Analisis Faktor yang Mempengaruhi Penurunan Angka Kematian Bayi di Indonesia
Periode : 1991 – 2014
Daniel A. Talmera 1110512020
Ilmu Ekonomi Universitas Andalas
Padang Indonesia
Abstract
Infant mortality rate (IMR) is an indicator of the quality of population health. This study purposed to determine the level of infant mortality rates and to examine the efect of macroeconomic, demographic, and environmental policy on the health status of the children under fve years in Indonesia. The data for this study were collected from secondary party like WHO, World Bank, and Ministry of Health of Indonesia, the data were analyzed statistically using Least-Square method. The result shows that Improved Sanitation Facilities, Government Expenditure, and Women’s Education are efectively reducing the IMR in Indonesia.
Background
Infant mortality rate is the number of infants dying before reaching one year of age, per 1,000 live births in a given year. Infant mortality rate (IMR) is generally regarded as an important national indicator of health because it is particularly sensitive to general structural factors, like socio-economic development and basic living conditions. The leading causes of infant mortality are birth asphyxia, pneumonia, pre-term birth complications, diarrhoea, malaria, measles and malnutrition1. Many factors contribute to
infant mortality such as the mother's level of education, environmental conditions, and political and medical infrastructure. Improving sanitation, access to clean drinking water, immunization against infectious diseases, and other public health measures could help reduce high rates of infant mortality.
The infant mortality rate is one of three indicators used to monitor achievements towards the Fourth Goal of the eight Millennium Development Goals. This goal's target value is to "Reduce by two-thirds, between 1990 and 2015, the under-fve mortality rate".
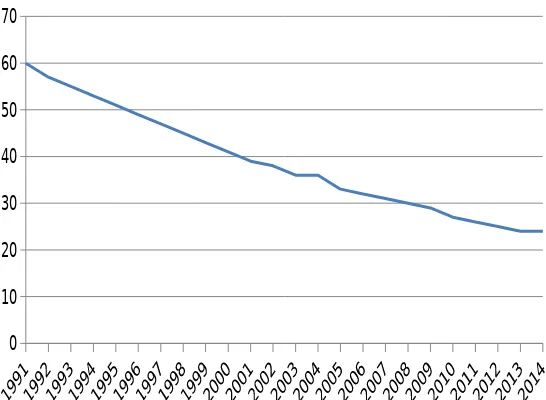
Table 1
0 10 20 30 40 50 60 70
Infant Mortality Rate Indonesia 1991- 2014 (per 1000 live birth)
Source : World Bank, Publication 2014
Today, Infant mortality rate in Indonesia is tends to diminish. IMR of Indonesia is 23 dead per 1000 in 2015, it is still high If we compare with another Asian countries like Malaysia (6/1000 dead), Thailand (11/1000 dead), and Vietnam (19/1000 dead)2. Various eforts it has made to reduce
maternal mortality, newborns, infants and toddlers. Among others through the placement of midwives in villages, empowering families and communities to use the Book Maternal and Child Health (MCH handbook) and Program Planning Labor and Prevention of Complications (P4K), and the provision of health facilities services Obstetric Neonatal Emergency Basis (PONED) at the health center care and Comprehensive Emergency Obstetric Neonatal care (PONEK) at the hospital, and also Immunization program for infant and toddler in Indonesia and improving sanitation facilities through Settlement Sanitation Development Acceleration (PPSP) Program . In other
side, the government efort to reduce infants and toddler mortality are improving education level for women, and increasing Government expenditure for Health3.
Literature Review
Many studied prove there are relationship between some government policies with infant mortality rate. Cheng. et all (2012) found that Access to improved water sources and sanitation reduces a nation’s infant mortality rate. One study found that the infant mortality rate decreases by 1.14 deaths per 1000 live births with increased access to an improved water source. The rate decreases by 1.66 with increased access to improved sanitation
Fink, Günther and Hill (2011) conducted one of the most comprehensive analyses onchild health, water, and sanitation. They merged all the DHS datasets available for seventy countries over the period 1986 to 2007. Even though the estimated efect of improved water and sanitation is smaller than estimations done by other studies, they still found a positive impact in the reduction of mortality, as well as a lower risk of diarrhea, and stunting. However, the authors also fnd that the positive results of clean water are more subtle and afect only children between 1 and 12 months4.
Bampoky (2013) found that there are efect of drinking water source and sanitation on child mortality in Senegal. Household who have water piped into the dwelling or a fush toilet increases the probability of child survival by 2.3 percentage points and 3.2 percentage points, respectively. The presence of soap or detergent in the dwelling also increases this probability by 2.5 percentage points.
Kapoor (2010) found that Female literacy has a negative and statistically signifcant on infant mortality. A 1% increase in female literacy is associated with a 23% drop in IMRs on average. These results further enforce the claims made in the existing literature, that there indeed is a strong association between female's education and infant mortality rates.
