W IRAWAN IMA, L ARSEN PD, A LDINGTON S, G RIFFITHS RF, E LLIS CJ. Cardiovascular risk score and cardiovascular events among airline pilots: a case-control study. Aviat Space Environ Med 2012; 83:465 – 71.
Background: A cardiovascular risk prediction score is routinely ap-plied by aviation authorities worldwide. We examined the accuracy of the Framingham-based risk chart used by the New Zealand Civil Avia-tion Authority in predicting cardiovascular events among airline pilots. Methods: A matched case-control design was applied to assess the as-sociation of 5-yr cardiovascular risk score and cardiovascular events in Oceania-based airline pilots. Cases were pilots with cardiovascular events as recorded on their medical records. Each case was age and gender matched with four controls that were randomly selected from the pilot population. To collect data before the events, 5-yr retrospective evaluations were conducted. Results: Over a 16-yr study period we identifi ed 15 cases of cardiovascular events, 9 (60%) of which were sud-den clinical presentations and only 6 (40%) of which were detected using cardiovascular screening. There were 8 cases (53%) and 16 con-trols (27%) who had a 5-yr risk of ⱖ 10 – 15%. Almost half of the events (7/15) occurred in pilots whose highest 5-yr risk was in the 5 – 10% range. Cases were 3.91 times more likely to have highest 5-yr risk score of ⱖ 10 – 15% than controls (OR 5 3.91, 95% CI 1.04 – 16.35). The accuracy of the highest risk scores were moderate (AUC 5 0.723, 95% CI 0.583 – 0.863). The cutoff point of 10% is valid, with a specifi city of 0.73, but low sen-sitivity (0.53). Conclusion: Despite a valid and appropriate cutoff point, the tool had low sensitivity and was unable to predict almost half of the cardiovascular events.
Keywords: assessment tool , Framingham risk score , risk stratifi cation , occupational group .
C
IVIL AVIATION authorities consider cardiovascu-lar disease (CVD) an important medical condition because of the risk of sudden pilot incapacitation ( 5,9 ). In addition, CVD has resulted in long-term disability and loss of license among commercial pilots ( 10 ). It has been reported that CVD accounts for almost half of the professional pilots who are declared to be “ long-term unfi t ” ( 20 ).Due to the critical nature of sudden incapacitation caused by CVD, airline pilots undergo an annual screen-ing examination. In New Zealand, the Civil Aviation Authority (CAA) requires an evaluation of the cardio-vascular risk of all medical certifi cate applicants who are over 35 yr of age ( 8 ). This is currently done using 5-yr CVD risk, calculated using the adjusted Framing-ham based method published by the New Zealand Guideline Group (NZGG) in 2003 ( 21 ) and updated in 2009 ( 22 ). The NZGG model predicts 5-yr CVD using the formula derived by Anderson et al. ( 2 ) and then ad-justment is made for a number of criteria, including family history of premature ischemic cardiovascular disease; being of Maori, Pacifi c, or Indian subcontinent
ethnicity; having diabetes and microalbuminuria; hav-ing type 2 diabetes for 10 yr or above; or havhav-ing type 2 diabetes and HbA1c consistently larger than or equal to 8% and having metabolic syndrome. An additional 5% CVD risk is then added to the calculated score. The NZGG method provides a 5-yr risk estimation and a 5-yr CVD risk of 10% (approximate 10-yr CVD risk of 20%) or higher is considered excessive for the purpose of the CAA medical standards. Pilots exceeding this threshold are required to undergo further investigations and normal myocardial perfusion needs to be demon-strated to gain a medical certifi cate ( 8 ).
However, there are questions regarding the accu-racy of the NZGG risk chart in the current era. The existing NZGG methods apply Framingham’s risk prediction tools, which are based on data collected more than 30 yr ago. There are also particular concerns about its validity due to the adjustments made by the NZGG to compensate for the infl uence of other possi-ble conditions. Although a previous study ( 19 ) had suggested that Framingham scores were fairly valid for the general population, very little evidence has been found on the accuracy of this method in occupa-tional groups, especially in the airline pilot popula-tion. Evidence that the current screening approach is working well would include a demonstration that the majority of CVD events are detected by screening and subsequent investigations, and not presenting as sud-den onset clinical events. This study examined CVD events occurring in a commercial pilot population and examined the sensitivity and specifi city of the current Framingham-based NZGG risk chart in predicting these events.
From the Occupational and Aviation Medicine Unit, Department of Medicine, University of Otago, Wellington, New Zealand; and the Occupational Health Department, School of Public Health, Faculty of Medicine, Udayana University, Bali, Indonesia.
