Page 1 of 2 https://www.njppp.com/?sec=eboard
Online First Current Issue Archive Most Downloaded Most Accessed
Service by
Home Journal Issues Guide for Authors Editorial Board About Aims & Scope Editorial Contact
Chief Editor Dr. Jaykaran Charan
Emeritus Editor Dr. Bharat Gajjar
Executive Editors Dr. Rajiv Mahajan Dr. Dharitri Parmar Dr. Summaiya Mulla Dr. Jagdish Goyal
Assistant Editors Dr. Amit Shah Dr. Jatin Dhanani Dr. Rakesh Ranjan Pathak Dr. Anuradha Joshi
Technical Editors (Language and Reference) Amit Upadhyah, Bhuj (India)
Ashutosh Jaiswal, Allahbad (India) Ebadullah Raidullah Shafi, Sharjah (UAE) Manish kumar khazane, Hyderabad (India)
Sarat chandra viswanadh Tata, Visakhapatnam (India)
Statistical Consultant Dr. Deepak Saxena Dr. Pankaj Bhardwaj
International Editorial Board Vipra Kundoor, USA Dr Ambrose Furey, Ireland Dr. Himanshu Gupta, USA Dr. Omar AlHussaini , Oman Professor Bhushan Patwardhan, India Dr. Ugur Cakilcioglu, Turkey Dr. Upendra Nagaich, India
AUTHOR LOGIN REVIEWER LOGIN
Indexed In
National Journal of Physiology,
Pharmacy and Pharmacology is Indexed in
-EMBASE
Index Copernicus (ICV 2016: 109)
Index Medicus for SEAR CAB abstract/Global Health CINAHL
Hinari
Google Scholar
ScopeMed
Ulrich’s International Periodical Directory
Indian Science Abstracts Open J- Gate
Geneva Foundation for Medical Education and Research
NewJour PSOAR InformIndia
EBSCO Publishing Electronic Database
Genamics JournalSeek ProQuest
Index Scholar SafetyLit
Chemical Abstracts Service (CAS)
Gale's Health Reference Center
16/02/18 17.13 National Journal of Physiology, Pharmacy and Pharmacology
Page 2 of 2 https://www.njppp.com/?sec=eboard
Dr. Achuta Kumar Guddati, USA Dr. M. Mohamed Essa, Oman Dr. A. B. Pant, India
Dr. Haleagrahara S. Nagaraja, Australia Dr. G. K. Pal, India
Dr. Ken Master, Oman Dr. Mu Xiaomei, China Dr. Amar Jesani, India Dr. Nashwa elgendy, USA
Mrs. Indah Binti Mohd Amin, Malaysia Dr. Bontha V. Babu, India
Dr. Lamiaa ahmed, Egypt Mr.sci dr Sladjana, Serbia Dr. B.Unnikrishnan, India Prof. Jacob A Kolawole, Nigeria Dr. Jianxia Guo, USA Mr.sci dr Branko, Serbia Dr. Ramin Ataee, Iran
Dr. Sharmishtha Ghosh, Malaysia Dr. Shehta Said, Egypt
Prof. Sheikh Riazuddin, Pakistan Dr. Sultan Suleman, Ethiopia Dr. Kamalakkannan Srinivasan, USA
Dr. Sameer Dhingra, Trinidad and Tobago, Latin America Dr. Spandan Shah, Post doctoral fellow, Columbia University, USA
National Editorial Board Dr. N. D. Kantharia, Surat Dr. Preeti Kapadia, Surat Dr. Barna Ganguly, Karamsad Dr. Swapnil Agarwal, Karamsad Dr. Chinmay Shah, Bhavnagar Dr. Prashant Nag, New Delhi Dr. Aswini Datt. R, Mangalore
Ind Medica Scirus
Scientific Publication Index Scientific Resources Database
Recent Science Index Scholarly Journals Index Directory of Academic Resources
Elite Scientific Journals Archives
Current Index to Scholarly Journals
Digital Journals Database Academic Papers Database Contemporary Research Index
Ayush Web Portal CiteFactor
Journal Membership World Association of Medical Editors (WAME), Dallas, Texas,
USA
Journal Listed in ICMJE- International Committee
of Medical Journal Editors HIFA 2015 – Healthcare Information for All by 2015, Charlbury, Oxfordshire, UK
Page 1 of 2 https://www.njppp.com/?iid=2017-7-2.000&&jid=28&lng=
Online First Current Issue Archive Most Downloaded Most Accessed
« Previous Issue Next Issue »
Service by
Home Journal Issues Guide for Authors Editorial Board About Aims & Scope Editorial Contact
Natl J Physiol Pharm Pharmacol. Year: 2017, Volume: 7, Issue: 2
Review Article
1. Cardioprotective function of progesterone: A new perspective
Asha Anand Dharwadkar, Raghuram Ramkumar Chitterusu, Anand Rajendra Dharwadkar, Bindu Balakrishnan Chenmarathy, Kavitarati Anand Dharwadkar
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 136-142
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0927404102016
Original Research
2. Knowledge, attitude, and practice of adverse drug reaction reporting among nurses in a South Indian tertiary health-care center
Scandashree K, Praveen Kumar B, Padmaja Udaykumar, Tanya Mary Thomas Natl J Physiol Pharm Pharmacol. 2017; 7(2): 143-146
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0823819082016
