The Role of Nuclear Medicine
in Diagnosis of the Diabetic Limb
1A. Hussein S. Kartamihardja Department of Nuclear Medicine Faculty of Medicine Universitas Padjadjaran
Dr. Hasan Sadikin General Hospital
Introduction
Diabetes mellitus is a systemic metabolic disease that is associated with significant complications affecting multiple organs and cause of cardiovascular disease, stroke, end-stage kidney disease, and lower extremity disease (diabetic limb), which lead to non-traumatic amputations. As the prevalence of diabetes increases, a number of important complications affecting lower extremity, such as foot infection are being more frequently and becoming a major worldwide health problem. Up to 15% of diabetic patients will develop foot ulcers, and about 15%–25% of these patients with severe forms of diabetic neuropathy require amputations. The foot of a diabetic patient has the potential risk of pathologic consequences, including infection, ulceration, and/or destruction of deep tissues associated.1,2
Diabetic foot infections require careful attention and integrated management
involving a multidisciplinary foot-care team. The team managing should include, or have
ready and direct access to specialist on infectious diseases or microbiologist. Diabetic foot
infections can potentially reduce the incidence of infection-related morbidities, the need for
and duration of hospitalization, and the incidence of amputation by adequate management.
An early and prompt diagnosis is very important and necessary in order antibiotic therapy, in conjunction with conservative surgery will give a benefit to cure diabetic limb and avoid amputation.2
There are several diagnostic modalities can be use in diabetic limb including imaging modalities. Imaging modalities for the diagnosis of diabetic limb can be divided into 2 goup. Imaging modalities based on anatomical changes and based on physiology and pathophysiology of the diseases. Nuclear medicine modalities have an important role in the management of diabetic limb.
Diabetic limb complications
There are 3 serious foot complications of diabetes mellitus, foot ulceration, infections and charcot neuropathic osteoarthropathy. Charcot foot may manifest as arthropathy, osteoarthropathy, neuroarthropathy. Non-infectious destruction of bone and joint in patients with diabetic limb usually associated with neuropathy, neurologic abnormalities, various degrees of peripheral vascular disease, and/or metabolic complications of diabetes in the lower limb. (Based upon the World Health Organization [WHO] definition.
The underlying pathophysiology of diabetic limb complications has been elucidated to a great extent. It is very important to determine which of treatments are most effective. How to effectively prevent those ulcerations, which are leading to amputation also very important.
Diagnosis of diabetic foot
Foot infection is a very serious and relatively frequent complication in diabetic
therapy, in conjunction with conservative surgery will give a benefit to cure diabetic limb and avoid amputation.1 Unfortunately, a prompt diagnosis in early stage of the disease is very difficult in the presence of diabetic osteopathy. Defining the location and extent of the infectious process is very important in deciding on the duration of antibiotic therapy and the need surgery for amputation.3
The detection of diabetic foot infection can’t be simple. It is difficult to differentiate between soft-tissue infection and osteomyelitis based on clinical examination only. Bone biopsy is the best modality, but it is not always performed, because it is an invasive procedure that loses its reliability when the biopsy fragment is contaminated by cutaneous bacteria. In this situation, Imaging modalities are valuable for the diagnosis and crucial in the evaluation of infections in DM.2
Several imaging modalities have been proposed to image foot infection in diabetic patients. These imaging diagnostic modalities could be divided into two groups, those are based on anatomical changes and physiology and pathophysiology of the disease.
