implementing APSED (2010).
Several countries and areas, such as the Paciic island countries and areas, Bhutan, Maldives and Timor-Leste, face unique naional and local capacity-development challenges due to a combinaion of factors, such as the small size of populaion, geographical isolaion, limited infrastructure and resources, and low baseline APSED capacity. Considering this special situaion, tailored approaches may be applied by these countries and areas when implemening APSED (2010) to meet the IHR (2005) requirements. Suggested approaches include:
• addressing challenges faced by areas of special public health needs, while implemening capacity-building aciviies in all of the APSED focus areas; • allowing flexibility to adapt the regional Strategy to meet the special
situations present in areas of public health needs, including approaches to resource-sharing and the implementation of standardized syndromic surveillance systems;
• addressing human resource development as a high priority through distance learning, in-country training and formal educaion focused on public health, when appropriate; and
• strengthening Paciic regional coordinaion mechanisms, internaional laboratory networks and improving interagency technical support.
Speciic event situaions, such as mass gatherings or the deliberate release of chemical, biological, radiological or nuclear (CBRN) agents should also be considered where relevant. Suggested approaches include:
• using or adapting existing public health preparedness, surveillance and response systems and networks to address specific event situations where required;
• utilizing specific event situations, such as mass gatherings, as an opportunity to obtain government and external support to strengthen long-term improvement of existing public health systems and capacities (i.e. establishing a health legacy); and
• strengthening regional preparedness to support public health responses for identified specific event situations and strengthening regional networks to facilitate sharing of experience and lessons learnt.
Social and environmental factors such as gender, inequality of services, migraion and climate change may also impact emerging disease programmes. These contextual factors may be taken into consideraion where relevant and feasible, when implemening APSED (2010). Possible approaches include:
• supporing and paricipaing in relevant advocacy and awareness aciviies; • paricipaing in iniiaives related to social and environment factors that have
clear implicaions for addressing emerging diseases; and
seCTIon 5: ImPlemenTInG THe sTRaTeGy 39
Emerging diseases and public health emergencies have substanial negaive economic impact on travel, tourism and trade, and may cause signiicant social disrupion and security concerns. Collecive acions of countries, technical experts, WHO and partners to implement the Strategy in a coordinated fashion are essenial to achieve the goal and objecives of APSED (2010)—ensuring regional public health security.
A mulisectoral approach, which enhances naional and regional coordinaion, collaboraion and harmonizaion among diferent stakeholders and is supported by adequate human resources and sustainable inancing mechanisms, is required to implement the Strategy efecively.
M&E is a criical component of Strategy implementaion and has been included as one focus area under Secion 3.
5.1 Regional coordination and management model
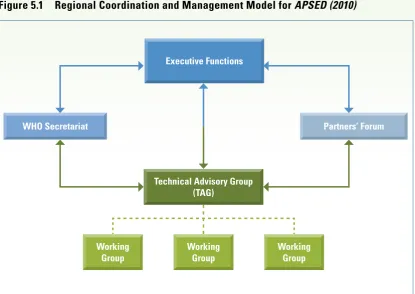
The following mechanisms are recommended to facilitate regional-level communicaion, coordinaion, management and monitoring of the Strategy (Figure 5.1).
5.1.1 Executive functions
Regional Commitees, WHO’s governing bodies in the South-East Asia and Western Paciic Regions, or other high-level forums of senior decision-makers from each naional health authority, such as the meeing of health ministers, will be used, when appropriate, to ensure poliical commitment, to engage in policy decisions (e.g. through adopion of resoluions), and to support acivity implementaion (e.g. through progress reporing).
5.1.2 Technical Advisory Group
The Asia Paciic Technical Advisory Group on Emerging Diseases will coninue to funcion as the key mech