3. Clinical effectiveness of olopatadine therapy in children with allergic conjunctivitis Scandashree K, Praveen Kumar B, Padmaja Udaykumar, Meghana Patil
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 147-150
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0823919082016
4. Study of drugs used in cerebral edema in patients with stroke at a tertiary care center Praveen Kumar B, Scandashree K, Padmaja Udaykumar
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 151-154
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0824619082016
5. Comparative assessment of glycemic control in hypertensive patients treated with or without statins Praveen Kumar B, Scandashree K, Padmaja Udaykumar
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 155-158
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0824719082016
6. Study of visual evoked potentials in patients with type 2 diabetes mellitus and diabetic retinopathy Rachula Daniel, Saravanan Ayyavoo, Bagavan Dass
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 159-164
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0824424082016
7. A prospective study of antibiotic sensitivity profile of pathogens isolated from surgical site infection at major surgical departments at tertiary care hospital
Mayur A Chaudhari, Shreya M Shah
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 165-169
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0709918082016
8. Role of serum uric acid and nitric oxide in the diagnosis of Type 2 diabetes mellitus - A case�control study Trilok Ranjan Srivastava, Ranjan Kumar Dixit
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 170-173
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0512210082016
9. A comparative study of impact of obesity on maximum voluntary ventilation in young adult women Malini M, Baljoshi V S, Kammar K F
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 174-177
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0719324082016
10. Causality, severity and preventability assessment of adverse drug reactions in patients received anti-retroviral therapy in a tertiary care hospital: A retrospective study
Abhishek Kumar, Lakhan Majhee, Manju Gari Natl J Physiol Pharm Pharmacol. 2017; 7(2): 178-182
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0821922082016
11. Evaluation of patterns and predictors of off-label prescribing of antidepressants in psychiatry at a tertiary care hospital - An analytical cross-sectional study
Debdipta Bose, Sushma Muraraiah, Hongali Chandrashekar Natl J Physiol Pharm Pharmacol. 2017; 7(2): 183-188
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0822216082016
12. Prescribing pattern and adverse events of drugs used in patients with primary open-angle glaucoma (POAG) attending a tertiary care hospital: Retrospective study
Seema Rai, Seemee Khilji, Lavanya G Rao, Puneet Hegde, Sarita R J Gonsalves, Tara V Shanbhag
AUTHOR LOGIN
Index Copernicus (ICV 2016: 109)
Geneva Foundation for Medical Education and Research
Chemical Abstracts Service (CAS)
Gale's Health Reference Center
Gale Info Trac
16/02/18 17.12 National Journal of Physiology, Pharmacy and Pharmacology
Page 2 of 2 https://www.njppp.com/?iid=2017-7-2.000&&jid=28&lng=
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 189-193
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0822624082016
13. Comparison of visual reaction time in myopic subjects with emmetropic subjects Saravanan Mohanraj, Aravindan Karthikeyan
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 194-197
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0824524082016
14. Study of prescribing patterns of hypolipidemic agents in a tertiary care teaching hospital in North India Seema Gupta, Rajesh Kumar, Dharminder Kumar, Sanjeev Bhat, Dinesh Kumar, Nusrat Kareem Bhat, Surbhi Mahajan Natl J Physiol Pharm Pharmacol. 2017; 7(2): 198-202
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0512830082016
15. Perception of stress in first-year MBBS, BDS, and BPTh students Seema Tanaji Methre, Nirmala Gopal Borade, Tanaji Sambhaji Methre Natl J Physiol Pharm Pharmacol. 2017; 7(2): 203-208
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0616630082016
16. A comparative study of gender difference in reaction time in response to exam stress among first-year medical students
