VOLUME 53 November NUMBER 6
Original Article
Safety and immunogenicity of the DTP/HB /Hib
combination vaccine: phase I study
Kusnandi Rusmil,1 Eddy Fadlyana,1 Novilia Sjafri Bachtiar,2 Hadyana3
Abstract
Background 7KH :RUOG +HDOWK 2UJDQL]DWLRQ :+2 KDV
UHFRPPHQGHGWKHLQWURGXFWLRQRIKHSDWLWLV%+%DQGHaemophilus influenzaW\SHE+LEYDFFLQHVLQWRURXWLQHFKLOGKRRGYDFFLQDWLRQ
SURJUDPV$QHZGLSWKHULDWHWDQXVSHUWXVVLV'73KHSDWLWLV%+LE pentavalent combination vaccine has been developed.
Objective To evaluate the safety and immunogenicity of a new FRPELQDWLRQ'73+%+LEOLTXLGYDFFLQHLQLQIDQWV
MethodsAn open-label, uncontrolled, prospective intervention SKDVH,VWXG\ZDVFRQGXFWHGRQKHDOWK\LQIDQWVDJHGï ZHHNV(DFKVXEMHFWUHFHLYHGGRVHVRI'73+%+LEYDFFLQH IRUPXODWHG E\ %LR )DUPD P/ LQWUDPXVFXODUO\ DW WKH OHIW DQWHURODWHUDO WKLJK UHJLRQ XVLQJ D JDXJH QHHGOH RI PP OHQJWK6XEMHFWVZHUHIROORZHGIRUPRQWKDIWHUDGPLQLVWUDWLRQRI each vaccine dose to evaluate its safety, while serum anti-diphteria, tetanus, HB, Hib, and pertussis antibodies were measured prior WRWKHstGRVHDQGPRQWKDIWHUWKHrd dose.
Results$PRQJYDFFLQDWHGVXEMHFWVLQIDQWVKDGIHYHUZLWKLQ KRXUVDIWHUWKHILUVWYDFFLQDWLRQ0RVWFDVHVRIIHYHUZHUHPLOG LQLQWHQVLW\DQGUHVROYHGZLWKLQKRXUV1RRWKHUV\VWHPLFRU local reactions, or serious adverse events were observed in our VXEMHFWVGXULQJWKHVWXG\7KHLPPXQRJHQLFLW\UHVXOWVDIWHUrd vaccine dose showed that the geometric mean titer of the anti-SRO\ULERV\OULELWRO SKRVSKDWH 353 DQWLERG\ OHYHOV LQFUHDVHG VLJQLILFDQWO\IURPJP/WRJP/DIWHUYDFFLQDWLRQ and most infants had a fourfold or greater rise in antibody levels RYHUWKHLUSUHLQMHFWLRQOHYHOV$OOVXEMHFWVZKRUHFHLYHG'73 +%+LE OLTXLG YDFFLQH KDG VHURSURWHFWLYH DQWLERGLHV DJDLQVW WHWDQXV GLSKWKHULDD DQG KHSDWLWLV % ZKLOH LQIDQWV KDG seroprotective antibodies against pertussis.
Conclusion7KLVQHZGLSKWKHULDWHWDQXVSHUWXVLVKHSDWLWLV%+LE combination vaccine has excellent safety profile and antibody responses in infants. These results encourage further clinical evaluation in phase II. [Paediatr Indones. 2013;53:309-14.].
Keywords: DTP/HB/Hib vaccine, safety, immunogenicity, phase I
)URPWKH'HSDUWPHQWRI&KLOG+HDOWK3DGMDGMDUDQ8QLYHUVLW\0HGLFDO 6FKRRO+DVDQ 6DGLNLQ +RVSLWDO %DQGXQJ ,QGRQHVLD Surveillance &
Clinical Trial Division, BioFarma, Bandung, Indonesia,Department
(SLGHPLRORJ\ %LRVWDWLVWLFV 3DGMDGMDUDQ 8QLYHUVLW\ 0HGLFDO 6FKRRO
Hasan Sadikin Hospital, Bandung, Indonesia3.