This manuscript was received for review in October 2011 . It was accepted for publication in January 2012 .
Address correspondence and reprint requests to: Dr. Ady Wirawan, Occupational and Aviation Medicine Unit, Department of Medicine, University of Otago, 23A Mein Street, Newtown, Wellington 6021, New Zealand; [email protected].
Reprint & Copyright © by the Aerospace Medical Association, Alexandria, VA.
DOI: 10.3357/ASEM.3222.2012
Cardiovascular Risk Score and Cardiovascular Events
Among Airline Pilots: A Case-Control Study
METHODS
This study was approved by the Northern X Regional Ethics Committee of New Zealand as an observational study. In order to evaluate the utility of the current screening process in detecting significant CVD, we undertook a case-control study. Because CVD events are rare in this group and the number of potential controls is large, a matched pair design with multiple controls per case was chosen. Each case was age and gender matched to four controls.
Cases were pilots at an Oceania-based airline who experienced a CVD event as recorded on their medical examination reports. CVD events were defi ned as myo-cardial infarction (MI), angina pectoris, unstable angina, ischemic stroke, transient ischemic attack, peripheral vascular disease, congestive heart failure, cardiovascu-lar-related death, and revascularization. All but revascu-larization were the cardiovascular endpoints used in the Framingham study ( 2 ). Revascularization was included to capture pilots who were asymptomatic but under-went percutaneous coronary interventions or coronary artery bypass graft surgery on the basis of myocardial perfusion defi cits detected as a result of the screening process. All eligible cases were included as the sample. Controls were pilots who had not experienced CVD events and were randomly selected from the airline’s employee list and matched for age. Age at diagnosis for the cases were matched with the ages at inclusion for the controls, from which point the data collection was started and followed retrospectively until 5 yr before the diagnosis of the cases or inclusion date of the controls. Control subjects were excluded if their cardiovascular risk score data 5 yr before inclusion was not available or the recorded clinical data were not suffi cient to calculate the risk score.
The main independent variable was the CVD risk score as recorded during screening for medical certifi ca-tion. All CVD risk factor data needed to calculate NZGG risk scores were collected. These included data on age, gender, ethnicity, blood pressure, diabetes status, ciga-rette smoking history (if stopped smoking for , 12 mo,
assessed as a current smoker), total cholesterol, HDL cholesterol, and the total cholesterol-HDL ratio. Addi-tionally, data related to isolated elevated single risk fac-tors (such as total cholesterol ⱖ 8 mmol z L 2 1 , total cholesterol-HDL ratio ⱖ 8, and blood pressure consis-tently ⱖ 170/100) and presence of additional risk factors (including history of premature ischemic heart disease, diabetes with microalbumin, type 2 diabetes more than 10 yr or with HbA1c more than 8%, and metabolic syn-drome) was also collected. All CVD risk scores were then recalculated using the updated NZGG cardiovas-cular risk chart, which yields an estimate of 5-yr abso-lute CVD risk for individual pilots of any and all initial atherosclerotic CVD endpoints used in the Framingham study, such as MI, including silent and unrecognized MI; death from coronary heart disease (sudden or non-sudden); stroke, including ischemic stroke, hemorrhagic stroke, or transient ischemic attack; coronary insuffi ciency,
angina, peripheral artery disease, or congestive heart failure ( 22 ). The 5-yr risk estimations were presented as ordinal variables of , 2.5%, 2.5 – 5%, 5 – 10%, 10 – 15%, 15 –
20%, and . 20%. To collect data before the onset of CVD
events, 5-yr retrospective evaluations were conducted. Continuous data were analyzed with conditional logistic regression to account for the 1-n matched design with PASW 18 (IBM, NY) using the COXREG procedure ( 16 ). The categorical variables were analyzed using EpiInfo 3.5.3 (CDC, Atlanta, GA) to perform maximum likeli-hood estimate statistics with mid- P exact tests to account for 1-n matched design and the small sample size (less than 25 pairs) in this study ( 14 ). To measure the accuracy of the NZGG risk chart, the risk scores were entered as continuous data of 0, 2.5, 5, 10, 15, and 20. The sensitiv-ity, specifi csensitiv-ity, and area under the receiver operating characteristics (ROC) were drawn using PASW 18.
