&KDQJHVLQ7XPRU1HFURVLV)DFWRU$OSKDDQG,QWHUOHXNLQ
/HYHOVLQ3DWLHQWVZLWK2EVWUXFWLYH-DXQGLFHGXHWR
3DQFUHDWRELOLDU\&DQFHU:KR8QGHUZHQW%LOLDU\'UDLQDJH
Adang Sabarudin*, Rino Alvani Gani**, Murdani Abdullah***,
C Martin Rumende****
* Department of Internal Medicine, Mitra Keluarga Bekasi Timur Hospital, Bekasi ** Division of Hepatobiliary, Department of Internal Medicine, Faculty of Medicine Universitas Indonesia/Dr. Cipto Mangunkusumo General National Hospital, Jakarta ***Division of Gastroenterology, Department of Internal Medicine, Faculty of Medicine
Universitas Indonesia/Dr. Cipto Mangunkusumo General National Hospital, Jakarta **** Division of Pulmonology, Department of Internal Medicine,Faculty of Medicine Universitas Indonesia/Dr. CiptoMangunkusumo General National Hospital, Jakarta
Corresponding author:
Rino Alvani Gani. Division of Hepatobiliary, Department of Internal Medicine, Dr. Cipto Mangunkusumo General National Hospital. Jl. Diponegoro No.71 Jakarta Indonesia. Phone: +62-21-31900924; Facsimile: +62-21-3918842. E-mail: [email protected]
$%675$&7
Background: Obstructive jaundice represents the most common complication of biliary tract malignancy.
2EVWUXFWLYHMDXQGLFHFDXVHVUHOHDVHVRISURLQÀDPPDWRU\F\WRNLQH7KHUHKDVEHHQFRQWURYHUV\DERXWHIIHFW RIELOLDU\GUDLQDJHRQWKHFKDQJHLQSURLQÀDPPDWRU\F\WRNLQHOHYHOLQSDQFUHDWRELOLDU\FDQFHUSDWLHQWV7KH
present study was designed to determine levels of tumor necrosis factor alpha (TNF-alpha) and interleukin 6 (IL-6) in preprocedure of either endoscopic retrograde cholangiopancreatography (ERCP) or percutaneous transhepatic biliary drainage (PTBD) and postprocedure of them in obstructive jaundice patient caused by pancreatobiliary cancer.
Method: The study method was before-and-after case study design with consecutive sampling. Blood was
FROOHFWHG¿YHGD\VSULRUWRHLWKHUHQGRVFRSLFUHWURJUDGHFKRODQJLRSDQFUHDWRJUDSK\(5&3SURFHGXUHRU SHUFXWDQHXVWUDQVKHSDWLFELOLDU\GUDLQDJH37%'SURFHGXUHDQG¿YHGD\VDIWHUHLWKHURIWKHP(Q]\PHOLQNHG
immunosorbed assay (ELISA) was used to determine TNF-alpha and IL-6.
Results:Forty subjects were included in this study which consisted of 22 men and 18 women. The age was 55.3 (SD 13.7) years old. According to the results of imaging and endoscopy procedure, twenty-two people were diagnosed cholangicarcinoma, ten people were diagnosed ampulla vateri and eigth people were diagnosed pancreatic tumor. In preprocedure, the TNF-alpha concentration was 4.81 (SD 2.91) pg/mL, the IL-6 concentration was 7.79 (SD 1.57) pg/mL and the bilirubin concentration was 15.5 (SD 6,9)mg%. In postprocedure, the
TNF-DOSKDFRQFHQWUDWLRQZDV6'SJP/WKHUHZDVDVLJQL¿FDQWLQFUHDVHLQ71)DOSKDFRQFHQWUDWLRQS +RZHYHU,/FRQFHQWUDWLRQZDV6'SJP/WKHUHZDVQRWDQ\VLJQL¿FDQWFKDQFHLQ,/
concentration (p = 0.52). The bilirubin concentration was 11.3 (SD 6,5) mg%.
Conclusion:7KHUHZDVDVLJQL¿FDQWLQFUHDVHLQPHDQFRQFHQWUDWLRQYDOXHRI71)DOSKDDIWHUELOLDU\GUDLQDJH
SURFHGXUH2QWKHRWKHUKDQGWKHUHZDVQRWDQ\VLJQL¿FDQWGHFUHDVHLQWKHPHDQFRQFHQWUDWLRQYDOXHRI,/
Keywords: obstructive jaundice, pancreaticobilliary cancer, tumor necrosis factor alpha (TNF-alpha), interleukin 6 (IL-6), endoscopic retrograde cholangiopancreatography (ERCP), percutaneus transhepatic biliary drainage (PTBD)
ABSTRAK
Latar belakang: Ikterus obstruktif merupakan salah satu komplikasi tersering keganasan sistem bilier.