Reprint requests to: Kusnandi Rusmil, Growth and Development Divison,
'HSDUWPHQW RI &KLOG +HDOWK 3DGMDGMDUDQ 8QLYHUVLW\ 0HGLFDO 6FKROO +DVDQ 6DGLNLQ +RVSLWDO %DQGXQJ -O 3DVWHXU %DQGXQJ 7HO )D[(PDLONXVQDQGL#KRUPDLOFRm.
G
lobal strategies for immunization againstGLSKWKHULDWHWDQXVDQGSHUWXVVLV'73 ZHUHDGRSWHGLQWKHODWHVDQGHDUO\ VXQGHUWKHDXVSLFHVRIWKH:+2
sponsored Expanded Program on Immunization
(3, 7KH WDUJHW ZDV WR DFKLHYH JOREDO '73
coverage with a three-dose vaccination schedule
LQ LQIDQWV DJHG OHVV WKDQ RQH \HDU E\ 7KLV
target has been achieved, though with considerable regional variation within the global target. The new
JRDO VHW UHFHQWO\ E\ WKH :+2 LV WR DFKLHYH
coverage with DTP vaccination of infants aged less
WKDQRQH\HDUE\WKH\HDU In countries where
hepatitis B is endemic, early infant immunization has also been recommended. Since the coverage
RI KHSDWLWLV % +% LPPXQL]DWLRQ LV PXFK ORZHU
in Indonesia, a combination of HB with DTP was considered to be a good way to increase the coverage of HB immunization. In Indonesia, the Lombok study
DGGLWLRQDVWXG\UHSRUWHGWKDWLQVXEMHFWVIURPWZR %DQGXQJVXEGLVWULFWVRIWKURDWVZDEVDPSOHV ZHUHSRVLWLYHIRUHaemophylus influenzae.4
The limited immunogenicity of the
polysaccha-ULGHDQWLSRO\ULERV\OULELWROSKRVSKDWH353YDFFLQH
in infants and young children led to the development
RIWKH+LESURWHLQFRQMXJDWHYDFFLQH&RQMXJDWLRQLV
the process of chemically bonding a polysaccharide, a somewhat ineffective antigen, to a protein carrier, a more effective antigen. This process changes the polysaccharide from a T-independent to a T-depen-dent antigen and greatly improves immunogenicity, particularly in young children.57KH+LEFRQMXJDWH vaccine is one such vaccine that can be used as part of EPI. It has dramatically reduced the incidence of Hib meningitis. This vaccine is given in a schedule of three doses during infancy, together with DPT, with or
ZLWKRXWDERRVWHUGRVHDWWKHDJHRIPRQWKV3,4 The aim of this trial was to assess the safety and
im-PXQRJHQLFLW\DIWHUWKUHHGRVHRI'73+%+LEYDFFLQH
formulated by Bio Farma.
Methods
This phase I of intervention study was conducted by the Department of Child Health at Hasan Sadikin
+RVSLWDOIURP$SULOWR$XJXVWDWWKHSULPDU\
health center (puskesmas LQ *DUXGD %DQGXQJ
Ethical clearance was obtained from the Ethics Committee of the Hasan Sadikin Hospital. The clinical trial protocol and vaccine were also approved by the Indonesian National Regulatory Affair. This trial was conducted in accordance with the latest Edinburgh, Scotland revision of the Declaration of Helsinki, International Conference on Harmonisation (,&+*RRG&OLQLFDO3UDFWLFHJXLGHOLQHV and local regulatory requirements.7KH VXEMHFWV LQYROYHG