Surendra S Wadikar, Parikshit A Muley, Pranjali P Muley Natl J Physiol Pharm Pharmacol. 2017; 7(2): 209-213
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0822429082016
17. Pattern of drug usage among medical students in Tumkur, Karnataka Rajesh B, Dharani Devangi R, Waseem Anjum
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 214-217
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0824827082016
18. Knowledge, attitude, and practice of pharmacovigilance among doctors in a tertiary care teaching hospital of Tripura Lakshman Das, Prithul Bhattacharjee, Ranjib Ghosh, Uttam Kumar Das, Tapasjyoti Ray
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 218-223
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0926912092016
19. Placenta previa, anemia, care in antenatal, employment score: Development of a scoring system to predict low birth weight in underserved area in Indonesia
Sarma Nursani Lumbanraja
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 224-227
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.030822316092016
20. A cross-sectional study of association of body mass index and VO2 max by nonexercise test in medical students Sunita Basavaraj Kalyanshetti, Sumalatha Veluru
Natl J Physiol Pharm Pharmacol. 2017; 7(2): 228-231
» Abstract » PDF Fulltext » doi: 10.5455/njppp.2017.7.0825804092016
Ind Medica
Scirus
Scientific Publication Index
Scientific Resources Database
Recent Science Index
Scholarly Journals Index
Directory of Academic Resources
Elite Scientific Journals Archives
Current Index to Scholarly Journals
Digital Journals Database
Academic Papers Database
Contemporary Research Index
Ayush Web Portal
CiteFactor
Journal Membership
World Association of Medical Editors (WAME), Dallas, Texas,
USA
Journal Listed in
ICMJE- International Committee of Medical Journal Editors
HIFA 2015 – Healthcare Information for All by 2015, Charlbury, Oxfordshire, UK
National Journal of Physiology, Pharmacy and Pharmacology 224 2017 | Vol 7 | Issue 2
RESEARCH ARTICLE
Placenta previa, anemia, care in antenatal, employment score:
Development of a scoring system to predict low birth weight in
underserved area in Indonesia
Sarma Nursani Lumbanraja
Department of Obstetrics and Gynecology, University of Sumatera Utara, Medan Baru, Sumatera Utara, Indonesia
Correspondence to: Sarma Nursani Lumbanraja, E-mail: [email protected]
Received: August 12, 2016; Accepted: September 16, 2016
ABSTRACT
Background: Early intervention of low birth weight (LBW) should reduce maternal and fetal morbidity. In underserved areas, with inadequacy of health technologies, it was very important to develop a simple scoring system based on the LBW risk factors. Aims and Objective: The aim of this study is to develop a scoring system to predict LBW in underserved area. Materials and Methods: This case–control study enrolled total of women with a singleton LBW in Padang Sidempuan General Hospital. For every case, the subsequent woman who delivered a baby weighing ≥2500 g acted as control. All data were by Chi-square or Fisher’s exact test. Significant variables were taken to be analyzed in backward stepwise binary regression. Then, receiver operating characteristic curve was developed to determine cutoff point and diagnostic value. This was done by SPSS (Statistical Product and Service Solutions, Chicago, IL, USA) 22.0 with 95% confidence interval significant value. Results: This study involved 62 LBW and 62 normal birth weight newborns. Among all variables, only four variables were found to be significant, such as employment, antenatal care, history of anemia in pregnancy, and history of placenta previa in pregnancy. The placenta previa, anemia, care in antenatal, employment (PACE) score was obtained as score for employment was +1, antenatal care was −2, history of anemia in pregnancy was +2, and history of placenta previa was +3. The cutoff point was determined as 0, where a positive score will predict fetal with LBW and total score ≤0 (negative) will predict fetal with normal weight. This model had sensitivity of 88.7%, specificity of 66.1%, and area under curve 0.844 (P < 0.001). Conclusion: Positive total score of PACE could be a promising predictor for LBW in underserved area.