3
http://dinkes.cirebonkab.go.id/artikel/upaya-percepatan-penurunan-angka-kematian-ibu-dan-bayi-baru-lahir-di-indonesia.html
Data and Method
This study aims to analyze the efect of macroeconomic, demographic, and environmental policies on the health status of the infant in Indonesia using
Least-Square method. Infant mortality can be attributed to a range of hierarchical determinants that include health status, water and sanitation, and socio-economic status, education factors. The data and variable which used in this study consist of ;
(1)IMR (Infant Mortality Rate Data in Indonesia), is the number of infants dying before reaching one year of age, per 1,000 live births in a given year.
(2)ISF (Improved Sanitation Facilities), Access to improved sanitation facilities refers to the percentage of the population using improved sanitation facilities. Improved sanitation facilities are likely to ensure hygienic separation of human excreta from human contact. They include fush/pour fush (to piped sewer system, septic tank, pit latrine), ventilated improved pit (VIP) latrine, pit latrine with slab, and composting toilet.
(3)Imm (Measles Immunization), Child immunization measures the percentage of children ages 12-23 months who received vaccinations before 12 months or at any time before the survey. A child is considered adequately immunized against measles after receiving one dose of vaccine.
(4)Hex (Government Health Expenditure), Total health expenditure is the sum of public and private health expenditure. It covers the provision of health services (preventive and curative), family planning activities, nutrition activities, and emergency aid designated for health but does not include provision of water and sanitation.
(5)WE (Women Education) number of women who fnished the primary education in Indonesia.
Classical Assumption
5The estimators that we create through linear regression give us a relationship between the variables. However, performing a regression does not automatically give us a reliable relationship between the variables. In order to create reliable relationships, we must know the properties of the estimators and show that some basic assumptions about the data are true.one must understand that having a good dataset is of enormous importance for applied economic research.
Given the following two assumptions, OLS is
the Best Linear Unbiased Estimator (BLUE). This means that out of all possible linear unbiased estimators, OLS gives the most precise estimates of and .
With the third assumption, OLS is the Best Unbiased Estimator (BUE), so it even beats non-linear estimators. Also given this assumption, is distributed according to the Student's t-distribution about , and is distributed in such a way about .
No Heteroskedasticity
The variance of the Error terms are constant. . This means that the variance of the error term does not depend on the value of . If this is the case, the error terms are called homoskedastic. To determine the heteroskedasticity we used White Heteroskedasticity test (with hypothesis : H0= no heteroskedasticity, H1= there heteroskedasticity) by looking at the
Breusch-Godfrey Serial Correlation LM Test (with hypothesis : H0= no serial
correlation, H1= there correlation) by looking at the value of probability chi
square from Obs*R-Squared, if the p-value obs * R-Square > α 0.1, then Ho is accepted and means there is no correlation. But if p-value obs * R-Square < α 0.1 then Ho is rejected and means there is correlation
Normally Distributed Errors
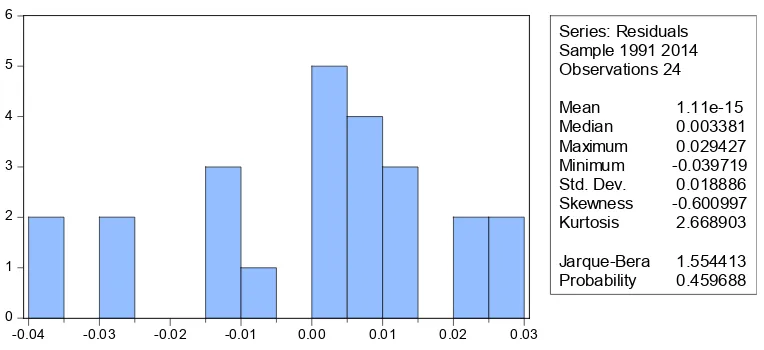
The error terms are normally distributed. . To determine the Normally Distributed Error we use Histogram Normality Test (with hypothesis : H0= no serial correlation, H1= there correlation) by looking at the value of
Jarque-Bera probability , if the Jarque-Bera probability > α 0.1, then Ho is accepted and means the error term are normally distributed. But if Jarque-Bera probability < α 0.1 then Ho is rejected and means the error term are normally distributed.
Models
To determine the contribution of the independent variables to the dependent variable, we use this following model :
IMR = a +β1ISF + β2Imm + β3Hex + β4WE
The model is transformed into logarithmic form become following model : LnIMR = a +β1 LnISF + β2 LnImm + β3 LnHex + β4 LnWE
Estimation Result
The result of least-square regression are presented in the equation below :
t-test (8.563510) 11.89712) 0.097982)
(-Based on the regression results in Table 4 it is known that the model used in this study is sufciently representative, it is proved by R-squared value of 0.99 This means that about 99% of the variations in Infant Mortality Rate in Indonesia could be attributed to the explanatory variables presented.
