Biodegradation Mechanisms of Restorative Dental
Resin Composites
H.D.K. Yulianto
Department of Biomedical Science and Technology Faculty of Den stry, Universitas Gadjah Mada Yogyakarta-Indonesia
Correspondence: H.D.K. Yulianto, c/o: Bagian Biomedik, Fakultas Kedokteran Gigi Universitas Gadjah Mada. Jl. Denta I, Sekip Utara Yogyakarta 55281, Indonesia. E-mail: [email protected]
ABSTRACT
Bacground: Sometime diffi cult question related with the survival time of dental resin composite restoration arises from our patient aft er their teeth has been restored with dental resin composites. Of course, precise time of the dental resin composite restoration maintained in their original shape cannot exactly be estimated. Although there are a number of diff erent reasons as to why we cannot precisely estimate the survival time of dental resin composite restoration, the summarizing answer is brief: “The biodegradation process of dental resin composite is complex and includes several various factors.” Purpose: to review the relationship of mechanical, physical and mechanical factors in the role of the biodegradation of restorative dental resin composites. Literature review: Combinations of mechanical, chemical, and biological factors in oral environment have been identifi ed as the important factors associated with decreasing surface properties and lost of their original shape. Initially during the biodegradation process of dental resin composite, small fraction of material component are detached from the surface, leaving various rough in the surface of the restoration. Surface roughness above the critical threshold value leads the adhesion of bacterial and biofi lm formation on the dental resin composite surface. Once again, the question associated with the precise mechanism of bacterial adhesion and biofi lm formations on the dental resin composite surface have not yet been identifi ed. Since the knowledge currently available about the biodegradation mechanism of dental resin composite still limited, more research is needed in this fi eld. Conclusion: Oral environmental changes within a restorative dental resin composites may aff ect the longevity of the composite restoration. The combination of mechanical and chemical factors is an important key to the role of the biodegradation material in oral environment.
Keywords: Dental resin composite; biodegradation; surface properties; oral environment
ABSTRAK
Latar belakang: Beberapa pasien sering menanyakan “berapa lama restorasi resin komposit tetap bertahan dan tidak terlepas ?”. Pertanyaan ini tidak bisa dij awab secara akurat dalam satuan waktu karena proses biodegradasi restorasi resin komposit dalam rongga mulut sangat komplek dan melibatkan interaksi dari banyak faktor. Tujuan: Studi pustaka ini bertujuan untuk mempelajari hubungan antara faktor mekanis, fi sik, dan kimiawi terhadap proses biodegradasi tumpatan resin komposit di dalam rongga mulut.
tentang mekanisme biodegradasi restorasi resin komposit masih terbatas, sehingga penelitian lebih lanjut diperlukan di bidang ini.
Simpulan: Perubahan lingkungan rongga mulut terhadap restorasi resin komposit diprediksi mempunyai pengaruh yang signifi kan terhadap “keawetan” restorasi resin komposit. Kombinasi antara faktor mekanik, fi sik dan kimia merupakan kunci penting yang berperan terhadap proses biodegradasi restorasi resin komposit di rongga mulut.