KEY WORDS: Low Birth Weight; Placenta Previa, Anemia, Care in Antenatal, EmploymentScore; Predictor
INTRODUCTION
Low birth weight is defined as birth weight <2500 g (5.5 pounds). This is based on the World Health Organization
Access this article online
Website: www.njppp.com Quick Response code
DOI: 10.5455/njppp.2017.7.030822316092016
National Journal of Physiology, Pharmacy and Pharmacology Online 2016. © 2016 Sarma Nursani Lumbanraja et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creative commons.org/licenses/by/4.0/), allowing third partiesto copy and redistribute the materialin any medium or for mat and to remix, transform, and build upon the material for any purpose, even commercially, provided the original work is properly cited and states its license.
epidemiological observations that infants weighing <2500 g are approximately 20 times more likely to die than heavier babies.[1] Low birth weight (LBW) remains a major cause of neonatal morbidity and mortality. As many as 16% of newborns in worldwide to experience LBW with an incidence of 18 million annually. In developing countries, incidence of LBW was two times higher than in developed countries.[2] LBW can cause early life mortality and development of chronic diseases in the elderly.[3]
Lumbanraja PACE score predict low birth weight incidence
225 National Journal of Physiology, Pharmacy and Pharmacology 2017 | Vol 7 | Issue 2
<20 or >35 years old,[4] parity >3,[5] employed,[6] antenatal care <4 visits,[7] birth spacing >2 years,[5] and maternal morbidity (anemia, preeclampsia, and placenta previa).[8,9] In Indonesia, Trihardiani (2011) found no effect of maternal height with LBW.[10]
In underserved areas, which were still abundant in developing countries, clinicians should predict LBW as early as possible to reduce the morbidity and mortality of maternal and fetal. In these areas, we could not do the standardized diagnostic test; even many areas did not have ultrasonography device or electricity to operate it.
MATERIALS AND METHODS
This was an analytical, case–control study that conducted at Padang Sidempuan General Hospital from January to November 2015. This study has been approved by the Ethical Committee of University of Sumatera Utara. All LBW neonates born from January to November 2015 were approached to participate in this study. LBW is defined as weight below 2500 g. Birth weight was measured by a calibrated weight scale. Those women with malformed baby, HIV infection, and malignancy were excluded from this study. Others data were taken from medical records or structured interview. These participants were included in the case group. For every case, the subsequent woman who delivered a baby weighing ≥2500 g acted as control. The parameters taken were maternal age, parity, birth spacing, employment, antenatal care, history of anemia, placenta previa, abruptio placenta, and preeclampsia in pregnancy.
Data were analyzed by SPSS (Statistical Product and Service Solutions, Chicago, IL, USA) 22.0 for Windows. Categorical data were expressed as number and continuous data as mean ± standard deviation. The qualitative variables in this study were analyzed by Chi-square or Fisher’s exact test. Significant value was taken by 95%, and P < 0.05 was
considered significant.