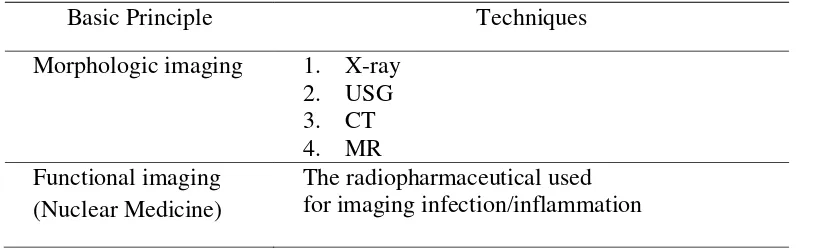
Table 1. Imaging of Diabetic Limb Osteomyelitis2
Basic Principle Techniques
Morphologic imaging 1. X-ray 2. USG 3. CT 4. MR Functional imaging
(Nuclear Medicine)
The radiopharmaceutical used for imaging infection/inflammation
Routine radiographic techniques have a low sensitivity since they do not reveal changes until the bone has been significantly eroded; furthermore a concomitant neuroarthropathy may hinder the radiological interpretation. 4
CT is one of imaging diagnostic modality based on anatomical can be used, but is not sufficiently accurate. MRI is also based on anatomical changes has high sensitivity and specificity, but has some limitations in differentiating osteomyelitis from neuropathic osteoarthropathy, from stress changes related to altered weight bearing, and from alterations of signal due to surgery.3
Nuclear medicine techniques
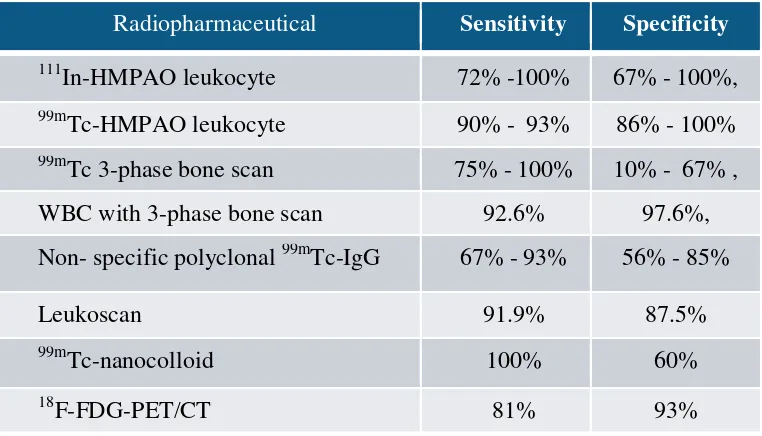
Nuclear medicine using gamma camera planar/SPECT system has an important role in the management of diabetic limb, particularly on the diagnosis of diabetic limb infection. Several radiopharmaceuticals can be use for imaging of infection. Following injection, radiopharmaceutical agent accumulates in the infectious/ inflammatory lesion due to the locally changed physiological condition. Table 2 shows various radiopharmaceutical can be use to image infection process.
Table 2: Radiopharmaceutical for diagnosis of diabetic limb.
Bone Scintigraphy
Bone scintigraphy is the most commonly performed nuclear medicine
procedure. The common radiopharmaceutical used for bone scintigraphy is
technetium-99m-labeled phosphonates. This radiopharmaceutical was introduce in
the early 1970s and responsible for the establishment of bone scanning as a major
diagnostic tool.5 Following injection of 99mTc-methylene diphosphonate (MDP), this
radiopharmaceutical has rapid blood clearance, excellent in vivo chemical stability,
and a high bone-to-soft tissue ratio, which are ideal for bone imaging.5 Bone
scintigraphy is a highly sensitive method for demonstrating disease in bone, often
permitting earlier diagnosis or demonstrating more lesions than are found by conventional
radiological methods.6
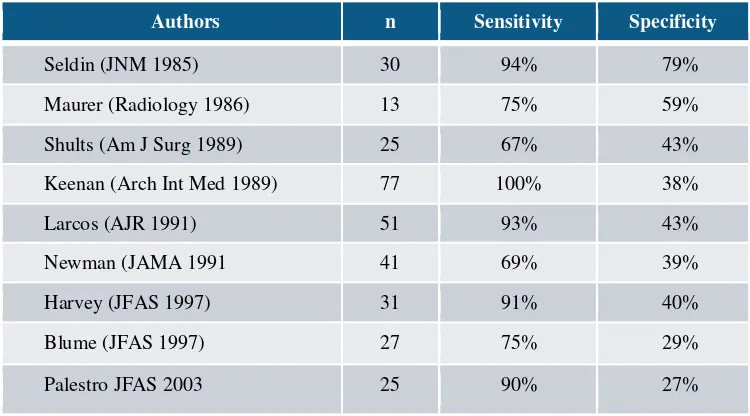
Table . Sensitivity and specificity of bone scan in the diagnose of diabetic limb
Authors n Sensitivity Specificity
Seldin (JNM 1985) 30 94% 79%
Maurer (Radiology 1986) 13 75% 59%
Shults (Am J Surg 1989) 25 67% 43%
Keenan (Arch Int Med 1989) 77 100% 38%
Larcos (AJR 1991) 51 93% 43%
Newman (JAMA 1991 41 69% 39%
Harvey (JFAS 1997) 31 91% 40%
Blume (JFAS 1997) 27 75% 29%
Palestro JFAS 2003 25 90% 27%
99m
Tc- HMPAO)–WBC scintigraphy
also used to image diabetic foot infection, but is often unable to differentiate bone from soft-tissue involvement. If the WBC-labelled scan was positive for osteomyelitis or if local therapy failed to heal the ulcer irrespective of the scan result, resection of the involved bone should be considered.4 Radiolabeled leukocytes scintigraphy is the nuclear medicine technique of choice to diagnose infection and define involvement of soft tissues and/or osteomyelitis. 99mTc-MDP is often used in association with labeled leukocyte scintigraphy to confirm or exclude the diagnosis of osteomyelitis. Combination this dual-isotope scans had a sensitivity of 92.6%, a specificity of 97.6% and accuracy 95.1%, while 99mTc-MDP alone had a sensitivity of 100%, a specificity of 28% and accuracy 62%.4 99mTc-MDP bone scans with the appropriate 111In-WBC scans can determine the site and extent of osteomyelitis in the neuropathic diabetic foot.7