Kata kunci: Material restorasi resin komposit; biodegradasi; sifat dan karakter permukaan; lingkungan rongga mulut
INTRODUCTION
Dental caries is a major cause of tooth decay for most of Indonesian population. The main cause of dental caries is the att achment of bacteria that form biofi lms on the surface layers of hard and
soft tissues oral cavity.1 Currently, composite resin is still the main option for restoring dental hard tissue damage due to the process of caries. It is not only brought a change in materials and techniques but also a change in treatment philosophy2 called minimal invasive dentistry.3,4 Composites allow the possibility of preserving sound tooth structure during cavity preparation.5 Composites resins have the ability to bind to the dental hard tissues through the adhesive material.6 Furthermore, composite resin represents a signifi cant aesthetic treatment
option, enabling the fabrication of restorations with a natural appearance.7
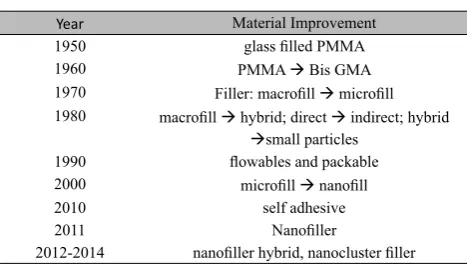
Table 1. Summary of the improvement of dental resin composite for which diff erent material proper es has been found14
Year Material Improvement
1950 glass fi lled PMMA
1960 PMMA Æ Bis GMA
1970 Filler: macrofi ll Æ microfi ll 1980 macrofi ll Æ hybrid; direct Æ indirect; hybrid
Æsmall particles 1990 fl owables and packable 2000 microfi ll Æ nanofi ll
2010 self adhesive
2011 Nanofi ller
2012-2014 nanofi ller hybrid, nanocluster fi ller
Table 1 summarizes the improvement of physical and mechanical properties of dental resin composite. As can be seen, although marked improvements have been noted in terms of physical and mechanical properties during the last 10-20 years, several factors in dynamic oral environment can degrade the composite matrix via three principal modes,8 i.e.: mechanical degradation,9 physical degradation and chemical degradation.10,11 Dynamic changes of oral environment are infl uenced by food components,
beverages, temperature changes, chewing, saliva and bacterial activity. Those factors have important role in the degradation of composite10,19 that clinically resulted various phenomena of failure, such as: discoloration, wear, ditching at the margins, delamination or simply fracture which may result in secondary dental caries.12,13
Ini
Ɵ
al biologic responses to resin composite
surfaces
The dental enamel and resin composite surface is a part that is always in contact with internal environment of oral cavity. Saliva, biofilm, and mastication force are identified as important contributing factors on dental resin composite biodegradation process.Resin composite surface is always encircled with saliva and form a thin layer of salivary pellicle, in which will promote adherence of oral bacteria. Adhesion of oral bacteria to salivary pellicle-coated tooth surface is critical step for oral bacteria colonization to form biofi lm.15,20-22
Biofilm adsorption depends on biologic flow rate at the site of contact, the type of interfacial interaction involved, and attachment strength with the substrate.23Adhesion and maturation of numerous species of cariogenic bacteria will promote maturation of biofi lm. These biofi lm will
easily trapped on the groove of rough surface that is resulted from degradation process by salivary enzyme like cholinesterase (CE),17 thereby promoting maturation. The att achment of bacteria on the teeth/ resin composite/ other restorative materials depend on surface roughness and surface free energy. In vivo studies showed that in supragingival regions, roughness contribute more to plaque formation than does the surface free energy.24 The possible explanation are: (1) microbial binding strength is lower on low-energy surfaces. (2) High surface-free energy microorganism binds with high-energy surfaces and vice versa. (3) The surface free energy regulates the adhesive strength of pellicle against the shear detachment forces. (4) The increased surface area and decreased protruding height of well-spread cells may produce a geometric confi guration with
Prolonged biologic responses
Mastication forces during mastication process will result various degree of surface roughness on the dental resin composite surface. Surface roughness and porosity are important factors to be determined when the material is subject to the oral biological environment. At high fl ow rate, surface
roughness and porosity produce local fl uid motions
of enhanced or reduced shear and will aff ect the shape, distribution, and aggregation of the att aching particles. At low fl ow rate or under static conditions,
the grooves of rough surface may act as stagnation points, therefore promoting biofi lm maturation.27
The role of surface roughness in biofi lm formation
has been widely investigated. Smooth polished surface of restoration have been shown to att ract less biofi lm in vivo compared to rough surface.24 Hydrophobic surface located supraginggivaly att ract less biofi lm in vivo than more hydrophilic
surfaces over a 9-day period. Increasing both surface energy and surface roughness above the threshold value were found to result more biofi lm
accumulation on dental resin composite surfaces. The progression of a rough dental resin composite caused by mechanically wear process (adhesion, abrasion, fatigue, corrosion) has also been associated with biofi lm formation.18
Bioadhesive activity of biofilm in biological environment depends on composition of outer monolayer and surface reactivity of outer monolayer. It can be explained that the material with high bioadhesive will increase surface tension and vice versa.28 High adhesion capability is one of the factors that determine the virulence of bacteria.29
Interaction between mastication force–saliva– biofilm is illustrated as chain “positive feedback loop”, which can be explained if there is one factor diminished, the chain will be broken.
