1
EXECUTIVE SUMMARY
Papua Health Worker Survey: Results of a study in four districts
When community health centers (puskesmas) were introduced in Indonesia in 1968, they were to function
as a focal point for community health development activities. As this infrastructure and manpower was
expanded across the country, community health centers increasingly served curative, primary-care
functions. With puskesmas now in nearly every sub-district (kecamatan), they are the backbone of the government’s primary- and preventive-care systems. For poor and rural communities, they are often the principal if not the only source of primary care. With decentralization introduced into Indonesia in 2000,
district/city health offices became administratively responsible for the operation and oversight of community
health centers.
Ensuring adequate numbers of health workers, as well as their
rational distribution and competence, contributes significantly to
the proper functioning of this primary-care system. Health workers
also need to be consistently present at their assigned posts in order for the system’s functioning to translate into achievements in terms of overall health provision and meeting development
objectives. The phenomenon of habitual absence among some
health workers from the workplace causes inequitable access to
public services and impacts the formation of human capital.
Addressing this problem must, therefore, figure prominently in
development planning and programming. Papua’s unique
geographical landscape, socio-cultural diversity and security
conditions present additional challenges to addressing health
worker absenteeism in the province.
Intervening in an effort to reduce absenteeism requires knowledge
of the magnitude of absenteeism and the characteristics of health
Important findings
Overall health worker
absenteeism: 30.7%
Most absent: Midwives (33%)
Highest absenteeism rate:
Jayapura District (49%)
Lowest absenteeism rate:
Jayapura City (14.5%)
Female-headed puskesmas
experienced less absenteeism
Remote puskesmas experienced
highest levels of absenteeism
Male health workers were
absent more often than female
2
providers where absenteeism rates are high. It also requires an in-depth understanding of why
absenteeism occurs and the contributory policy roots. This study was conducted to provide the evidence
needed to develop initiatives that reduce absenteeism and improve the delivery of frontline health services
to communities. Evidence from this study is intended for use by district governments to address gaps in
local service delivery and to deliver services that are more responsive to local needs and preferences.
Methodology
The study was conducted in four districts in the province of Papua: Jayapura City, Jayapura District, Jayawijaya District and Mimika District. In total, 50 community health centers participated in the study (12 in Jayapura City, 16 in Jayapura District, 13 in Jayawijaya, and 9 in Mimika), including health centers categorized by DHOs as “urban”, “rural”, “remote” and “very remote”. A total of 577 health workers were interviewed from a target of 611.
A combination of quantitative and qualitative methods was used for this study. The quantitative component
included face-to-face, structured interviews with doctors, nurses and midwives practicing at community
health centers (“health workers”), heads of those health centers and health facility assessments. A “practicing” health worker was defined as someone who was currently assigned to provide direct diagnoses and treatment to patients. An unannounced, initial visit to each of the targeted puskesmas by the survey
team established which health workers were scheduled to be providing patient services at that time and
whether they were present or absent. Those present were interviewed upon the completion of their patient
responsibilities that day. Absent workers were sought upon a second visit to the health center and
interviewed if they were then present. If they were found to be absent once again, they were traced to their
recorded home address or another location and interviewed there.
Kinerja Papua provided the study team with initial rosters of doctors, nurses and midwives for each of the
sample community health centers. They obtained these rosters in December 2013 from the DHOs in each
of the four study districts. These initial rosters were verified upon the first, unannounced visit at each
puskesmas through an interview with the head of the health center or his/her representative if s/he was
absent. The names of new health workers reported by each puskesmas head were added to the roster,
while the names of health workers reported as no longer employed at the health center were dropped from
3
worker (see Section 2.1). Volunteers and interns were included as practicing health workers on the final,
verified roster. A total of 127 doctors, 699 nurses and 365 midwives working at the 50 sample community
health centers met the definition of practicing health workers. Of these, 99 doctors, 407 nurses and 262 midwives were scheduled to be working at the time of the survey team’s first, unannounced visit to each puskesmas. Health worker absenteeism was calculated on this sample of practicing health workers that were scheduled to be working at their assigned community health centers at the time of the survey team’s first health-center visit.
Table 1: Health Worker Sampling Frame and Targeted Sample Sizes
Health Services to Patients
Type of Interview (present or absent
health worker)
Interviews were conducted with a sub-sample of these health workers in order to obtain information about
absenteeism correlates. All of the practicing doctors and midwives scheduled to be working at the time of the survey team’s first visit were targeted for interviews. A random sample of two present and two absent nurses, who were scheduled to provide services at the puskesmas, was drawn from each health center’s final nurses’ sample frame. Additionally, all nurses reportedly assigned to offer community-based services at the time of the survey team’s first visit were targeted for interview, to determine whether or not they had been so assigned and were not in fact absent.
The qualitative component included male and female focus group discussions (FGDs) with community
members and one-on-one, in-depth interviews with community leaders. These tools were designed to
obtain community perspectives on puskesmas services and health worker absenteeism. FGD participants
4
during the previous one month, as well as community members who had not been ill during the past month
but who had previously used their community health center’s services. In-depth interviews, one per
health-center community, targeted male and female community leaders.
Respondents to both the quantitative and qualitative components were asked for their opinions on
interventions that could help reduce health worker absenteeism at puskesmas.