.HDGDDQLQLDNDQPHPLFXSHOHSDVDQVLWRNLQSURLQÀDPDVL7HUGDSDWNRQWURYHUVLPHQJHQDLSHQJDUXKGUDLQDVH ELOLHUWHUKDGDSSHUXEDKDQNDGDUVLWRNLQSURLQÀDPDVLSDGDSHQGHULWDNDQNHUSDQNUHDWRELOLHU3HQHOLWLDQLQL
bertujuan untuk mengetahui kadar tumor necrosis faktor alfa (TNF-alfa) dan interleukin 6 (IL-6) sebelum dan sesudah endoscopic retrograde cholangiopancreatography (ERCP) atau percutaneus transhepatic biliary drainage (PTBD) pada penderita ikterus obstruksi etiologi kanker pankreatobilier.
Metode: Desain penelitian adalah penelitian satu kelompok sebelum dan setelah dengan pemilihan sampel secara konsekutif. Sampel darah diambil sebelum dan lima hari sesudah ERCP atau PTBD. Pengukuran kadar TNF-alfa dan IL-6 dengan cara enzyme linked immunosorbed assay (ELISA).
Hasil: Terdapat 40 orang responden yang diikutsertakan dalam penelitian ini, 22 laki laki dan 18 perempuan dengan usia rata rata 55,3 (SD 13.7) tahun. Berdasarkan imaging dan endoskopi, ditegakkan diagnosis kolangiokarsinoma sebanyak 22 orang, tumor ampulla vateri 10 orang, dan tumor pankreas 8 orang. Kadar rata-rata TNF- alfa sebelum tindakan 4,81 (SD 2,91) pg/mL dan sesudah tindakan 8,05 (SD 6,7) pg/mL, terdapat peningkatan yang bermakna setelah tindakan drainase bilier (p = 0,02). Kadar rata-rata IL-6 sebelum tindakan 7,79 (SD 1,57) pg/mL dan sesudah tindakan 7,75 (SD 1,76) pg/mL, tidak terdapat perbedaan yang bermakna setelah tindakan drainase bilier (p = 0.52). Kadar rata-rata bilirubin sebelum tindakan 15,5 (SD 6,9) mg% dan sesudah tindakan 11,3 (SD 6,5) mg%.
Simpulan:Terjadi peningkatan kadar rata-rata TNF-alfa secara bermakna setelah drainase. Tidak ada penurunan yang bermakna kadar rata-rata IL-6.
Kata kunci:ikterus obstruksi, kanker pankreatobilier, tumor necrosis factor alpha (TNF-alfa), interleukin 6 (IL-6), endoscopic retrograde cholangiopancreatography (ERCP), percutaneus transhepatic biliary drainage (PTBD)
,1752'8&7,21
(YHU\\HDULWLVSUHGLFWHGWKDWWKHUHDUH
of new pancreatobiliary cancer cases with mortality
UDWH RI One of the complications of SDQFUHDWRELOLDU\FDQFHULVREVWUXFWLYHMDXQGLFHZKLFK LV DQ REVWUXFWLRQ LQ WKH ELOLDU\ ÀRZ IURP OLYHU WR
duodenum..XUQLDZDQHWDOIRXQGWKDWFDXVHV of obstructive jaundice was malignancy in patients hospitalized in Cipto Mangunkusumo Hospital in
4 0HDQZKLOH6MDPVXKLGD\DWHWDOUHSRUWHG WKDW FDVHV RI H[WUDKHSDWLF WXPRXU FDXVLQJ
obstructive jaundice were malignancy and carcinoma of the head of pancreas which were the most common
FDXVH RI PDOLJQDQW REVWUXFWLYH MDXQGLFH !