LQWKLVVWXG\ZHUHKHDOWK\LQIDQWVDJHGïZHHNV ZKRVHSDUHQWVDJUHHGWRMRLQWKHVWXG\XQGHUVWRRG
the nature of the study and signed the informed
FRQVHQWIRUP(DFKVXEMHFWUHFHLYHGGRVHVRI'73 +%+LE YDFFLQH P/ LQWUDPXVFXODUO\ DW WKH OHIW DQWHURODWHUDO WKLJK UHJLRQ XVLQJ D JDXJH QHHGOH RIPPOHQJWK(DFKP/GRVHRIWKH'73+%
Hib vaccine contained purified diphtheria toxoid ( LQWHUQDWLRQDO XQLWV ,8 SXULILHG WHWDQXV toxoid (,8LQDFWLYDWHGB. pertussis whole-cell
suspension ( ,8 PFJ UHFRPELQDQW +%V$J
SURWHLQPJDOXPLQXPSKRVSKDWHPJVRGLXP FKORULGHDQGPJWKLPHURVDOSURGXFHGE\%LR )DUPDEDWFKQXPEHU7KHLQWHUYDORIHDFK GRVHZDVGD\V
6\VWHPLFDQGORFDOUHDFWLRQVZHUHHYDOXDWHGDW PLQXWHVDQGKRXUVDVZHOODVGD\VDIWHU LPPXQL]DWLRQ6XEMHFWVZHUHHYDOXDWHGDWWKHSULPDU\
health center for the first three days after the first immunization dose for adverse events. The reactions
EHWZHHQ GD\V DQG ZHUH UHFRUGHG LQ WKH GLDU\
cards collected and confirmed by the investigators at
WKHVXEMHFWV·ODVWYLVLWV5HDFWLRQVDIWHUWKHVHFRQGDQG WKLUGGRVHVZHUHUHFRUGHGRQWKHGLDU\FDUGIRU DQGKRXUVDVZHOODVGD\VDIWHULPPXQL]DWLRQ
%ORRGVSHFLPHQVZHUHWDNHQEHIRUHWKHVWLP
-PXQL]DWLRQDQGGD\VDIWHUWKHODVWLPPXQL]DWLRQ $QWLERG\WLWHUVWR3537RU+LEGLSKWKHULDDQGWHWD -nus were evaluated using the enzyme-linked
immuno-VRUEHQWDVVD\(/,6$PHWKRGDQGSHUWXVVLVDQWLERGLHV
were tested using a microagglutination method. All four methods had been validated and were done at the Clinical Trial Department of Bio Farma after blinding procedure. Anti-HB antibodies were tested using a kit from Abbott in a commercial laboratory which had been audited by Quality Assurance from Bio Farma. The original identity of the samples was concealed to ensure unbiased antibody testing.
7KH QXPEHU RI VXEMHFWV SURWHFWHG IURP +LE
diphtheria, tetanus, pertussis, and hepatitis B were calculated in percentages. Protective levels of Hib
DQWLERGLHVDUHJP/IRUDVKRUWWHUPSURWHFWLRQ DQGJP/IRUORQJWHUPSURWHFWLRQ For tetanus
DQGGLSKWKHULDSURWHFWLYHDQWLERG\OHYHOVDUH,8 P/IRUVKRUWWHUPSURWHFWLRQDQG,8P/IRUDORQJ WHUPSURWHFWLRQZKLOHWKDWIRU+%LVP,8P/
Seroconversion rates are calculated by the percentage
RI VXEMHFWV ZLWK D WUDQVLWLRQ IURP VHURQHJDWLYH WR VHURSRVLWLYHRUWKHSHUFHQWDJHRIVXEMHFWVZLWKIRXU
fold antibody increase after immunization. Geometric mean titers prior to immunization were compared to those after immunization.
Results
VXEMHFWVUHFHLYHGWKUHHGRVHVRI'73+%+LEOLTXLG
vaccine, and met the protocol criteria.