Labeled leukocyte scintigraphy currently remains the gold standard imaging technique in patients with suspected diabetic foot infection.7
SPECT/CT Technology
SPECT/CT system is a technique to increas the accuracy of conventional scintigraphic imaging using planar gamma camera. SPECT system provide detail data throught 3 dimentional images with 3 sectional slices, sagital, coronal and horizontal slicing images. In this system, low dose CT is used to give detail anatomical information. SPECT/CT scan can be useful for imaging infectious processes, particularly when osteomyelitis is suspected in patients with diabetic limb.
18
F-FDG PET/CT SCAN
F-FDG (fluorodioxyglucoce). F-FDG behave similar to glucose will be uptake by any cell with high metabolic activity. 18F-FDG PET/CT scan has some theoretic advantages, such as no blood manipulation is necessary, acquisition time is shorter, and image resolution is higher compared to SPECT. 18F-FDG-PET is a highly specific complimentary imaging modality for the diagnosis of diabetic foot osteomyelitis, but due to its characteristic, it is impossible to distinguish infection from aseptic inflammation or malignancy. Quantitative parameter from PET scan such as SUVmax is not useful for differentiating soft-tissue infection from osteomyelitis as well as dual-time acquisition was not helpful. Combining visual assessment of PET and CT images was more useful.2
The data on the role of PET and PET/CT in the evaluation of diabetic foot infections are limited.8
Concluding Remarks
Radionuclide tests are decisive in the localization and diagnosis of foot osteomyelitis
99m
Tc-MDP and labeled leukocytes bone scans are the main imaging modalities employed, while emerging techniques include SPET/CT and, 18F-FDG-PET/CT.
Three phase bone scan is a useful clinical tool to assist the orthopedist in making a
more objective decision regarding the amputation level of ischemic lower limbs and surgical procedure to be employed, prior to surgery
SPECT/CT can represent a potential tool for diagnosing diabetic foot infection by 99m
Reference
1. Baker J et al. Diabetic musculoskeletal complications and their imaging mimics. RadioGraphics 2012; 32:1959-1974.
2. Familiari D, Glaudemans AWJM, Vitale V, et al. Can sequential F-18 FDG-PET/CT replace WBC imaging in the diabetic foot? J Nucl Med. 2011 (52) : 1012–1019. 3. Filippi L, Uccioli L, Giurato L, and Schillaci O. Diabetic Foot Infection: Usefulness of
SPECT/ CT for 99mTc-HMPAO-Labeled Leukocyte Imaging. J Nucl Med 2009; 50:1042–1046
4. Poirier JY, Garin E, Derrien C, Deviller A, Moisan A, Bourguet A and Maugendre D. Diagnosis of Osteomyelitis in the Diabetic Foot with a 99m Tc-HMPAO Leucocyte scintigraphy combined with 99m Tc-MDP Bone Scintigraphy. Diabetes Metab 2002.28.485-490.
5. Peller PJ, Ho VB and Kransdorf MJ. Extraosseus 99mTc-MDP Uptake: A Pathophysiologic Approached. RadioGraphics 1993. Volume 13 Number 4: 715-734 6. Bombardieri E, Aktolun C, Baum RP, Bishof-Delaloye A, Buscombe J, Chatal JF, et
al. Bone scintigraphy: procedure guidelines for tumour imaging. Eur J Nucl Med Mol
Imaging (2003) 30:BP99–BP106
7. Palestro CJ. 18F-FDG and Diabetic Foot Infections: The Verdict Is…J Nucl Med 2011; 52:1009-1011