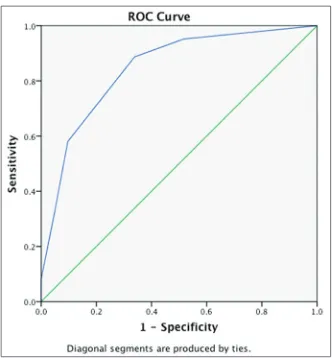
Figure 1 shows the Receiver Operating Curve from PACE Score. The area under curve (AUC) obtained was 0.844 with 88.7% and 66.1% as the best sensitivity and specificity, respectively.
All significant variables were taken to be analyzed in backward stepwise binary regression and Hosmer– Lemeshow test. A weighted score was then determined by Exp (B) from the logistic regression. Then, the weighted scores were simplified by their decimals to obtain simpler equation. Receiver operating characteristic curve was then being constructed to prove the diagnostic value of the scoring system. Cutoff point was determined using Youden index, with the best sensitivity and specificity value.
RESULTS
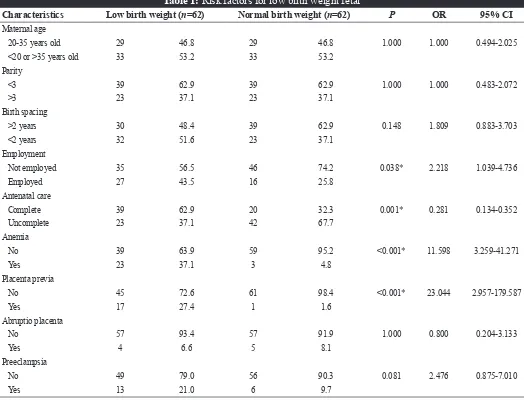
This study involved 62 LBW and 62 normal birth weight newborns. Association between LBW risk factors could be seen in Table 1.
To develop a scoring model using logistic regression (backward stepwise), we included all significant variables. Among all variables, only four variables were found to be significant, such as employment, antenatal care, history of anemia in pregnancy, and history of placenta previa in pregnancy.
In backward stepwise binary regression, all independent variables were found to affect LBW outcome by 43.8% (Nagelkerke R square). All variables, employment, antenatal care, history of anemia in pregnancy, and history of placenta previa, were significant (P = 0.038; P = 0.001; P < 0.001; and
P < 0.001). In this study, the models to predict LBW were
shown below:
y = 0.01+0.766 * Employment −1.747 * Antenatal care +2.127 * Anemia +3.023 * Placenta previa
Based on Hosmer–Lemeshow test, this model was well calibrated with P = 0.034, χ2 10.388. However, we simplified the equation to,
y = 1 * Employment −2 * Antenatal care +2 * Anemia +3 * Placenta previa
The cut-off point was taken by Youden index with the best sensitivity and specificity. We took 0 as the cutoff value, with sensitivity of 88.7% and specificity of 66.1%. Any participant with total score ≤0 (negative) will be said not to have LBW baby in upcoming delivery while participant with total score >0 (positive) will be said to have LBW baby in upcoming delivery. The area under curve (AUC) obtained was 0.844 (P < 0.001).
National Journal of Physiology, Pharmacy and Pharmacology 226 2017 | Vol 7 | Issue 2
DISCUSSION
In this study, a scoring model was developed to predict LBW baby in upcoming delivery. The scoring model was named placenta previa, anemia, care in antenatal, employment (PACE) score. From all risk factors of LBW, we found that only four variables, employment, antenatal care, history of anemia in pregnancy, and history of placenta previa in pregnancy, were significant, even after logistic regression. The weighted score for employment was +1, antenatal care was -2, history of anemia in pregnancy was +2, and history of placenta previa was +3. The constant 0.01 was omitted due to the low yield value. As seen in Table 2, we could be designed a scoring system.
All scores were summed. The maximal value was 6 and the minimal value was −2. The cutoff point was determined as 0, where a positive score will predict fetal with LBW and total score ≤0 (negative) will predict fetal with normal weight. This model had sensitivity of 88.7%, specificity of 66.1%, and AUC 0.844 (P < 0.001).