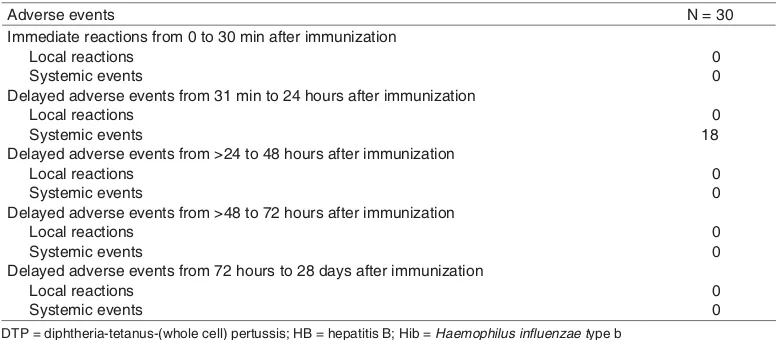
Adverse events reported after immunization are summarized in Table 11RVXEMHFWVSUHVHQWHG
with immediate local reactions or systemic events
IURPWRPLQXWHVDIWHULPPXQL]DWLRQ+RZHYHU VXEMHFWVSUHVHQWHGZLWKGHOD\HGV\VWHPLFHYHQWV PDLQO\LQWKHSHULRGIURPPLQXWHVWRKRXUV DIWHULPPXQL]DWLRQ)XUWKHUPRUHQRVXEMHFWVSUH -sented with immediate local reactions or systemic
HYHQWVIURP!KRXUVWRGD\VDIWHULPPXQL]D -tion and no serious adverse events were observed during the study.
After the 3rd LPPXQL]DWLRQ GRVH LQIDQWV were considered to be protected against Hib, as the
JHRPHWULFPHDQWLWHU*07RIDQWL+LELQFUHDVHG IURPJP/SUHLPPXQL]DWLRQWRJP/
post-immunization (Table 2).
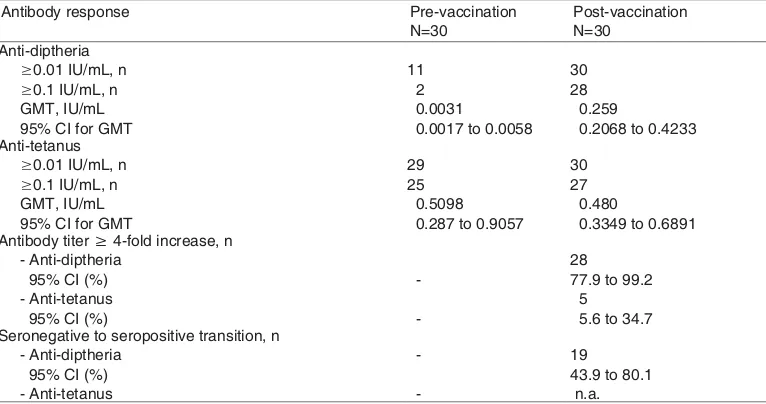
The proportions of infants who had post-immunization anti-diphtheria titers of ,8P/
DQG,8P/ZHUHDQGUHVSHFWLYHO\ 7KH*07RIDQWLGLSKWKHULDDQWLERGLHVZDVJ
mL post-immunization. The proportions of infants who had post-immunization anti-tetanus titers of
,8P/DQG,8P/ZHUHDQG
respectively. The GMT of anti-tetanus antibodies
ZDV JP/ SRVWLPPXQL]DWLRQ )XUWKHUPRUH WKH SURSRUWLRQV RI VXEMHFWV ZLWK !IROG LQFUHDVHG DQWLERG\ WLWHUV ZHUH IRU DQWLGLSWKHULD DQG IRU DQWLWHWDQXV :H DOVR REVHUYHG WKDW
infants underwent an anti-diphtheria transition from seronegative to seropositive (Table 3).
7KH DQWLSHUWXVVLV 37 *07 ZDV O G/ ZKLOH RI LQIDQWV SUHVHQWHG ZLWK DQWL37
titersG/SUHVHQWHGZLWKDQWL37WLWHUV
G/DQGSUHVHQWHGZLWKDQWL37WLWHUV
Table 1. 5WOOCT[QHCFXGTUGGXGPVUHQNNQYKPIVJGſTUVFQUGQH&62*$*KDXCEEKPG
Adverse events N = 30
Immediate reactions from 0 to 30 min after immunization Local reactions
Systemic events
Delayed adverse events from 31 min to 24 hours after immunization Local reactions
Systemic events
Delayed adverse events from >24 to 48 hours after immunization Local reactions
Systemic events
Delayed adverse events from >48 to 72 hours after immunization Local reactions
Systemic events
Delayed adverse events from 72 hours to 28 days after immunization Local reactions
Systemic events
0 0
0 18
0 0
0 0
0 0 &62FKRJVJGTKCVGVCPWUYJQNGEGNNRGTVWUUKU*$JGRCVKVKU$*KD*CGOQRJKNWUKPƀWGP\CGVype b
Table 2. #PVKDQF[TGURQPUGUVQVJG*KDEQORQPGPVRTGCPFRQUVXCEEKPCVKQPYKVJ&62*$*KD Antibody responses Pre-vaccination
N=30
Post-vaccination N=30 Anti-PRP >0.15 µg/mL, n
95% CI (%)
8 12.3 to 45.9
29 82.8 to 99.9 Anti-PRP >1.0 µg/mL, n
95% CI (%)
0 0 to 11.6
26 69.3 to 96.2
#PVK*KD)/6zIO.