Biliary tract obstruction causes decrease of bile level
LQGXRGHQXPDQGELOHDFFXPXODWLRQLQWKHELOLDU\WUDFW WKXVDOWHUDWLRQVLQLQWHVWLQDOQRUPDOÀRUDLQWHVWLQDO PXFRVDHSLWKHOLDOEDUULHULPSDLUPHQWDQGLQWHVWLQDO
bacteria translocation occur.Bile accumulation causes impairment of Kuppfer cells and hepatocytes which
VWLPXODWHWKHUHOHDVHRISURLQÀDPPDWRU\F\WRNLQHV
including interleukin 6 (IL-6) and tumour necrosis factoralpha (TNF-alpha).6
In patients suffering from obstructive jaundice
GXHWRXQUHVHFWDEOHSDQFUHDWRELOLDU\FDQFHUGUDLQDJH SURFHGXUHZDVDQRSWLRQDOSDOOLDWLYHWKHUDS\KRZHYHU
the survival rate of malignant obstructive jaundice
ZKRXQGHUZHQWELOLDU\GUDLQDJHZDVQRWVLJQL¿FDQW
Biliary drainage procedure will decrease bilirubin level in the blood and is expected to decrease hepatocytes
LPSDLUPHQW GHFUHDVH VWLPXOL WR LQÀDPPDWRU\ FHOOV DQG.XSSIHUFHOOVKHQFHWKHLQÀDPPDWLRQSURFHVV LVGHFUHDVHG+RZHYHUWKHGUDLQDJHSURFHGXUHDORQH
possesses the risk of trauma and infection after the procedure which can stimulate proinflammatory cytokines. TNF-alpha and IL-6 were the main
SURLQÀDPPDWRU\F\WRNLQHV7KHPDLQVRXUFHVRI71) DOSKDDQG,/DUHPDFURSKDJHVDQGPRUHWKDQ
and IL-6 levels.0HDQZKLOHVRPHRWKHUVVWDWHGWKDW biliary drainage did not decrease TNF-alpha and IL-6 levels.10
This study was aimed to understand the pathogenesis of inflammation which occur after biliary drainage in patients with obstructive jaundice due to pancreatobiliary cancer by measuring alteration in TNF-alpha and IL-6 levels before and after biliary
GUDLQDJH WKXV LW ZDV H[SHFWHG WR SURYLGH EHWWHU
understanding regarding this matter.
0(7+2'
This study was a prospective longitudinal
VWXG\RQHJURXSEHIRUHDIWHUVWXG\7KLVVWXG\ZDV
performed in Internal Medicine Inpatient Ward Cipto
0DQJXQNXVXPR+RVSLWDOLQ2FWREHUWR0DUFK 6DPSOHV ZHUH FROOHFWHG XVLQJ FRQVHFXWLYH
sampling method. Samples were patients suffering from obstructive jaundice due to pancreatobiliary cancer in Internal Medicine Inpatient Ward Cipto
0DQJXQNXVXPR +RVSLWDO GXULQJ 2FWREHU WR 0DUFK SHULRG ZKR IXOILOOHG VWXG\ FULWHULD
Inclusion criteria included patients aged > \HDUV old with diagnosis of obstructive jaundice due to pancreatobiliary cancer. Exclusion criteria in this study were patients who had undergone PTBD or ERCP
SUHYLRXVO\DQGSDWLHQWVZKRUHIXVHGWRSDUWLFLSDWHLQ
the study.
Independent variable in this study was biliary
GUDLQDJH(5&3RU37%'ZKLOHGHSHQGHQWYDULDEOH
in this study were TNF-alpha and IL-6 levels. Sample examination was performed in Hepatobiliary
/DERUDWRU\)DFXOW\RI0HGLFLQH8QLYHUVLWDV,QGRQHVLD
Cipto mangunkusumo Hospital. Reagent kit being used were Quantukune ELISA Human IL-6 and
+XPDQ71)DOSKDSURGXFWVIURP5 '6\VWHP,QF 0LQHDSROLV86$&ROOHFWHGGDWDZHUHSULPDU\GDWD ZKLFKLQFOXGHGDJHVH[DQWLELRWLFVXVHQRQVWHURLGDO DQWLLQÀDPPDWRU\ drugs (16$,'6 XVH FRPRUELG
VFRUH ELOLUXELQ OHYHO71)DOSKD OHYHOV DQG ,/
levels. Data processing and analysis was performed
XVLQJ6366VRIWZDUH7KLVVWXG\KDGUHFHLYHG
ethical approval from Faculty of Medicine Universitas Indonesia and had obtained ethical approval from Cipto Mangunkusumo Hospital Jakarta with letter number
/%;
5(68/76
Basic characteristics of 40 research participants
were presented in Table 1. This study included 40 obstructive jaundice patients due to pancreatobiliary
FDQFHUPDOHVIHPDOHVZLWKDYHUDJHDJHRI 6'\HDUVROG&KRODQJLRFDUFLQRPDZDVWKHPRVW FRPPRQDHWLRORJ\IRXQGLQLQGLYLGXDOVIROORZHG E\ DPSXOOD YDWHUL WXPRXU IRXQG LQ LQGLYLGXDOV DQGSDQFUHDWLFWXPRXUIRXQGLQLQGLYLGXDOV(5&3
Mean age (years old) Diagnosis
Cholangiocarcinoma Ampulla vateri tumour Pancreatic tumour
Figure 1 showed results of TNF-alpha levels before
DQGDIWHUELOLDU\GUDLQDJHQ
P=0.02 8.05 (6.7)
4.81 (2.91)
Before Drainage After Drainage Average Levels of TNF-Alpha (pg/mL)
)LJXUHU71)DOSKDOHYHOVEHIRUHDQGDIWHUGUDLQDJH
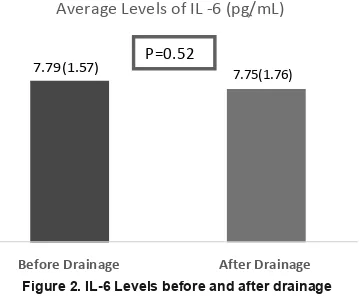
)LJXUHSUHVHQWHGWKHUHVXOWVRI,/OHYHOVEHIRUH DQGDIWHUELOLDU\GUDLQDJHSURFHGXUHQ
P=0.52
Average Levels of IL -6 (pg/mL)
7.79 (1.57) 7.75(1.76)
Before Drainage After Drainage
)LJXUH,//HYHOVEHIRUHDQGDIWHUGUDLQDJH
TNF-alpha levels before and after biliary drainage
YVSJP/6'ZKLOH,/OHYHOVEHIRUH DQGDIWHUWKHSURFHGXUHGLGQRWGLIIHUVLJQL¿FDQWO\ZLWK S SJP/6'YVSJP/6' 7DEOHVKRZHGUHVXOWVRIELOLUXELQOHYHODQG
leucocyte count before and after biliary drainage.