Antenatal care was the most interesting factor to be analyzed in this study. Isiugo-Abanihe and Oke (2011) found that low antenatal care visits were more associated with having LBW babies. About 27% of women with <6 antenatal care visits had LBW babies relative to 15% of those who had more than six ANC visits (χ2 = 23.6; P < 0.05).[11] Siza et al. (2008) also showed pregnant women who did not attend antenatal care service had about one-third (28.57%) of their neonates in the LBW group as compared with 13.78% of those who attended.[3] Mumbare et al. (2012) also emphasize inadequate ANC (odds ratio [OR] - 4.98, 95% confidence interval [CI] - 2.64-9.39) as one of the most significant risk factors for LBW along with maternal weight and height.[12] However, da Fonseca et al. (2014) found no association between adequacy of ANC and LBW.[13]
Although antenatal care is one of the most effective ways of reducing maternal and perinatal mortality and morbidity, this study found contradictory results in LBW pregnancy. Complete antenatal care increased the risk of having a LBW baby. The author assumed that mother who was felt that she
Table 1: Risk factors for low birth weight fetal
Characteristics Low birth weight (n=62) Normal birth weight (n=62) P OR 95% CI
Maternal age
20-35 years old 29 46.8 29 46.8 1.000 1.000 0.494-2.025
<20 or >35 years old 33 53.2 33 53.2
Parity
<3 39 62.9 39 62.9 1.000 1.000 0.483-2.072
>3 23 37.1 23 37.1
Birth spacing
>2 years 30 48.4 39 62.9 0.148 1.809 0.883-3.703
<2 years 32 51.6 23 37.1
Employment
Not employed 35 56.5 46 74.2 0.038* 2.218 1.039-4.736
Employed 27 43.5 16 25.8
Antenatal care
Complete 39 62.9 20 32.3 0.001* 0.281 0.134-0.352
Uncomplete 23 37.1 42 67.7
Anemia
No 39 63.9 59 95.2 <0.001* 11.598 3.259-41.271
Yes 23 37.1 3 4.8
Placenta previa
No 45 72.6 61 98.4 <0.001* 23.044 2.957-179.587
Yes 17 27.4 1 1.6
Abruptio placenta
No 57 93.4 57 91.9 1.000 0.800 0.204-3.133
Yes 4 6.6 5 8.1
Preeclampsia
No 49 79.0 56 90.3 0.081 2.476 0.875-7.010
Yes 13 21.0 6 9.7
Lumbanraja PACE score predict low birth weight incidence
227 National Journal of Physiology, Pharmacy and Pharmacology 2017 | Vol 7 | Issue 2
had high-risk pregnancy of threatened pregnancy would be more likely to control her pregnancy compared to the normal one. Triped et al. (2012) also showed antenatal care <4 visits was the significant protective factor of LBW in Maharat Nakhon Ratchasima Hospital. However, this would be bias results for LBW resulted from uncomplete antenatal care.[14]
Dooley and Prause (2010) showed that adverse employment change was associated with decreased intrauterine growth and weight gain due to poor nutrition of risky health behaviors by the mother. Employed mothers were also associated with more activities and less intake of nutrition. Stress in working could also contributed to have LBW babies.[6] Baum (2004), in the other hand, did not show any indirect effect of employment during pregnancy with LBW.[15]
Anemia and placenta previa were both associated with blood loss during pregnancy.[16] Elhassan et al. (2010) found that maternal anemia (OR = 9.0, 95% CI = 3.4-23.8; P < 0.001) was the main risk factor for LBW.[8] Lone et al. in a multivariate analysis of their study population showed that the risk of LBW babies in the anemic population was 1.9 times higher (95% CI = 1.0-3.4).[17] Kollman et al. (2013) found that in 328 patients with placenta previa and 35.6% would deliver LBW babies.[9]
Limitations in this study are the case–control design and the risk of recall bias. The strength of this study is the representative samples in underserved area with high incidence of LBW babies. The author hoped for the improvement of this PACE score.