95% CI (%)
0.0041
0.0015 to 0.0108
4.37
2.0635 to 9.2858
#PVKDQF[VKVGTŮHQNFKPETGCUGP
95% CI (%)
-27 73.5 to 97.9 Seronegative to seropositive transition, n
95% CI (%)
G/,QDGGLWLRQLQIDQWVKDGIROG
increased antibody titers (Table 4).
The proportion of infants with anti-hepatitis B
WLWHU!P,8/SRVWLPPXQL]DWLRQZDVWKH
*07 ZDV P,8P/ 3URSRUWLRQ RI VXEMHFWV ZLWKLQFUHDVLQJDQWLERG\WLWHUIROGZDVDQG VXEMHFWVH[SHULHQFHGWUDQVLWLRQRIVHURQHJDWLYH
to seropositive (Table 5).
Table 3. Serological responses to diphtheria and tetanus toxoid antigens, pre- and post- vaccination
YKVJ&62*$*KD
Antibody response Pre-vaccination N=30 Seronegative to seropositive transition, n
- Anti-diptheria
post-booster seroconversion rates).
n.a: percentage of infants presenting with anti-tetanus transition of seronegative to seropositive is not applicable, since all the subjects were protected before immunization
Table 4. #PVKDQF[TGURQPUGUVQVJGRGTVWUUKUEQORQPGPVRTGCPFRQUVXCEEKPCVKQPYKVJ&62*$
*KDXCEEKPG
Antibody response Pre-vaccination N=30
Post-vaccination N=30
GMT, l/dL 95% CI (%) Anti-PT >40 (1/dL) 95% CI (%)
104.448 to 212.3244 28
Table 5.#PVKDQF[TGURQPUGUVQVJGJGRCVKVKU$EQORQPGPVRTGCPFRQUVXCEEKPCVKQPYKVJ&62*$
*KDXCEEKPG
Antibody response Pre-vaccination N=30
Post-vaccination N=30
Anti-hepatitis B >10 mIU/L 95% CI (%)
(0.0007 to 0.0061)
547.898
(381.5926 to 786.8646) Antibody titer 4-fold increase, n
95% CI (%)
- 29
82.8 to 99.9 Seronegative to seropositive transition, n
95% CI (%)
- 27
73.5 to 97.9
&62Y*GR$*KDFKRJVJGTKCVGVCPWUYJQNGEGNNRGTVWUUKUJGRCVKVKU*CGOQRJKNWUKPƀWGP\C type B; IU= international unit; 4-fold
Discussion
The availability of combined vaccines containing
SURWHFWLYH DQWLJHQV DJDLQVW WKH PDMRULW\ RI DQG
ideally all, diseases for which universal immunization is recommended in infancy would simplify the implementation, increase the acceptance, reduce the global cost of immunization programs, and improve disease control, while offering the possibility of disease elimination or even pathogen eradication.Vaccine development proceeds through discovery, process engineering, toxicology, and animal studies to human phase I, II, and III trials. The human trials initially focus on safety, involving small groups of people
SKDVH,WKHQSURJUHVVWRPRGHUDWHVL]HG´WDUJHWµ
populations (persons close to the age and other
FKDUDFWHULVWLFV IRU ZKRP WKH YDFFLQH LV LQWHQGHG
to determine both safety and the stimulation of an
LPPXQH UHVSRQVH SKDVH ,, DQG ILQDOO\ WR ODUJH
target populations to establish whether a vaccine
DFWXDOO\ SUHYHQWV D GLVHDVH DV LQWHQGHG HIILFDF\ SKDVH,,,
$WRWDORIVXEMHFWVUHFHLYHGWKHLQYHVWLJDWLRQDO YDFFLQH FRQWDLQLQJ '73+%+LE IRU WKH ILUVW WLPH
in our phase I trial. All participants were intensively examined at the primary health care center during the
ILUVWKRXUVDIWHULQMHFWLRQ7KHUHVXOWVRIWKLVSKDVH
I study demonstrated good safety and immunogenicity
SURILOHVIRUWKHQHZFRPELQHG'73+%+LEYDFFLQH
There were no serious local or systemic reactions in this study. All observed reactions were slight,
WUDQVLHQWDQGGLGQRWODVWPRUHWKDQKRXUVDIWHU
the administration of the vaccine and resolved without medical intervention.