Then, from the equation we can found that all of independent variables have negative relationship with dependent variable. ISF (Improved Sanitation Facilities) has negative impact on Infant Mortality rate, where when percentage of the population using sanitation facilities increases 1% will reduces 1.347003% of infant mortality. t-statistic value of ISF is -11.89712, more than t-table (1,711). It means Improved Sanitation Facilities signifcantly reduce the Infant Mortality Rate in Indonesia.
IMM (Measles Immunization) has negative impact on Infant Mortality rate, where when the number of infant who get infant immunization increases 1% will reduces 0.008983% of infant mortality rate. tstatistic value of ISF is -0.097982, less than t-table (1,711). It means Measles Immunization is not signifcantly reduces the Infant Mortality Rate in Indonesia.
Then, Hex (Government Health Expenditure) has negative impact on Infant Mortality rate either, it 0.259110% reducing infant mortality. t-statistic value of Hex is -3.957844, more than t-table (1,711). It means Government Health Expenditure signifcantly reduces the Infant Mortality Rate in Indonesia.
Finally, WE (Women Education) has negative impact on Infant Mortality rate, where when the number of women who fnish their primary education reducing 0.884148% infant mortality. t-statistic value of WE is -4.652582, more than t-table (1,711). It means Women Education signifcantly reduces the Infant Mortality Rate in Indonesia.
The result of classical assumption test are shown in table below : Heteroskedasticity Test
Table 2
White Heteroskedasticity Test
Heteroskedasticity Test: White
F-statistic 0.681263 Prob. F(4,19) 0.6135 Obs*R-squared 3.010406 Prob. Chi-Square(4) 0.5561 Scaled explained SS 1.574384 Prob. Chi-Square(4) 0.8134
from the table 2 we can see that the Obs*R-Squared value is 3.010406 with probability value Chi-Square 0.5561. the value of Prob. Chi-Square more than α 0.1 , it is mean H0 is accepted and means there was no heteroskedasticity
Serial Correlation Test
Table 3
Breusch-Godfrey Serial Correlation LM Test
from the table 3 we can see that the Obs*R-Squared value is 0.788827 with probability value Chi-Square 0.6741. the value of Prob. Chi-Square more than α 0.1 , it is mean H0 is accepted and means there was no serial correlation
Breusch-Godfrey Serial Correlation LM Test:
Normality Test
-0.04 -0.03 -0.02 -0.01 0.00 0.01 0.02 0.03
Series: Residuals
from the table 2 we can see that the value of Jarque-Bera Probability is
0.459688 and more than α 0.1 , it is mean H0 is accepted and means the error
term are normally distributed.
Conclusion and Policies
This study aims to analyze the efect of macroeconomic, demographic, and environmental policies on the health status of the infant in Indonesia The results above have very useful implications for policy formulations reducing the infant mortality rate in Indonesia. The result shows that Improved Sanitation, Government Health Expenditure, and Women Education are signifcantly reduce the number of infant mortality rate in Indonesia. But government policy for Measles Immunization is not signifcantly reduces infant mortality rate. Indeed, it can be concluded that, socio-economic factors play an important role in reducing IMR in Indonesia.
Government Health Expenditure variable is signifcantly reduce the IMR in Indonesia, it implied that the expense that were incurred by the Government of Indonesia are efective reducing the IMR. From this result we suggest policies for boots government spending for health.
Measles Immunization is not signifcantly reduces infant mortality rate. From this result we suggest the government should promote the vaccine movement broadly.
References
Bampoky, Chaterine. (2013 ). Can clean drinking water and sanitation reducing infant mortality rate in Senegal. Pepperdine University, School of Public Policy.
Benova L, Cumming O, Gordon BA, Magoma M, Campbell OM. (2014). Where there is no toilet: water and sanitation .
Cheng JJ, Schuster-Wallace CJ, Watt S, Newbold BK, Mente A. (2012). An ecological quantifcation of the relationships between water, sanitation and infant, child, and maternal mortality. Environ Health; 11: 4.
Fink, G., Geunther, I., & Hill, K. (January 01, 2011). The efect of water and sanitation on child health: evidence from the demographic and health surveys 1986-2007. International Journal of Epidemiology, 40,
5, 1196-1204.
Kapoor, Shruti (2014). Infant Mortality Rates in India: District Level Variations and Correlations. UC Riverside.
World Bank Development Indicators (WBI). Mortality Rate, Infant (1000). http://data.worldbank.org/indicator/SP.DYN.IMRT.IN/countries
(accessed april, 10, 2015)