Effect of surface properties on biofilm
forma
Ɵ
on
Initial bacterial adhesion is the fi rst step in the
plaque formation and is facilitated by electrostatic i n t e r a c t i o n s , h y d r o d y n a m i c i n t e r a c t i o n s , thermodynamic binding parameters, specifi c binding
mechanism, and cementation by polysaccharide matrices or glucans. Extracellular polysaccharide or glucan is produced by bacteria and will provide barrier protection for trapped organic acid. Organic acid that is trapped within glucan barrier, resulting prolonged low pH around resin composite and tooth surfaces.29,30,31
The att ached biofi lm on resin composite and tooth
surface can be classifi ed as “retained biofi lm” and
“detached biofi lm”. Biofi lm att achment is predicted
not only by single factor but might be come from several factors that will contribute together, like fi ller
size, type of matrix monomer, surface roughness, and amount of unpolymerized monomers. The fi ller
size and type of matrix monomer are depending on the type of resin composite material.31
The component of saliva that plays an important role in att achment of bacteria and biodegradation process are: albumin,29 salivary esterase, sucrose (glucan)-independent, aglutinins, proline-rich proteins, and mucins. Albumin plays a role in the adsorption and accumulation of bacteria on hard surfaces. Albumin is an inhibitor of hydrophobic interactions and will aff ect bacterial adhesion mediated by hydrophobic interactions.32-34 Cholesterol esterase (CE) and pseudocholinesterase (PCE) can hydrolyze bis-GMA and TEGDMA matrix synthetics monomer.35 Previous study showed that the amount and the patt ern of protein adsorbtion onto the material surface is specifi c to the type of
material,29 As the composition of composite may diff er among brands, the salivary adsorption of composite may result diff erent amount and patt ern. Once in contact with resin composite surface, saliva is able to form adsorbed layers that are termed as conditioning fi lm. Development of conditioning
surface is considered as an initial stage in the process of biofi lm formation.
DISCUSSION
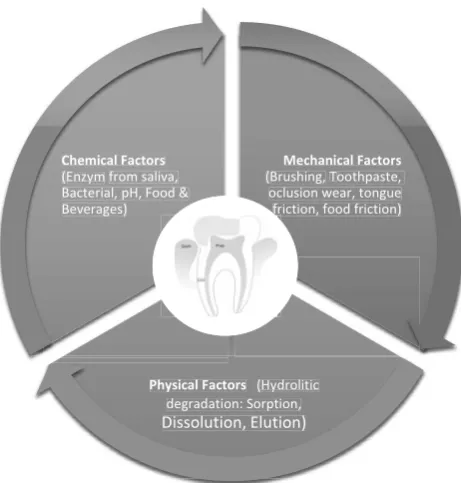
Aging of composite resins in the oral cavity is very complex as depicted in Figure 1. Thermal changes, food, beverages, saliva, temperature will degrade composite restoration.
Numerous different in vitro models were developed to evaluate the effect of the oral environment on dental resin composite and each model proposed to simulate different factors. However, In vitro aging models for composites study only single factors thus lacking the synergy of factors operative in the oral cavity. Some studies has been widely demonstrated the bacterial att achment on the dental resin composite surfaces, however the molecular and physical interactions that govern bacterial adhesion to dental resin composite have not been understood in detail. Conditioning fi lm is likely
Microorganisms in the oral environment not only form a biofi lm on all available surfaces, including
hard and soft tissue surfaces, but also on the surface of materials used for restoration of function or aesthetics.42 Exposure to saliva and biofi lm43 lead
to degradation of composite surfaces that may have increased roughness, sometimes accompanied by decreased microhardness and increased exposure of fi ller particles or matrix swelling.44,45 The amount
of unpolymerized monomer released is caused by hydrolase activity cholin esterase-like of saliva. The leaching of unpolymerized monomer in specifi c
amount is the marker that indicates the composite biodegradation process.36
Previous study showed that exposure to biofi lm
is the best choice for in vitro aging of dental resin composite surfaces.16 To refl ect what actually occurs
in the oral environment, in situ studies that is used as a golden standard also has been done.16 However, both of exposure to biofi lm and in situ study still
has limitations. The biofi lm study did not evaluate
the role of each bacteria involved and the patt ern of biofi lm adsorption that may infl uence the aging of
composite in these study. In the in situ study, the authors did not evaluate the eff ect of saliva protein and enzyme and the effect of teeth/restoration cleaning on the aging of composite. Based on the limitation of biofi lm and in situ study, both of those
studies is potential to be extended in the future research.