The anti-PRP antibody GMT significantly increased after the 3rd YDFFLQDWLRQ GRVH J mL, compared to the concentrations found in pre-vaccination sera, and most infants had a
4-fold-or-JUHDWHUULVHLQDQWLERG\OHYHOVRYHUWKHLUSUHLQMHFWLRQ OHYHOV$OOVXEMHFWVZKRUHFHLYHG'73+%+LEKDG
seroprotective antibodies against tetanus, diphtheria, and hepatitis B. We observed good immunogenicity and reactogenicity profiles for the new combined'73
+%+LEYDFFLQH
Combination vaccines have numerous
advan-WDJHV LQFOXGLQJ D GHFUHDVHG QXPEHU RI LQMHFWLRQV
increased compliance, better coverage, and simplified logistics. They also result in substantial reductions in
program costs, since the indirect costs of immunizing a child (e.g., logistics, materials involved, payment of
PHGLFDOVWDIIDQGFKLOGWUDQVSRUWDWLRQDUHIDUJUHDWHU WKDQWKHYDFFLQHVWKHPVHOYHV$QHZ'73Z+%+LE
combination vaccine for primary and booster vaccina-tion study of infants in Latin America showed that both vaccination regimens elicited excellent immune
UHVSRQVHVZLWKDOOVXEMHFWVLQERWKJURXSVDFKLHYLQJ
seroprotective anti-PRP antibody concentrations of
JP/RQHPRQWKDIWHUSULPDU\YDFFLQDWLRQ 7KHYDFFLQDWLRQUHJLPHQVFRQVLVWHGRI'73+%+LE
was given in one shot immunization in the left thigh
RIVXEMHFWDQG'73+%DQG+LEZDVJLYHQLQWZR
shots at the different thigh (e.e combined DTPw-HB
ZDVJLYHQLQOHIWWKLJKXVXDOO\DQG+LEZDVJLYHQLQ ULJKWWKLJK7KHFRPELQHG'73Z+%+LEYDFFLQH
was not inferior to licensed vaccines in terms of sero-protection, seropositivity, and vaccine response rates for all component antigens. Persistence of antibodies against all study vaccine antigens up to the time of booster vaccination was comparable between groups, and a marked increase of all antibody concentrations was observed after the booster dose. Both vaccine regimens were similar in terms of their overall reac-togenicity profiles.
7KH XVH RI WKH QHZ '73+%+LE YDFFLQH SURYLGHV SURWHFWLRQ DJDLQVW ILYH PDMRU FKLOGKRRG
pathogens and will ease the implementation of global pediatric immunization programs, with a minimum
RILQMHFWLRQVDQGSRWHQWLDOO\LPSURYHGLPPXQL]DWLRQ
coverage.
In conclusion, the excellent safety profile and antibody responses in the infants observed during this study encourage us to proceed to further clinical evaluations in phase II.