Results
Health worker presence/absence was measured during the survey team’s unannounced, first visit to each
community health center. Overall, 30.7 percent of practicing health workers (doctors, nurses and midwives) were found to be absent during the survey team’s first health center visits. The results
presented here likely underestimate absenteeism among health workers because we only recorded their
presence/absence between the hours of 9:30 a.m. and 10:30 a.m. Monday to Friday. Although official
patient-service hours are 8 a.m. to 2 p.m., we observed that few health workers were present before 9 a.m.
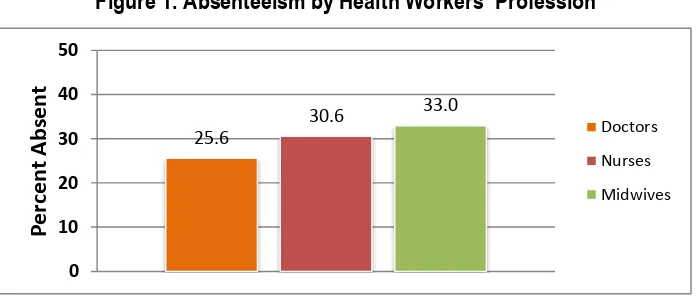
and most left their assigned puskesmas before noon. Absenteeism was lowest among doctors (26 percent) and highest among midwives (33 percent). Jayapura District saw the highest absenteeism rates, while Jayapura City experienced the lowest.
Figure 1. Absenteeism by Health Workers’ Profession
5
Figure 2: Absenteeism by District
The most common reasons given by health workers for their absence included attending trainings and
job-related meetings, official leave, family illness, safety concerns about travelling to the center, lack of
transportation, commitments to their own private practices, and inclement weather. Many also admitted that
they were absent because they were performing non-work activities or that they did not have a good reason
for being absent. Community members, on the other hand, mostly thought that health workers were absent
because they or a family member was ill, or because of safety concerns, transportation issues, or
community conflict.
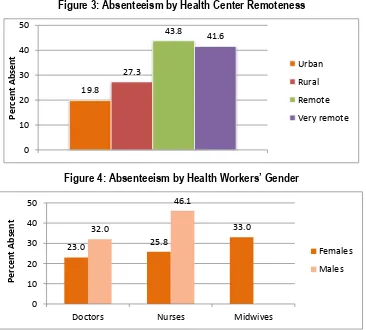
Figure 3: Absenteeism by Health Center Remoteness
Figure 4: Absenteeism by Health Workers’ Gender
6
Figure 5: Absenteeism by Number of Years Working as a Health-Care Provider
Figure 1: Absenteeism by Health Workers’ Job Satisfaction
Figure 7: Absenteeism by Health Workers’ Residential Location
There is a clear link between distance and absenteeism. Among present workers, absenteeism rates were
7
were greater than Rp 50,000 (US$4.15). Among absent workers, absenteeism rates increased slowly in
line with travel costs up to Rp 50,000, and then rose considerably when the costs exceeded Rp 50,000.
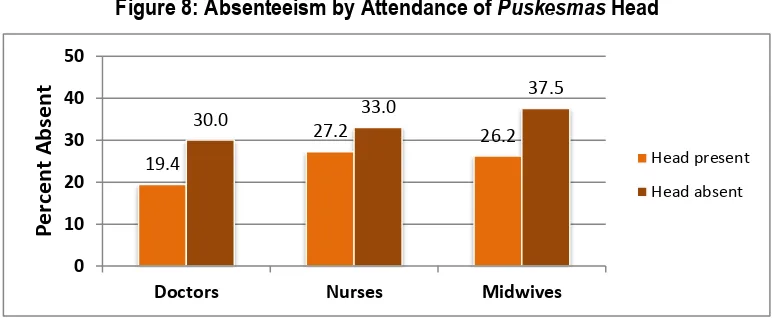
Figure 8: Absenteeism by Attendance of Puskesmas Head
Absenteeism among health workers was uniformly higher at health centers where the head was also
absent. Additionally, absenteeism was highest – among doctors, nurses and midwives - when the health
center head was a nurse. Among doctors and midwives, absenteeism was lowest when the head was a
midwife. For all health workers, absenteeism was lower in health centers headed by women.
Conclusion
Based on this survey’s findings, one can create a general profile of those health workers who are more likely to be absent. They are more likely to be non-Papua-born, male health workers who have been
practicing for between three and five years and who express high levels of dissatisfaction with their jobs.
They tend to be staff that live further away from their assigned health centers.
This study also found a number of environmental correlates. Poor health-facility conditions were found to
be associated with higher absenteeism. As worker satisfaction is in part driven by structural and material
conditions at puskesmas, improving these conditions could improve both job satisfaction among health
workers as well as reduce absenteeism.
Improving the managerial environment at puskesmas presents another opportunity. It is clear that
absenteeism is lower when the head of a puskesmas is not absent; in other words, leadership by example
matters. It appears that certain types of puskesmas heads are more effective at curbing absenteeism. For
8
combinations of workers and who leads them are also associated with different levels of absenteeism.
Midwives seem to do best at motivating other midwives to show up for work while overall, nurses seem to
be least effective with this managerial responsibility.
The evidence presented here favors solutions that are not only rooted in disciplinary action against
underperforming health workers, but also in measures that can improve health-center facilities, managerial
competence and surrounding environmental factors. Policymakers should take these factors into