7DEOH5HVXOWVRIODERUDWRU\WHVWVQ
3DUDPHWHU %HIRUHSURFHGXUH $IWHUSURFHGXUH Bilirubin (mg%) 15.5 (SD 6.9) 11.3 (SD 6.5) Leucocyte count/mL 11.570 (SD 6100) 11.700 (SD 5800)
There was a decrease in the average of bilirubin
OHYHOV EHIRUH SURFHGXUH IURP 6' PJ WR 6' PJ DIWHU GUDLQDJH SURFHGXUH 0HDQZKLOHOHXFRF\WHFRXQWEHIRUHDQGDIWHUSURFHGXUH LQFUHDVHGVOLJKWO\P/6'YVP/ 6'
7DEOHSUHVHQWHGUHVXOWVRIV\VWHPLFLQÀDPPDWRU\ UHVSRQVHV\QGURPH6,56FRPRUELGVFRUHXVHRI
antibiotic and use of NSAIDs before and after ERCP or PTBD.
7DEOH(YDOXDWLRQRQWKHSUHVHQFHRI6,56FRPRUELGVFRUH DQWLELRWLFXVHDQG16$,'VXVH
3DUDPHWHU %HIRUHSURFHGXUH $IWHUSURFHGXUH
Presence of SIRS 13 (32.5%) 15 (37.5%)
Comorbid score 2 28 (70%) 28 (70%)
Comorbid score 3 12 (30%) 12 (30%)
Antibiotic use 40 (100%) 40 (100%)
NSAIDs use 40 (100%) 40 (100%)
6,56 V\VWHPLF LQÀDPPDWRU\ UHVSRQVH V\QGURPH 16$,'V QRQVWHURLGDO DQWLLQÀDPPDWRU\GUXJV
There was an increased number of SIRS patients as
PXFKDVSDWLHQWVDIWHUXQGHUJRLQJGUDLQDJHSURFHGXUH 7KHUHZDVQRFKDQJHLQFRPRUELGVFRUH16$,'VXVH
and antibiotic use before and after drainage.
7KHUH ZHUH SDWLHQWV VXIIHULQJ IURP SDQFUHDWLWLVKRXUVDIWHU(5&3SURFHGXUH3DQFUHDWLWLV
diagnosis was established based on increased results of
DP\ODVHDQGOLSDVHHQ]\PHH[DPLQDWLRQPRUHWKDQ[ RIXSSHUQRUPDOOLPLWV7KUHHGD\VDIWHUWKHSURFHGXUH WKHUHVXOWVRIWKRVHHQ]\PHVGHFUHDVHGWROHVVWKDQ[
upper normal limits.
There was an increased level of TNF-alpha before
DQGDIWHU(5&3SJP/YVSJP/ZKLOH DIWHU37%'ZDVVLPLODUSJP/YVSJP/
IL-6 levels before and after ERCP or PTBD did not
GLIIHUVLJQL¿FDQWO\
Highest TNF-alpha levels before drainage procedure
ZDV IRXQG LQ SDWLHQWV ZLWK DPSXOOD YDWHUL WXPRXU ZKLFKVKRZHGSJP/6'IROORZHGE\ FKRODQJLRFDUFLQRPDZLWKSJP/6'DQG SDQFUHDWLFWXPRXUZLWKSJP/6'$IWHU ELOLDU\ GUDLQDJH DOO LQFUHDVHG WR SJP/ 6' SJ/6'DQGSJP/6' UHVSHFWLYHO\0HDQZKLOH,/OHYHOVEHIRUHDQGDIWHU
procedure were similar in all types of tumour.