Several strategies have been done to reduce or avoid formation of biofi lm on the dental resin
composite surface by introducing antibacterial agents into dental composite.37 i.e.: silver and titanium,38 quaternary ammonium polyethylenimine nanoparticles,39 alkylated ammonium chloride derivatives,40 chlorhexidine diacetate.41 Although several antibacterial agents are proved to have an antimicrobial effect, there are still problems introducing these antimicrobial agents into composites, such as the problem associated with reducing mechanical properties, polymer leakage, decrease of antimicrobial properties with time and reduced ability of the composite to light cure.
Considering the fact that biodegradation of dental resin composites as a result of aging challenges their integrity and longevity over time the properties of composite still need to be improved. The information derived from role of biodegradation dental resin composite under in situ and in vitro aging model and the eff ect of antibacterial agent will give scientifi c contribution on the development of
antibacterial material to achieve clinically eff ective materials and to develop an agent that in the future can be minimized the att achment of bacterial on dental resin composite restoration.
REFERENCES
1. Khalichi P, Cvitkovitcha DG, Santerre JP. Effect of composite resin biodegradation products on oral streptococcal growth. Biomaterials 2004; 25: 5467–72. 2. Roeters FJM, Opdam NJM, Loomans BAC. The
amalgam-free dental school. J Dent 2004; 32: 371-7.
3. Murdoch-Kinch MA, McLean ME. Minimally invasive dentistry. J Am Dent Assoc 2003; 134: 87-95.
4. Tyas MJ, Anusavice KJ, Frencken JE, Mount GJ. Minimal intervention dentistry - a review - FDI Commission Project 1-97. Int Dent J 2000; 50:1-12.
5. Leinfelder K. A conservative approach to placing posterior composite resin restorations. J Am Dent Assoc 1997; 127:743-8.
6. Imazato S. Antibacterial properties of resin composites and dentin bonding systems. Dental Materials 2003; 19: 449–57.
7. Gordan V, Mjør I, Blum I, Wilson N. Teaching students the repair of resin-based composite restorations: a survey of North American dental schools. J Am Dent Assoc 2003; 134: 317-23.
8. Ferracane JL. Elution of leachable components from composite. J Oral Rehabil 1994; 21: 441-52.
Mechanical Factors
(Brushing, Toothpaste, oclusion wear, tongue
friction, food friction)
Physical Factors (Hydrolitic degradation: Sorption,
Dissolution, Elution)
Chemical Factors
(Enzym from saliva, Bacterial, pH, Food & Beverages)
9. Mair L, Stolarski T, Vowlest R, Lloyd C. Wear: mechanisms, manifestations and measurement. Report of a workshop. J Dent 1996; 24: 141-8.
10. Oilo G. Biodegradation of dental composites/glass-ionomer cements. Adv Dent Res 1992; 6: 50-4.
11. Winkler M, Greener E, Lautenschlager E. No-linear in vitro wear of posterior composites with time. Dent Mater 1991; 7: 258-62.
12. Roulet JF. The problems associated with substituting composite resins for amalgam: a status report on posterior composites. J Dent 1988; 16: 101-13.
13. Swift EJ. Wear of composite resins in permanent posterior teeth. J Am Dent Assoc 1987; 115: 584-8.
14. Ferracane JL. Resin composite-state of the art.Dental
Materials 2011; 27: 29-38.
15. Beytha N, Bahira R, Matalona S, Dombb AJ, Weiss EI. Streptococcus mutans biofilm changes surface-topography of resin composites. Dent 2008; 24: 732–6. 16. Rinastiti M. The eff ect of aging on composite-to-composite
repair strength. Thesis. Universiteit Groningen, Netherland, 2009.
17. Finer Y, Santerre JP. Salivary esterase activity and its association with the biodegradation of dental composite. J Dent Res 2004; 83(1): 22-6.
18. Sakaguchi RL, Power JM. Craig’s restorative dental materials. 13th Ed. St. Louis: Mosby Inc; 2012,
19. Akova T, Ozkomur A, Uysal H. Eff ect of food-simulating
liquids on the mechanical properties of provisional restorative materials. J Dent 2004; 22: 1130-4.