RESULTS
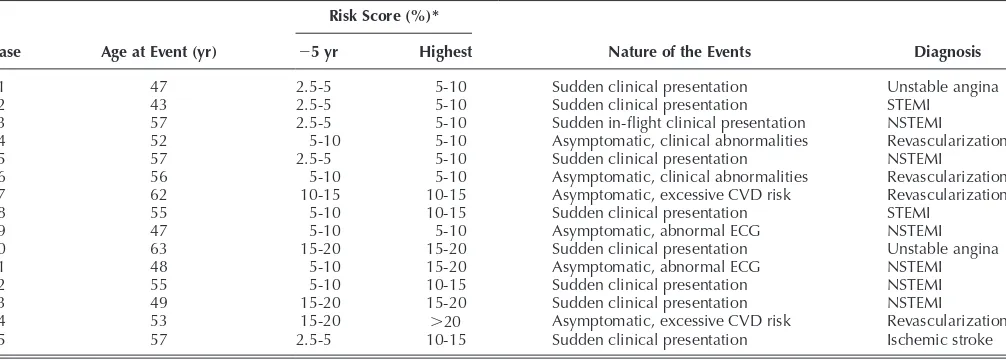
There were 15 cases with a cardiovascular event iden-tifi ed between 1994 and 2010. Each case was age and gender matched to 4 controls, resulting in 75 medical re-cords analyzed. The characteristics of the cardiovascular events among airline pilots are shown in Table I .
Among the 15 cardiovascular events, 8 were classifi ed as MI, 2 as unstable angina, 1 as ischemic stroke, and 4 as revascularization (3 percutaneous coronary inter-ventions with stents and 1 coronary artery bypass graft surgery). Nine (60.0%) cardiovascular events occurred as sudden clinical presentations. The other six cases were asymptomatic and detected through routine medi-cal screening; two (13.3%) cases had an excessive cardio-vascular risk score and four (26.7%) cases were the result of clinical or laboratory abnormalities detecting during screening.
Most of those with sudden clinical presentations were admitted or sought a medical practitioner and were re-ferred to hospitals due to having one or more symptoms such as chest pain, chest tightness, and shortness of breath. Two cases had ST segment elevation on their electrocardiograms and severe lesions on their coronary angiograms. Two pilots with unstable angina showed positive exercise stress on their ECGs and lesions on their coronary angiograms. The other cases were diag-nosed based on non-ST segment elevation changes on their ECGs and their elevated troponin level or creatine kinase, as well as severe lesions on their coronary angio-grams. One pilot was admitted to the hospital due to acute onset of right hemiplegia and severe dysphasia, and the brain scan showed multiple acute infarcts in the left middle cerebral artery territory. In one of the sudden clinical presentations, symptom onset occurred while the pilot was on duty in fl ight.
stressed nuclear scan, which demonstrated abnormal myocardial perfusion, hence a coronary angiography was undertaken and revealed occlusion of the dominant right coronary system and other severe lesions.
Of the four cases referred because of clinical or labora-tory abnormalities found during their medical screening process, one case had a 5-yr history of non-insulin-dependant diabetes mellitus and hyperlipidemia. This pi-lot was referred for an exercise stress nuclear scan, which showed a positive result; hence a coronary angiography was performed and demonstrated severe lesions. The second pilot was found to have high cholesterol and three computed tomography calcium scores that in-creased each time. This pilot was referred for an exercise stress ECG, which was suggestive of myocardial isch-emia at a high workload, but was not conclusive. There-fore, a coronary angiography was undertaken which demonstrated three signifi cant stenoses. The third and fourth pilots were found to have abnormal resting ECG, indicating old inferior myocardial infarctions. The exer-cise stress ECG results were normal for both pilots; hence coronary angiographies were undertaken which demonstrated severe lesions in both pilots.
Ages at diagnosis for the cases were exactly matched with the controls’ age at inclusion. For both groups, the ages ranged from 43 to 63 yr. The mean ages at inclusion for cases and controls was 53.4 yr (SD 5 5.7 yr) and 53.4
yr (SD 5 5.6 yr), respectively. The median (interquartile
range) of ages at inclusion for both groups was 55 yr (interquartile range 5 9 yr). The age at the review date
with the other characteristics of the cases and their con-trols in this study are shown in Table II . All of the cases and controls were men. It is interesting that nearly half of the cardiovascular events (47%) occurred in pilots ages 35-54 yr old.
There were some missing data on the continuous vari-ables in Table II . Analysis for these varivari-ables was per-formed from cases and controls with valid data only.
Glucose level data were not analyzed due to many missing data. However, the diabetes status was ob-tained from the medical records (a diagnosis of diabetes mellitus).