',6&866,21
Levels of TNF-alpha and IL-6 vary in healthy population. TNF-alpha and IL-6 levels are very
SRVVLEOH WR EH LQÀXHQFHG E\ HQYLURQPHQWDO IDFWRU SROOXWLRQ KDELWV VPRNLQJ DQG YLWDPLQ ' OHYHOV
in the blood.Experts agree that in the presence
RIELOLDU\REVWUXFWLRQWKHOHYHORISURLQÀDPPDWRU\ F\WRNLQHVZLOOLQFUHDVHLQFOXGLQJ71)DOSKDDQG,/ ,QWKLVVWXG\ZHIRXQGSDWLHQWVZLWKREVWUXFWLYH
jaundice with malignancy aetiology with the average
DJHRI6'\HDUVROGZLWKRIWKHP
were males. This result was similar to the previous
VWXG\ZLWKDYHUDJHDJHRI\HDUVROGDQGPDOHVZHUH 4 7KLV VKRZHG WKDW GXULQJ SHULRG
demographical data did not change considerably.
%HVLGHVZHREWDLQHGWKDWWKHPRVWFRPPRQFDXVH RI REVWUXFWLRQ ZDV SDQFUHDWLF WXPRXU IROORZHG E\ FKRODQJLRFDUFLQRPD DQG DPSXOOD YDWHUL WXPRXU
This difference was thought to be caused by different sampling method.
The role of NSAIDs and antibiotic in this study could not be evaluated because all patients received
16$,'V SDUDFHWDPRO DQG DQWLELRWLFV EHIRUH DQG DIWHU WKH SURFHGXUH ,Q WKLV VWXG\ ZH IRXQG DQ
7DEOH71)ĮDQG,/OHYHOVEHIRUHDQGDIWHUELOLDU\GUDLQDJHEDVHGRQW\SHRISURFHGXUH
7\SHRIELOLDU\ 71)ĮSJP/ ,/SJP/
SURFHGXUHQ %HIRUHELOLDU\GUDLQDJH $IWHUELOLDU\GUDLQDJH %HIRUHELOLDU\drainage $IWHUELOLDU\GUDLQDJH
PTBD (n= 6) 5.48 5.10 7.39 7.97
ERCP (n = 34) 4.87 8.93 8.49 8.02
37%'SHUFXWDQHXVWUDQVKHSDWLFELOLDU\GUDLQDJH(5&3HQGRVFRSLFUHWURJUDGHFKRODQJLRSDQFUHDWRJUDSK\71)ĮWXPRUQHFURVLVIDFWRU
alpha; IL-6:interleukin 6
7DEOH71)ĮDQG,/OHYHOVEHIRUHDQGDIWHUELOLDU\GUDLQDJHEDVHGRQW\SHVRIWXPRXU
Cholangiocarcinoma 22 (55) 4.80 7.64 7.86 7.71
Ampulla vateri tumour 10 (25) 6.13 12.41 7.86 7.71
Pancreatic tumour 8 (20) 3.28 5.11 7.56 7.59
increased average of TNF-alpha level accompanied
ZLWKWKHWHQGHQF\RILQFUHDVHGOHXFRF\WHVWKHUHIRUH
the presence of infection after drainage needs to
EH FRQVLGHUHG7KHUH ZHUH LQGLYLGXDOV VXIIHULQJ IURP6,56DIWHUSURFHGXUHRIWKHPVXIIHUHGIURP SDQFUHDWLWLVSRVW(5&3ZLWKLQFUHDVHGOHYHOVRI71)
alpha and IL-6. We did not observe the other patient for the cause of SIRS because this study was not designed for that purpose. Evaluation on the presence
RI6,56ZDVYHU\SRVVLEOHWREHLQÀXHQFHGE\WKH
administration of paracetamol and antibiotics. Biliary drainage procedure succeeds to decrease
ELOLUXELQOHYHOZLWKDYHUDJHRIPJ7KHUHLVQR VSHFL¿FFULWHULDUHJDUGLQJWKHVXFFHVVUDWHRIELOLDU\ GUDLQDJHEXW.XUQLDZDQHWDOLQWKHLUSUHOLPLQDU\VWXG\
stated that a biliary drainage is considered successful
LIWKHUHLVDGHFUHDVHGOHYHORIELOLUXELQPRUHWKDQ PJLQGD\V4XLet al in their analysis suggested that biliary drainage was said to be successful if after
GUDLQDJHZDVSHUIRUPHGELOLUXELQOHYHOGHFUHDVHGWR PRUHWKDQRUZLWKLPDJLQJHYDOXDWLRQWKHZLGWK
of biliary tract was back to the normal size.14 In this
study we did not evaluate the width of biliary tract. The success rate of biliary drainage in this study
DYHUDJHOHYHORIELOLUXELQGHFUHDVHGIURPPJ WR PJ ZDV QRW IROORZHG ZLWK VLJQLILFDQW GHFUHDVH RI ,/ 3DGLOOR HW DO REWDLQHG VLJQL¿FDQW
decrease of IL-6 in obstructive jaundice with benign or malignant aetiology who underwent ERCP. This difference is possibly caused by the bilirubin level