CONCLUSION
Positive total score of PACE could be a promising predictor for LBW in underserved area.
REFERENCES
1. World Health Organization. Low Birth Weight: Country,
Regional, and Global Estimates. Available from: http://www. apps.who.int/iris/bitstream/10665/43184/1/9280638327.pdf/.
[Last accessed 2016 June 12].
2. Beddek F, Demmouche A, Mai AH, Ghani A, Benali A. Low
birth weight in Sidi Bel Abbes region (West of Algeria):
Retrospective study of 10008 deliveries. J Blood Disorders Transfus. 2014;5:1-4.
3. Siza JE. Risk factors associated with low birth weight of neonates among pregnant women attending a referral hospital
in Northern Tanzania. Tanzania J Health Res. 2008;10(1):1-8. 4. Feresu SA, Harlow SD, Woelk GB. Risk factors for prematurity
at Harare Maternity Hospital, Zimbabwe. Int J Epidemiol.
2004;33(6):1194-201.
5. Kazaura MR, Kidanto HL, Massawe SN. Levels, trends and risk
for early neonatal mortality at Muhimbili National Hospital,
Tanzania, 1999-2005. East Afr J Public Health. 2006;3:10-3.
6. Dooley D, Prause J. Birth weight and mothers’ adverse
employment change. J Health Soc Behav. 2005;46:141-55.
7. Chumnijarakij T, Nuchprayoon T, Chitinand S, Onthuam Y,
Sudan. BMC Res Notes. 2010;3:181.
9. Kollman M, Gaulhofer J, Lang U, Klaritsch P. Placenta previa: Incidence, risk factors, and outcome. J Matern Neonatal Med.
2013;34(1):1-4.
10. Trihardiani I. Risk factors for LBW in Puskesmas Singkawang.
Available from: https://www.core.ac.uk/download/
files/379/11731574.pdf. [Last accessed 2016 June 28].
11. Isiugo-Abanihe UC, Oke OA. Maternal and environmental factors influencing infant birth weight in Ibadan, Nigeria. Afr
Popul Stud. 2011;25(2):250-66.
12. Mumbare SS, Maindarkar G, Darade R, Yenge S, Tolani MK, Patole K. Maternal risk factors associated with term low birth weight neonates: A matched-pair case control study. Indian
Pediatr. 2012;49(1):25-8.
13. da Fonseca CR, Strufaldi MW, de Carvalho LR, Puccini RF. Adequacy of antenatal care and its relationship with low birth weight in Botucatu, São Paulo, Brazil: A case-control study.
BMC Pregnancy Childbirth. 2014;14:255.
14. Triped O, Arj-Ong S, Aswakul O. Maternal risk factors of low
birth weight at Maharat Nakhon Ratchasima hospital. Thai J Obstet Gynecol. 2012;20:12-20.
15. Baum CL. The effects of employment while pregnant on health at birth. Univ Middle Tennesse State. 2004. Available from: http://www.mtsu.edu/econfin/docs/working-papers/Ruhm%20
VII.pdf. [Last accessed 2016 June 30].
16. Jang DG, We JS, Shin JU, Choi YJ, Ko HS, Park IY, et al.
Maternal outcomes according to placental position in placental
previa. Int J Med Sci. 2011;8(5):439-44.
17. Lone FW, Qureshi RN, Emanual F. Maternal anaemia and its impact on perinatal outcome in a tertiary care hospital in
Pakistan. Trop Med Int Health. 2004;9(4):486-9.
How to cite this article: Lumbanraja SN. Placenta previa, anemia, care in antenatal, employment score: Development of a scoring system to predict low birth weight in underserved area in Indonesia. Natl J Physiol Pharm Pharmacol 2017;7(2):224-227.
Source of Support: Nil, Conflict of Interest: None declared.
Table 2: PACE score
Risk factor Category Score
Employment Employed 1
Not employed 0
Antenatal care Complete (≥4) −2
Uncomplete (<4) 0
History of anemia in pregnancy Yes 2
No 0
History of placenta previa in pregnancy Yes 3