The variables that were statistically signifi cantly as-sociated with cardiovascular events include BMI 5 yr before the events (OR 5 1.32, 95% CI 1.02-1.70, P 5 0.03),
history of hypertension (OR 5 6.00, 95% CI 1.44, 30.17,
P 5 0.01), triglycerides at inclusion (OR 5 3.26, 95% CI
1.29-8.26, P 5 0.01), highest triglycerides during 5-yr
ret-rospective review (OR 5 1.87, 95% CI 1.06-3.29, P 5
0.03), and highest total cholesterol-HDL ratio during 5-yr retrospective review (OR 5 1.89, 95% CI 1.10-3.23, P 5
0.02). None of the controls were current smokers, com-pared to 20% of current smokers in the cases group. When current and past smoker were grouped, the asso-ciation between cigarette smoking status and cardiovas-cular events was statistically signifi cant (OR 5 4.34, 95%
CI 1.34, 15.10, P 5 0.01)
Table III presents 5-yr cardiovascular disease risk score data immediately before the events, 5 yr before the events, and the highest score during the 5-yr retrospec-tive review. We found that 8 cases (53%) and 16 controls (27%) had the highest 5-yr CVD risk of greater than 10%. Almost half of the events (7/15), however, occurred in pilots whose highest 5-yr CVD risk was in the 5 – 10% range. Based on the 95% confidence interval and P -value, the highest CVD risk score found during the 5-yr retrospective review was associated with increased cardiovascular events (OR 5 3.91, 95% CI 1.04-16.35,
P 5 0.04). Because cardiovascular events are rare among
airline pilots, the odds ratio is a good estimate of the risk ratio. We could, therefore, say that the risk of cardiovas-cular events among those with a 5-yr CVD risk score of 10 – 15% or more is 3.91 times greater than the risk among those with a 5-yr CVD risk score less than 10 – 15%, and we are 95% confi dent that the true risk is captured be-tween 1.04 and 16.35.
TABLE I. CARDIOVASCULAR EVENTS IN AIRLINE PILOTS.
Case Age at Event (yr)
Risk Score (%) *
Nature of the Events Diagnosis
2 5 yr Highest
1 47 2.5-5 5-10 Sudden clinical presentation Unstable angina
2 43 2.5-5 5-10 Sudden clinical presentation STEMI
3 57 2.5-5 5-10 Sudden in-fl ight clinical presentation NSTEMI
4 52 5-10 5-10 Asymptomatic, clinical abnormalities Revascularization
5 57 2.5-5 5-10 Sudden clinical presentation NSTEMI
6 56 5-10 5-10 Asymptomatic, clinical abnormalities Revascularization
7 62 10-15 10-15 Asymptomatic, excessive CVD risk Revascularization
8 55 5-10 10-15 Sudden clinical presentation STEMI
9 47 5-10 5-10 Asymptomatic, abnormal ECG NSTEMI
10 63 15-20 15-20 Sudden clinical presentation Unstable angina
11 48 5-10 15-20 Asymptomatic, abnormal ECG NSTEMI
12 55 5-10 10-15 Sudden clinical presentation NSTEMI
13 49 15-20 15-20 Sudden clinical presentation NSTEMI
14 53 15-20 . 20 Asymptomatic, excessive CVD risk Revascularization
15 57 2.5-5 10-15 Sudden clinical presentation Ischemic stroke
STEMI 5 ST segment elevation myocardial infarction; NSTEMI 5 Non-ST segment elevation myocardial infarction.
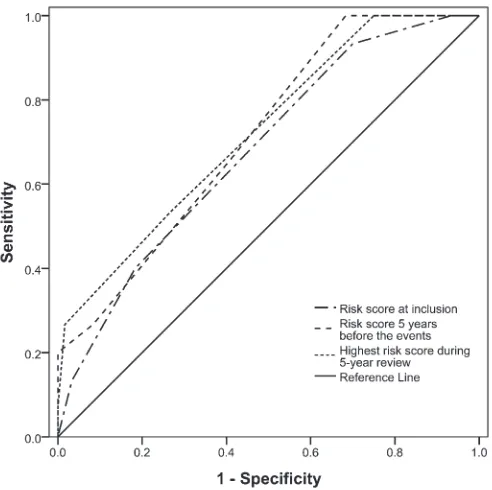
The area under the ROC curve (AUC) is illustrated in
Fig. 1 . It demonstrates that the AUC of CVD risk score 5 yr before the events is 0.714 (95% CI 0.580-0.848, P 5
0.01), the AUC of CVD risk score immediately before the events is 0.679 (95% CI 0.534-0.824, P 5 0.03), and
the AUC of the highest CVD risk score during the 5-yr retrospective review is 0.723 (95% CI 0.583-0.863, P 5
0.008). The diagnostics test showed that the cut point of 10% is preferred for CVD risk score immediately before the events and as the highest CVD risk score during the 5-yr retrospective review, with specifi cities of 0.82 and 0.73 respectively, albeit with low sensitivities (0.40 and 0.53, respectively). However, a cut point of 5% was more suitable for CVD risk score 5 yr before the events, although with sensitivity and specifi city of 0.67 and 0.58, respectively.