ZKLFK FRQWLQXHG WR VWD\ KLJK DIWHU GUDLQDJH LH PJLQWKLVVWXG\+LJKOHYHORIELOLUXELQZLOO
lead to hepatocyte impairment and will stimulate
.XSSIHUFHOOVWRUHOHDVHSURLQÀDPPDWRU\F\WRNLQHV 0HDQZKLOH*ZDQJGDHHWDOGLGQRWIRXQGVLJQL¿FDQW
changes of IL-6 in obstructive jaundice patients with cholangiocarcinoma aetiology (16 individuals) and
SDQFUHDWLF WXPRXU LQGLYLGXDOV ZKR XQGHUZHQW
ERCP or PTBD. This study also obtained no changes in IL-6 level and cholangiocarcinoma as the most common aetiology. This is in accordance with the theory that cholangiocarcinoma is closely related to
FKURQLFLQÀDPPDWLRQSURFHVVDQGPLFURHQYLURQPHQW. 2WKHUIDFWRUVZKLFKFDQEHFRQVLGHUHGWRLQÀXHQFH ,/OHYHODUHWLPHRIVDPSOHFROOHFWLRQDIWHUSURFHGXUH GUDLQDJHWHFKQLTXHGLIIHUHQWW\SHRIWXPRXU$VWXG\
conducted by Griseldis et alin rats which created full thicknessinjury of 6 mm showed increased levels of
,/DQG71)DOSKDIURPKRXUWRKRXUVDIWHU
injury.16)URPGD\RILQMXU\71)DOSKDVWDUWHGWR
decrease and reached the baseline level in day-14 when
complete healing was achieved. Gokhan et alin their study attained that IL-6 and TNF-alpha levels increased
VLJQL¿FDQWO\KRXUVDIWHU(5&3WKLVVXSSRUWHGWKDW SURLQÀDPPDWRU\F\WRNLQHVDIWHUELOLDU\GUDLQDJHZDV LQÀXHQFHGE\LQMXU\GXULQJSURFHGXUH
Qiu et alin their meta-analysis study concluded
WKDW WKH LQÀDPPDWLRQ FDVFDGH ZKLFK KDSSHQ DIWHU (5&3 SURFHGXUH KDG QRW EHHQ IXOO\ XQGHUVWRRG QRQHWKHOHVVWKHWHFKQLTXHRISURFHGXUHZDVEHOLHYHG WRKDYHJUHDWLQÀXHQFHSK\VLFDOWUDXPDFKHPLFDO WKHUPDO DQG GXUDWLRQ RI SURFHGXUH14 This study HQFRXQWHUHG GLI¿FXOW\ LQ XQLIRUPLQJ WKH SURFHGXUH
being performed.
,Q WKLV VWXG\ ZH DWWDLQHG FKRODQJLRFDUFLQRPD FDVHV &XUUHQWO\ LW LV WKRXJKW WKDWFKURQLFLQÀDPPDWLRQSURFHVVLQWKHELOLDU\WUDFW
plays role in the presence of cholangiocarcinoma.
3URORQJHGKLJKOHYHORISURLQÀDPPDWRU\F\WRNLQHV
will induce cell transformation and inhibit antitumour
UHFHSWRU)XUWKHUPRUHWXPRXUPLFURHQYLURQPHQWZLOO SURGXFHSURLQÀDPPDWRU\F\WRNLQHVLQFOXGLQJ71) DOSKDDQG,/LQDKLJKOHYHOWKXVFDXVLQJSURORQJHG LQÀDPPDWLRQSURFHVV
,QWKLVVWXG\ZHIRXQGVLJQL¿FDQWLQFUHDVHLQWKH
average of TNF-alpha level after biliary drainage. This
ZDVWKRXJKWWREHFDXVHGE\WUDXPDGXULQJSURFHGXUH LQIHFWLRQ XVH RI XURJUDSKLQ LQ (5&3 XVH RI 2$,16 DQG FRPSOLFDWLRQV DIWHU (5&3 (5&3 RU
PTBD procedure causes trauma in the tissue which will cause increased levels of TNF-alpha and IL-6. Grisledis et al concluded that TNF-alpha levels would increase 6 hours after tissue injury and would reach its
SHDNDWKRXUVZKLFKODWHUGHFUHDVHGJUDGXDOO\LQ GD\ 16 PTBD procedure in 6 patients did not show LQFUHDVHG OHYHOV RI71)DOSKD WKLV ZDV SRVVLEO\
due to the liver tissue had very good regeneration characteristic.0HDQZKLOH(5&3SURFHGXUHLQ
SDWLHQWVLQFUHDVHG71)DOSKDOHYHOWKLVZDVWKRXJKWWR
be caused by trauma which happened during ERCP due to sphingterotomy and electric cauterisation. Biliary
GUDLQDJHSURFHGXUHLVYHU\GLI¿FXOWWRVLPSOLI\EHFDXVH
of the size of injury due to sphingterotomy in PTBD and liver impairment due to needle insertion in PTBD
ZDVQRWHTXDOLQDOOSDWLHQWV7KLVPLJKWLQÀXHQFHWKH
TNF-alpha level.
