Scoliosis Correction for AIS Tips and Pitfalls
By; Tjokorda GB Mahadewa, MD., Ph.D.
Abstract
The author presents a review of scoliosis, incidence, diagnostic, conservative
management and operations, including the pitfalls that are often encountered. Although the
cases are done are relatively little that are 9 cases, but given the desire to share the difficulties
and obstacles encourage authors to submit at this meeting. The author does not intend to
teach but let's share and start doing scoliosis surgery in our cases should be studied properly,
is actually not difficult.
The success of surgery in these patients, the results were encouraging for both patient
and doctor. Calculation of appropriate corrections, outsmart wedge vertebra and
hemivertebra, mounting screw with anatomy based on landmarks and straighten the curve of
the spine is the most interesting part. If all can be done with either the patient can have a near
normal curve and is free from the difficulty of expanding lung or neurological deficits.
Scoliosis correction should also be done by a neurosurgeon spine, though not
uncommon, should be started immediately because the case is there and very challenging and
encouraging results so worth doing. Thorough knowledge of the anatomy of the spine
landmarks and strict selection of cases as indicated would support the results of patient
outcomes.
INTRODUCTION
Scoliosis is actually not a disease but an abnormal form or structure or curvature of
the spine. Treatment of scoliosis is still challenging. Primarily for neurosurgeons, still a few
of us who were involved in its handling. Generally scoliosis treatment performed by an
orthopedic spine, the authors learned to Korea at Samsung Medical Center (SMC) Hospital
under the guidance of Prof. Chung, Sung-Soo, which is the largest spine center there, in the
SMC POTENTIAL LEADERS In Spinal Surgery Program.
SCOLIOSIS
Most common is the Adult Idiopathic Scoliosis (AIS).
Approximately 2% of the population. The term idiopathic means a condition or disease with
no known cause. Sign and symptoms consist of the abnormality of curvature of the spine,
uneven shoulders or protrusion of one shoulder blade, asymmetry of the waistline and one hip
higher than the other.1-3
Radiology Assesment4
Conventional thoracolumbar X-rays are needed for diagnostic, etiology and
measurement using the Cobb Method thus determine the severity of scoliosis and progreesion
of the angle. The Scoliosis Research Society Classification of Severity of Scoliotic Curvature
Using the Cobb Method. Group Angle of Curvature i.e : I 20º; II 21º–30º; III 31º–50º; IV
51º–75º; V 76º–100º; VI 101º–125º; VII 125º.
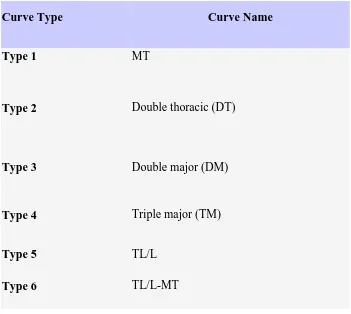
In 2001, Lenke proposed classification for AIS consist of 6 types including
Curve Type Curve Name
Type 1 MT
Type 2 Double thoracic (DT)
Type 3 Double major (DM)
Type 4 Triple major (TM)
Type 5 TL/L
Type 6 TL/L-MT
Table 1. Lenke Classification4
Differential Diagnosis:1
Congenital scoliosis, which is present in infants
Neuromuscular scoliosis, which is the results of neuromuscular conditions
Degenerative scoliosis, which occurs later in life
TREATMENT1-3
Mild curvature that remains at 20 degrees or less will most likely requires monitoring and observation, but further treatment is rarely needed.
Curvature greater than 20 degrees may require non-surgical or surgical intervention, including treatments such as a back brace for scoliosis or scoliosis surgery, both of
Thoraco-Lumbo-Sacral-Orthosis (TLSO)
Cervico-Thoraco-Lumbo-Sacral-Orthosis (known as a Milwaukee brace)
Charleston Bending Brace (Nightmare brace)
Surgical Anterior Vs Posterior approaches
Advantages:4
Not as many lumbar vertebral bodies will need to be fused and some additional motion segments can be preserved
Saving motion segments is especially important for lower back curves (lumbar spine), because if the fusion goes below L3 there is a higher risk of later back
pain and arthritis
Saving lumbar motion segments also helps prevent loading all the stress on just a few motion segments
This approach can sometimes allow for a better reduction of the curve and a more favorable cosmetic result.
The major disadvantage of the anterior approach4
Is that it can only be done for thoracolumbar curves, and most scoliotic curves are in the thoracic spine.
PITFALLS
Removing the discs allows for a better reduction of the spine and also results in a better fusion but some times too risky.
Without the anterior release procedure, the anterior column (the part of the spine facing the front of the body) can continue to grow, eventually twisting around the
fused, non-growing posterior spinal column, forming a new scoliosis curve (called
Somewhat difficult when using C-arm mounting screw for anatomical changes, preferably using only anatomical landmarks.
Fusion levels are key for preventing decompensation, as fusing the wrong levels is among the culprits of a postoperatively decompensated spine.4
Distal fusion levels are essentially based on the relationship between the end, neutral, and stable vertebrae of the distal structural curve to be fused. However, current
correction techniques employing pedicular fixation and derotation maneuvers often
allow for distal fusion levels to be saved by fusing one or two levels proximal to the
stable vertebra.4
CONCLUSION
The etiology of AIS remains unclear, as its diagnosis of exclusion implies. Once it has been diagnosed, follow-up with possible bracing or surgical intervention might be
warranted.1-4
Proper curve classification is imperative for proper surgical management.4
We also predicate that a selective fusion be carried out whenever possible; hence, curve analysis should be carried out from this perspective.4
Caring for this group of deformity patients is a very satisfactory undertaking, and when the aforementioned principles are employed, some of the shortcomings of
scoliosis surgery, such as decompensation and adding on of a fused curve, can be
avoided.4
REFERENCES
1. O'Brien MF, Newman, PO, "Nonsurgical Treatment of Idiopathic Scoliosis," Surgery
of the Pediatric Spine, ed. Daniel H. Kim et al. (Thieme Medical Publishers, 2008),
580.books.google.com.
2. Good CR, "The Genetic Basis of Idiopathic Scoliosis," Journal of the Spinal Research
Foundation, 2009:4:1:13-5,www.spinemd.com.
3. Types of Scoliosis braces. Available at
4. Thomas JE, Baron SL, Andrew WM. Surgical Management of Spinal Deformities.