DISCUSSION
This study found that the incidence of CVD in this pilot cohort was low, with only 15 events in a 16-yr time period. However, the majority of cases presented as sud-den clinical events despite the annual cardiovascular risk assessment. Of the 15 cases, 1 occurred in fl ight, although
the event did not result in a pilot incapacitation. In eight (53%) of the cases, the highest CVD risk did exceed the 10% risk score at some point in the preceding 5-yr period, while only 27% of controls had a 5-yr risk score greater than 10%. While the risk score showed a reasonable level of specifi city, the sensitivity remained low.
Studies examining in-fl ight cardiovascular incapaci-tation have been few in number and the lack of good quality data limits our ability to make safety recom-mendations. A review of medical incapacitation and impairment studies indicated that from the articles based on in-fl ight medical events, the leading causes of fatal sudden incapacitation were MI, cardiac arrhyth-mia, and seizures ( 9 ). While the number of incapacita-tions that may occur is low, the potential consequences are so signifi cant that this remains a high risk area ( 5,9,20 ). This study suggests that the current process of screening for CVD is not effective at identifying clini-cally signifi cant disease, as more than half the cases were sudden clinical presentations.
The age of pilots experiencing a cardiovascular event in this study was quite young. Nearly half of them expe-rienced premature ischemic heart disease. Premature
TABLE III. FIVE-YEAR CVD RISK FROM THE FRAMINGHAM SCORE (WITH NZGG 2003/2009 ADJUSTMENTS).
Cardiovascular Disease Risk Score Case * ( N 5 15) Control * ( N 5 60) OR (95% CI) † P
Immediately before the events , 10 – 15% 9 (60.0) 49 (81.7) 1 0.08
ⱖ 10 – 15% 6 (40.0) 11 (18.3) 3.32 (0.84, 14.24)
5 yr before the events , 10 – 15% 11 (73.3) 55 (91.7) 1 0.06
ⱖ 10 – 15% 4 (26.7) 5 (8.3) 5.53 (0.89, 45.78)
Highest score during 5-yr retrospective review , 10 – 15% 7 (46.7) 44 (73.3) 1 0.04
ⱖ 10 – 15% 8 (53.3) 16 (26.7) 3.91 (1.04, 16.35)
* Data are presented as count and proportion within column (%).
† From MLE statistics with exact mid- P tests.
TABLE II. CHARACTERISTICS OF CASES WITH CARDIOVASCULAR EVENTS AND THEIR CONTROLS.
Characteristics Case * ( N 5 15) Control * ( N 5 60) OR (95%CI) † P
Age at review date (yr) 59.8 6 4.8 59.7 6 4.5 1.33 (0.55, 3.20) 0.53
Age at inclusion category, n (%)
35-44 yr 1 (6.7) 4 (6.7) NA NA
45-54 yr 6 (40.0) 24 (40.0)
55-64 yr 8 (53.3) 32 (53.3)
Flight time at inclusion (h) ‡ 14,576 6 3384 15,339 6 4084 1.00 (1.00, 1.00) 0.45
Current and past smoker, N (%) 8 (53.3) 11 (18.3) 4.34 (1.34, 15.10) 0.01
Alcohol at inclusion (units/wk) 7.2 6 4.0 5.9 6 4.3 1.09 (0.94, 1.26) 0.27
BMI 5 yr before event (mg · kg 2 2 ) 27.3 6 1.7 25.7 6 2.5 1.32 (1.02, 1.70) 0.03
Systolic BP 5 yr before event (mmHg) 127 6 13 130 6 12 0.98 (0.94, 1.03) 0.45
Diastolic BP 5 yr before event (mmHg) 80 6 6 79 6 7 1.02 (0.94, 1.11) 0.68
History of hypertension, N (%) 6 (40.0) 6 (10.0) 6.00 (1.44, 30.17) 0.01
TC 5 yr before events (mmol · L 2 1 ) 5.8
6 1.2 5.5 6 0.9 1.48 (0.80, 2.73) 0.22
HDL 5 yr before events (mmol · L 2 1 ) 1.2
6 0.3 1.3 6 0.3 0.37 (0.04, 3.93) 0.41
Triglycerides 5 yr before event (mmol · L 2 1 ) ‡ 1.8 6 0.8 1.5 6 0.7 2.09 (0.70, 6.27) 0.19
TC-HDL ratio 5 yr before event 5.1 6 1.9 4.4 6 1.1 1.62 (1.00, 2.64) 0.05
Diabetes, N (%) 2 (13.3) 1 (1.7) 8.00 (0.61, 235.98) 0.11
Family history of PIHD, n (%) 4 (26.7) 5 (8.3) 4.11 (0.82, 22.75) 0.08
TC 5 total cholesterol; HDL 5 high density lipoprotein cholesterol; PIHD 5 premature ischemic heart disease; NA 5 not available due to zero dis-cordances.