References
/RRNHU & DQG .HOO\ + 1RIDXOW FRPSHQVDWLRQ IROORZLQJ adverse events attributed to vaccination: a review of interna-WLRQDOSURJUDPPHV%XOO:RUOG+HDOWK2UJDQ
:RUOG +HDOWK 2UJDQL]DWLRQ +HSDWLWLV % 9DFFLQH :+2 :NO\(SLGHPLRO5HF
Indonesian children: hamlet-randomized vaccine-probe trial. /DQFHW
4. Kartasamita CB, Krishna E, Murad C, Sudigdoadi S, Rendieni Y. Haemophilus influenza serotypes distribution and antimi-crobial resistance in children with non-severe pneumonia. 3URFHHGLQJVRIWKHWK,QWHUQDWLRQDO&RQJUHVVRI3HGLDWULFV $XJXVW$WKHQV*UHHFH
:HQJHU-'+LJKWRZHU$:)DFNODP55*DYHQWD6%URRPH &9%DFWHULDOPHQLQJLWLVLQWKH8QLWHG6WDWHV5HSRUW of multistates surveillance study. The Bacterial meningitis 6WXG\*URXS-,QIHFW'LV
6. International Conference on Harmonization ICH Guidance (&KRLFHRI&RQWURO*URXSDQG5HODWHG,VVXHVLQ&OLQLFDO 7ULDOV>FLWHG)HE].$YDLODEOHIURPKWWSwww.ich.
RUJILOHDGPLQ,&+*XLGHOLQHV(SGf.
7. International Conference on Harmonization ICH Guideline. (WKQLFIDFWRUVLQWKHDFFHSWDELOLW\RIIRUHLJQFOLQLFDOGDWD( >FLWHG-DQ@$YDLODEOHIURPKWWSZZZLFKRUJ/2% PHGLD0(',$SGI
,QWHUQDWLRQDO&RQIHUHQFHRQ+DUPRQL]DWLRQ,&+*XLGHOLQH Clinical Safety Data Management Definition and Standards IRU([SHGLWHG5HSRUWLQJ($>FLWHG-DQ@$YDLODEOH IURPKWWSSULYDWHLFKRUJ/2%PHGLD0(',$SGI %320%DGDQ3HQJDZDV2EDWGDQ0DNDQDQ3HGRPDQ
&DUD8ML.OLQLN\DQJ%DLN&8.%GL,QGRQHVLD*XLGHOLQHV IRU*RRG&OLQLFDO3UDFWLFHLQ,QGRQHVLD-DNDUWD,QGRQHVLD
/HTXLQ ´(Q]\PH LPPXQRDVVD\ (,$HQ]\PHOLQNHG LP-PXQRVRUEHQWDVVD\(/,6$µ&OLQ&KHP *DOD]ND$07KHLPPXQRORJLFDOEDVLVIRULPPXQLVDWLRQ
VHULHV0RGXOH'LSKWKHULD:+2(3,*(1*HQHYD S
+RUQH$'/DFKHQEUXFK3$*HVQHU35+VX+6$QDO\VLV of studies to evaluate immune response to combination vac-FLQH&OLQ,QIHFW'LV6
*UDQRII'0$VVHVLQJHIILFDF\RI+DHPRSKLOXVLQIOXHQ]DH W\SHEFRPELQDWLRQYDFFLQHV&OLQ,QIHFW'LV6
)DLQJH]LDVW , $YLOD$TXRUUR 0/ &HUYDQWHV < )RXUQHDX Marc, Costa-Clemens Sue Ann. Primary & booster vac-FLQDWLRQZLWK'73Z+%+LESHQWDYDOHQWYDFFLQHLQ&RVWD Rican children who had received a birth dose of hepatitis B YDFFLQH3DQ$P-3XEOLF+HDOWKï 'RXJODV5*6DGRII-6DPDQW97KHYDFFLQHLQGXVWU\,Q
Plotkin S, Orenstien W, Offit P, editors. Vaccines. Amster-GDP(OVHYLHUS
7UHJQDJKL0/ySH]35RFKD&5LYHUD/3LHUUH'DYLG0 5WWLPDQQ 5 DQG 6FKXHUPDQ / $ QHZ '73Z+%+LE combination vaccine for primary and booster vaccination of LQIDQWVLQ/DWLQ$PHULFD5HY3DQDP6DOXG3XEOLFD