71)DOSKDLVDSURLQÀDPPDWRU\F\WRNLQHZKLFK KDVPDLQUROHLQWKHUHVSRQVHRIDFXWHLQÀDPPDWLRQ
to gram negative bacteria. It is found that there are
FRXQWLQFUHDVHGQXPEHURISDWLHQWVVXIIHULQJIURP 6,56 LQGLYLGXDOV LQGLYLGXDOV VXIIHUHG IURP
pancreatitis accompanied with increased average
RI71)DOSKDOHYHOWKXVWKHSRVVLELOLW\RILQIHFWLRQ
needs to be considered. Abeed et al through an in vitro study found that lipopolysaccharide-stimulated monocyte cells from patients with obstructive jaundice with malignancy aetiology secrete lesser TNF-alpha
FRPSDUHGWRQRUPDOLQGLYLGXDOWKHUHIRUHLWFRXOGEH
concluded that they are more prone to be infected by bacteria.
,Q WKLV VWXG\ ZH XVHG XURJUDSKLQ GXULQJ
ERCP. Urographin is an ionized iodine contrast which has high osmolality and has cytotoxic effect upon mucous cells of the biliary tract. Michele and Quintavalle stated that iodine contrast medium may increase apoptosis of endothelial cells and kidney
WXEXODUFHOOVZKLFKPD\FDXVHDFXWHNLGQH\LQMXU\
therefore the possibility of apoptosis in endothelial cells of biliary tract and hepatocytes could be assumed.
Excessive apoptosis may stimulate the release of
SURLQÀDPPDWRU\F\WRNLQHV2WKHUIDFWRUZKLFKZDV
thought to play role in the increase of TNF-alpha was
16$,'VXVH,QWKLVVWXG\DOOSDWLHQWVEHIRUHDQGDIWHU
procedure received NSAIDs (ketorolac or ketoprofen). It was found that single dose administration of NSAIDs
FHOHFR[LEDQGNHWRURODFLQKHDOWK\LQGLYLGXDOVZLOO GHFUHDVHWKHOHYHORI3*(DQGLQFUHDVHWKHOHYHORI
TNF-alpha. TNF-alpha level will return to normal after
DGPLQLVWUDWLRQRI3J(LQWUDYHQRXVO\
,QWKLVVWXG\ZHIRXQGLQGLYLGXDOVVXIIHUHG
from pancreatitis which was manifested as complaint of stomachache and increased amylase serum to more
WKDQWLPHVRIXSSHUQRUPDOOLPLW(5&3SURFHGXUH PD\FDXVHORFDORHGHPDWKXVFDXVLQJREVWUXFWLRQWR WKHSDQFUHDWLFGXFWDQGOHDGWRSDQFUHDWLFHQ]\PHUHÀX[
Incidence of pancreatitis post ERCP in this study was similar to other studies.,QWKLVVWXG\ELOLDU\GUDLQDJH
SURFHGXUHLVEHQH¿FLDOWRLPSURYHOLYHUIXQFWLRQZKLFK LVVLJQL¿HGE\GHFUHDVHGDYHUDJHUDWHRIELOLUXELQDV PXFKDVPJ+RZHYHUZHVKRXOGUHPDLQFDXWLRXV
as this procedure causes increased level of TNF-alpha
ZKLFKLQGLFDWHGDSURJUHVVLQJLQÀDPPDWLRQ
6HOHFWLQJSDWLHQWEHIRUHELOLDU\GUDLQDJHSURFHGXUH WKHXVHRI16$,'VSDUDFHWDPRODQGDQWLELRWLFVEHIRUH DQG DIWHU ELOLDU\ GUDLQDJH SURFHGXUH ZLOO LQÀXHQFH
the evaluation on the presence or absence of SIRS.
'HWDLOVRISURFHGXUHDUHQRWSRVVLEOHWRJHQHUDOL]HG LQFOXGLQJWKHGXUDWLRQRISURFHGXUHWUDXPDXVHRI FRQWUDVWDOORIWKHVHIDFWRUVSRVVLEO\LQÀXHQFH,/
and TNF-alpha values.
&21&/86,21
,QWKLVVWXG\ZHIRXQGDVLJQL¿FDQWLQFUHDVHLQWKH DYHUDJHOHYHORI71)DOSKDDIWHUELOLDU\GUDLQDJHEXW WKHUHZDVQRVLJQL¿FDQWGHFUHDVHLQWKHDYHUDJHOHYHO
of IL-6 after biliary drainage procedure.