* Data are presented as mean 6 SD for continuous variables or count (proportion) for categorical variables.
† From univariate conditional logistic regression for continuous variables or MLE statistics with exact mid- P tests for categorical variables.
ischemic heart disease is defi ned as an event occurring before the age of 55 yr in men or 65 yr in women ( 22 ). Similarly, in a study of 275 Norwegian pilot groundings, of which 97 (35%) were for cardiovascular reasons, it was noted that the majority of the cardiovascular events occurred in the age range of 40 to 60 yr ( 4 ). This fi nding, however, supports a review result conducted by the Aerospace Medical Association on the “ Age 60 Rule ” that there is insuffi cient evidence to suggest restriction of pilot certifi cation based on age alone ( 1 ).
The highest score during the 5-yr retrospective review is preferred in this study, since cardiovascular events are predictable if the excessive risk score is present any time during the 5-yr period before an event. For the purpose of the New Zealand CAA medical standards, a cut-off point of 10% per 5 yr is considered to be excessive ( 8 ), while for the general population a cut-off point of 15% per 5 yr is used, as also stated on the NZGG risk chart ( 22 ). In spite of using a lower cut-off point, this study demonstrated that there is a statistically signifi cant as-sociation between cardiovascular events and highest cardiovascular risk score in the airline pilot population. In this study, 53% of pilots with an actual CVD event had a high 5-yr CVD risk of 10% or more. A similar fi g-ure was found in a population-based study in New Zea-land, where 44% of men with a risk of more than 10% had CVD events ( 19 ). Milne et al. also concluded that the Framingham based tool fairly accurately predicted a 5-yr risk of fi rst cardiovascular events in New Zealand men ages 35-74 yr at a population level ( 19 ). This study is the fi rst time that the NZGG risk assessment tool (a Framingham based method) was validated in an occu-pational group of airline pilots. This was accomplished by calculating the odds ratio of pilots with CVD events
who had a 5-yr CVD risk of 10% or greater and deter-mining the area under ROC curve, including the sensi-tivity and specifi city of the risk assessment tool. This fi nding indicates that the 5-yr CVD risk of 10% is appro-priate as a cut-off point to determine the need for further examinations and cardiovascular management in the airline pilot population. This is important since this level of risk in an asymptomatic pilot is similar to the level of risk in a patient with established CVD ( 23 ).
Despite a statistically signifi cant association, it should be noted that almost a half of the events (47%) occurred in pilots whose highest 5-yr risk during review was in the 5 – 10% range. Other methods might be needed to predict events among those in the Framingham based lower risk group. For example, the quantifi cation of cor-onary artery calcium score using non-invasive com-puted tomography (CT) is one of the methods that can improve risk prediction over the conventional risk pre-diction model, even in an asymptomatic population ( 3 ). Ellis et al. found that approximately 10 – 27% of patients with a low CVD risk score as assessed by the NZGG risk chart have a markedly increased calcium score and hence are actually at a high cardiovascular risk ( 11 ).
The diagnostic tests show the trade off between sensi-tivity and specifi city in determining the best cut-off point. Although the specifi city and the accuracy are moderate, the tool has low sensitivity. Similarly, the as-sessment of the NZGG risk chart in a general population indicated that its discriminative ability was also moder-ate (AUC 5 0.73, 95% CI 0.72-0.74) and the sensitivities
at a cut-off point of 10% and 15% were also low, despite good specifi city ( 18 ).
In the assessment of airline pilots, the International Civil Aviation Organization (ICAO) introduced the ap-plication of the “ 1% rule, ” a rule that does not allow probability of cardiovascular mortality of an individual to exceed 1% per annum ( 17 ). Because of the fl exibility of ICAO in the application of this rule and based on comprehensive reviews, the 2% per annum risk (or 10% per 5 yr) in airline pilot assessment has been applied in some ICAO contracting countries ( 17 ). The CAA of New Zealand based the decision to move to 2% per annum on a review conducted by Mr. Bruce Corkill (Wellington Barrister) and Dr. Simon Janvrin (UK CAA Medical), known as the Corkill-Janvrin Report, in 2002 ( 7 ). Simi-larly, the Transport Canada Civil Aviation Directorate has applied 20% per 10-yr risk (2% per annum) as a cut-off point for further cardiovascular examinations ( 24 ). A modeling of in-fl ight cardiovascular incapacitations in aircrew also suggested relaxing the maximum accept-able sudden incapacitation risk to 2% per year ( 20 ). The statistically signifi cant association between cardiovas-cular events and the 5-yr risk score of 10% or greater found in this study, as well as the moderate accuracy of the risk score, support the application of the 2% per annum risk in airline pilots. However, careful consider-ation should be taken with regard to the transportability of this risk prediction model and its direct applicability in the regulatory environment. The differences in char-acteristics from the Framingham sample population,
from which the risk assessment model is derived, and lower prevalence of risk factors found in airline pilots than in the general population are among those that should be taken into account ( 15 ).
It is important to note that detecting signifi cant latent CVD and intervening prior to a clinical event occurring is only one of the aims of a screening program. Arguably of equal or greater importance is the early identifi cation of cardiovascular risk, as appropriate life style modifi ca-tions and use of statins and antihypertensive medica-tions in this population may result in a signifi cant lowering of CVD risk across the whole cohort. This aspect of screening has not been investigated in the current study. A new recommendation to licensing authorities in the most recent revision of ICAO Annex 1 Standards and Recommended Practices relating to the content of medical examinations is to increase the em-phasis on health education and prevention of ill health ( 15 ). The result from this study is in support of this rec-ommendation to form a health promotion program so that CVD risk scores are properly communicated and understood by airline pilots.
The sample size for this study was quite small, which can lead to sparse-data bias. This, however, can be re-duced as only one parameter, i.e., cardiovascular risk score, was investigated in the fi nal analysis ( 13 ). In addi-tion, the small number of cases involved resulted in large 95% CIs. However, in a rare and fi xed number of cases a matched case-control design is appropriate and can increase the precision of the comparisons ( 6,12 ). Since the number of potential controls is quite large in this occupational group, the multiple controls per case can increase the power and effi ciency of this study ( 25 ). Furthermore, in order to make an appropriate analysis, we performed the mid- P exact test. This method can be used for binary outcome matched pair designs with fewer than 25 matched pairs ( 14 ).
As with any case-control design, this study is prone to confounding by external variables. A cardiovascular event is always an event resulting from the complex in-teraction of many factors, not only from risk factors that contribute to the cardiovascular risk score. Other factors to be considered include physical inactivity, obesity, ho-mocysteine level, psychosocial factors, lipoprotein(a), fi brinogen level, and C-reactive protein. Furthermore, retrospective analysis is always dependant on the accu-racy of the data in the records. We were also unable to investigate the complete treatment history and other possible comorbidities of the samples due to some miss-ing information. Biases to our results may be introduced by the above data limitations along with unmeasured confounding variables. The adjusted Framingham NZGG method is considered by the Civil Aviation Authority to be the most credible tool to be applied in New Zealand ( 8 ). However, risk prediction and validation have vari-ous complexities. We cannot completely accurately pre-dict a future cardiovascular event.
Utilizing a matched case-control design, we have quantifi ed the odds ratio of airline pilots with excessive cardiovascular risk and measured the accuracy of the
current practice in risk stratifi cation among this occupa-tional group. In spite of fairly appropriate cut-off points, the risk assessment tool had a low sensitivity and was unable to predict almost half of the events. More than half of the CVD events observed occurred as sudden clinical presentations. A major implication of the present study is that other methods are needed to increase the sensitivity of screening in addition to the conventional Framingham based risk score.
ACKNOWLEDGMENTS
The authors thank Dr. James Stanley, Biostatistical Services University of Otago Wellington, for his statistics assistance.
Authors and affi liations: I. Made Ady Wirawan, M.D., M.P.H., School of Public Health, Faculty of Medicine, Udayana University, Bali, Indonesia; Peter D. Larsen, B.Sc.(Hons.), Ph.D., Sarah Aldington, M.Av. Med., Ph.D., and Robin F. Griffi ths, M.B., Ch.B.,(Hons.), FAFOEM, Occupational and Aviation Medicine Unit, University of Otago, Wellington, New Zealand; Sarah Aldington, M.Av.Med., Ph.D., Air New Zealand Aviation Medicine Unit, Auckland, New Zealand; and Chris J. Ellis, BM, Green Lane CVS Service, Cardiology Department, Auckland City Hospital, Auckland, New Zealand.
REFERENCES
1. Aerospace Medical Association, Aviation Safety Committee, Civil Aviation Safety Subcommittee . The Age 60 Rule . Aviat Space Environ Med 2004 ; 75 : 708 – 15 .