5()(5(1&(6
1. )HUOD\-6RHUMRPDWDUDP,'LNVKLW5(VHU60DWKHUV&
5HEHOR0&DQFHULQFLGHQFHDQGPRUWDOLW\ZRUOGZLGHVRXUFH
methods and mayor pattern in GLOBOCAN. Int J Cancer
RIWKHOLYHUDQGELOLDU\V\VWHPth ed. West Sussex: Blackwell 3XEOLVKLQJS
4. Kurniawan J. Kesintasan tiga bulan pasien ikterus obstruktif dengan etiologi maligna dan faktor-faktor yang
PHPSHQJDUXKLQ\D>7HVLV@-DNDUWD).8,3URJUDP3HQGLGLNDQ
Dokter Spesialis II Program Studi Ilmu Penyakit Dalam:
8QLYHUVLWDV,QGRQHVLD
6MDPVXKLGD\DW 5 /DOLVDQJ 7-0 6LUHJDU 1& 7DKHU$
Inhibition of bile acid accumulation decreased the excessive hepatocyte apoptosis and improved the liver secretion functions
RQREVWUXFWLYHMDXQGLFHSDWLHQWV0DNDUD
6. /MXQJGDKO02VWHUEHUJ-5DQVM|8(QJVWUDQG/+DJOXQG8
,QÀDPPDWRU\UHVSRQVHLQSDWLHQWVZLWKPDOLJQDQWREVWUXFWLYH MDXQGLFH6FDQG-*DVWURHQWHURO
=DQJ*</L:7'HQJ:-/L*'&OLQLFDORXWFRPHVDQG
prediction of survival following percutaneus biliary drainage for malignant obstructive jaundice. Oncology Letters
%DUDWDZLMD\D.*6LWRNLQ,Q%DUDWDZLMD\D.*5HQJJDQLV ,HGV,PXQRORJLGDVDUnd ed. Jakarta: Balai Penerbit FKUI S
3DGLOOR )- 0XQWDQH - 0RQWHUR -/ %ULFHQR - 0LQR * 6RODU]DQR * HW DO (IIHFW RI LQWHUQDO ELOLDU\ GUDLQDJH RQ SODVPD OHYHOV RI HQGRWR[LQ F\WRNLQHV DQG &UHDFWLYH
protein in patients with obstructive jaundice. Word J Surg
10. <LOPD] % 3DULOGDU = %R]ND\D + %DUXWFXRJOX % &LQDU
&%DVRO*HWDO3URJQRVWLFXWLOLW\RIVHUXPQHRSWHULQLQ
obstructive jaundice secondary to malignant lesions treated by percutaneous transhepatic biliary drainage. J Vasc Interv
5DGLRO
11. *LXOLR.$QQDOLVD09DOHQWLQR=&\WRNLQHOHYHOLQWKH serums of healthy subjects [serial online] Mediator of
LQÀDPPDWLRQ>FLWHG)HEUXDU\@$YDLODEOHIURP85/
of endotoxin and cytokine of obstructive jaundice before and
DIWHUELOLDU\GUDLQDJH.RUHDQ-*DVWURHQWHURO
14. 4LX<'%DL-/;X)*'LQJ<7(IIHFWRISUHRSHUDWLYH biliary drainage on malignant obstructive jaundice: a
*ODXEHQ / )DXQWH 07KXZDILW 3 &KURQLF LQIODPDWRU\
and cytokine in the tumor microenuviroment. J Immunol
16. *ULVHOGLV + %UDXFOH 0 6PROD +:DUQHU 6 'LIIHUHQWLDO
UHJXODWLRQRISURLQÀDPDWRU\F\WRNLQHGXULQJZRXQGKHDOLQJ LQQRUPDODQGJOXFRFRUWLFRLGWUHDWHPLFH&\WRNLQH
*RNKDQ$.KHPLN$$GDV0.RF%*XUEX](.DUDKDQ 60HWDEROLFDQGLQÀDPDWRU\UHVSRQVHVDIWHU(5&3,QW-%LRPRO6FL
Nicholai M Szary. Complication of endoscopy retrograde cholangiopankreotography: How to avoid and manage them.
*DVWURHQWURODQG+HSDWRO
$EXG+&DPXUD03DQDUXV/=DLWRQ$,PPXQHG\VIXQFWLRQ
in patient with obstructive jaundice before and after endoscopic Retrograd cholangiopancreatography. British J
6XUJ
0LFKHOH$)DJD70LFKDHO$&\WRWR[LFHIIHFWVRIFRQWUDVW
media on renal tubular cell. Pathogenesis of contrast-induced acute kidney injury and prevention. J Bioche Molec Biol Res
4XLQWDYDOOH&%UHQFD00LFFR)')LRUH',QYLYRDQG
invitro assessment of pathway involved in contrast