2. Anderson KM, Odell PM, Wilson PWF, Kannel WB . Cardiovascular disease risk profiles . Am Heart J 1991 ; 121 ( 1, Pt. 2 ): 293 – 8 . 3. Arad Y, Goodman KJ, Roth M, Newstein D, Guerci AD . Coronary
calcifi cation, coronary disease risk factors, C-reactive protein, and atherosclerotic cardiovascular disease events: the St. Francis Heart Study . J Am Coll Cardiol 2005 ; 46 : 158 – 65 . 4. Årva P, Wagstaff AS . Medical disqualifi cation of 275 commercial
pilots: changing patterns over 20 years . Aviat Space Environ Med 2004 ; 75 : 791 – 4 . medical standards and certifi cation. Wellington, New Zealand: Civil Aviation Authority of New Zealand; 2006 .
8. Civil Aviation Authority of New Zealand . CAA medical information sheet: cardiovascular risk. Wellington, New Zealand: Civil Aviation Authority of New Zealand; 2010 .
9. DeJohn CA, Wolbrink AM, Larcher JG . In-fl ight medical inca-pacitation and impairment of airline pilots . Aviat Space Environ Med 2006 ; 77 : 1077 – 9 .
10. Ekstrand K, Boström P-A, Arborelius M, Nilsson J-Å, Lindell S-E . Cardiovascular risk factors in commercial fl ight aircrew offi cers compared with those in the general population . Angiology 1996 ; 47 : 1089 – 94 .
11. Ellis CJ, Legget ME, Edwards C, Pelt NV, Ormiston JA, et al. High calcium scores in patients with a low Framingham risk of cardiovascular (CVS) disease: implications for more accurate CVS risk assessment in New Zealand . N Z Med J 2011 ; 124 : 13 – 26 .
12. Fleiss JL . Statistical methods for rates and proportions. New York: Wiley; 1973 .
13. Greenland S, Schwartzbaum JA, Finkle WD . Problems due to small samples and sparse data in conditional logistic regression analysis . Am J Epidemiol 2000 ; 151 : 531 – 9 .
14. Hirji KF . A comparison of exact, mid-P, and score tests for matched case-control studies . Biometrics 1991 ; 47 : 487 – 96 .
15. Houston S, Mitchell S, Evans S . Application of a cardiovascular disease risk prediction model among commercial pilots . Aviat Space Environ Med 2010 ; 81 : 768 – 73 .
16. IBM . Conditional logistic regression using COXREG. Hampshire: IBM United Kingdom Limited; 2010 [updated 2010 15 November 2010]; accessed 2011 20 June from: https://www-304.ibm.com/ support/docview.wss?uid 5 swg21477360 .
Unedited Version. Montreal, Quebec, Canada: ICAO; 2008. Doc 8984-AN/895 .
18. Milne R, Gamble G, Whitlock G, Jackson R . Discriminative ability of a risk-prediction tool derived from the Framingham Heart Study compared with single risk factors . N Z Med J 2003 ; 116 ( 1185 ): U663 .
19. Milne R, Gamble G, Whitlock G, Jackson R . Framingham Heart Study risk equation predicts fi rst cardiovascular event rates in New Zealanders at the population level . N Z Med J 2003 ; 116 ( 1185 ): U662 .
20. Mitchell SJ, Evans AD . Flight safety and medical incapacitation risk of airline pilots . Aviat Space Environ Med 2004 ; 75 : 260 – 8 .
21. New Zealand Guideline Group . The assessment and management of cardiovascular risk. Wellington: New Zealand Guideline Group; 2003 .
22. New Zealand Guideline Group . New Zealand cardiovascular guidelines handbook: a summary resource for primary care
practitioners, 2nd ed. Wellington: New Zealand Guideline Group; 2009.
23. Pearson TA, Blair SN, Daniels SR, Eckel RH, Fair JM, et al. AHA Guidelines for Primary Prevention of Cardiovascular Disease and Stroke: 2002 update: Consensus Panel Guide to Compre-hensive Risk Reduction for Adult Patients Without Coronary or Other Atherosclerotic Vascular Diseases. American Heart Association Science Advisory and Coordinating Committee. Circulation 2002; 106:388-91.
24. Transport Canada . Guidelines for the assessment of cardio-vascular fi tness in licenced aviation personnel 2003, chapter 1: acute ischemic syndromes. Transport Canada; [20 May 2010]; accessed 2011 2 September from: http://www.tc.gc. ca/eng/civilaviation/publications/tp13312-2-cardiovascular-chapter1-2333.htm .