20. Eick S, Glockmann E, Brandl B, Pfi ster W. Adherence of
Streptococcus mutans to various restorative materials
in a continuous fl ow system. J Oral Rehabil 2004; 31:
278–85.
21. Eliades G, Eliades T, Brantley WA, Watt s DC. Dental
material in vivo: aging and related phenomena. Carol Stream Illinois, Quintessence Publishing Co, Inc; 2004. 61-99
22. Filoche SK, Zhu M, Wu CD. In situ Biofi lm formation by
multi-species oral bacteria under fl owing and anaerobic
conditions. J Dent Res 2009; 83: 802.
23. Hoff man A. Modifi cation of material surfaces to aff ect
how they interact with blood. Ann N Y Acad Sci 1987; 516: 96-101.
24. Quirynen M, Marechal M, Busscher HJ, Weerkamp AH,
Darius PL, Van Steenberghe D. The infl uence of surface
free energy and surface roughness on early plaque formation. J Clin Periodontol 1990; 17: 138-44.
25. Quirynen M, Marecal M, Busscher HJ. The infl uence of
surface free-energy on planimetric plaque growth in man. J Dent Res 1989; 68: 796-9.
26. Weerkamp AH, Quirynen M, Marechal M, van der Mei HC, Van Steenberghe D, Busscher, HJ. The role of surface energy in the early in vivo formation of dental plaque on human enamel and polymeric substrata. Microb Ecol Health Disease 1989; 2: 11-8.
27. Eliades G, Eliades T, Vavuranakis M. General aspect of biomaterial surface alterations following exposure to biologic fl uids. In: Eliades G, editor. Dental material
in vivo: aging and related phenomena. Carol Stream Illinois, Quintessence Publishing Co, Inc; 2003. p. 3-20.
28. Baier RE, Mayer AE, Natiella JR, Natiella PR, Carter JM. Surface properties determine bioadhesive outcomes: methods and results. J Biomed Mater Res 1984; 18: 337-55.
29. Steinberg D, Eyal S. Early formation of Streptococcus sobrinus biofi lm on various dental restorative materials.
Journal of Dentistry 2002; 30: 47-51.
30. Schilling KM, Bowen WH. Glucans synthesized in situ
in experimental salivary pellicle function as specifi c
binding sites for Streptococcus mutans. Infect Immun 1992; 60: 284 -95.
31. Ikeda M, Matin K, Nikaido T, Foxton RM, Tagami J. Eff ect of surface characteristics on adherence of S. mutans biofi lms to indirect resin composites. Dent Mater J 2007;
26(6): 915-23.
32. Satou J, Fukunaga A, Morikawa A, Matsumae I, Satou N, Shintani H. Streptococcal adherence to uncoated and saliva-coated restoratives. J Oral Rehabil 1991; 18: 421-9.
33. Gibbons RJ, Etherden I. Albumin as a blocking agent in studies of streptococcal adsorption to experimental salivary pellicles. Infect Immun 1985; 50: 592-4.
34. Rosenberg M, Buivids IA, Ellen RP. Adhesion of Actinomyces viscosus to porphyromonas (bacteriodes) gingivalis-coated hexadecane droplets. Bacteriology 1991; 173: 2581-9.
35. Finer Y, Santerre JP. Salivary esterase activity and its association with the biodegradation of dental composite. J Dent Res 2004; 83(1): 22-6.
36. Khalichi P, Cvitkovitch DG, Santerre JP. Effect of composite resin biodegradation products on oral streptococcal growth. Biomaterials 2004; 25: 5467-72. 37. Jandt KD, Sigusch BW. Future perspective of resin-based
materials. Dental Material 20092; 5: 1001-6.
38. Jandt KD, Al-Jasser AMO, Al-Ateeq K, Vowles RW, Allen GC. Mechanical properties and radiopacity of experimental glass-silica–metal hybrid composites. Dent Mater 2002; 6: 429–35.
39. Beyth N, Yudovin-Farber I, Bahir R, Domb AJ, Weissa E. Antibacterial activity of dental composites containing quaternary ammonium polyethylenimine nanoparticles against Streptococcus mutans. Biomaterials 2006; 21: 3995–4002.
40. Kim O, Shim WJ. Studies on the preparation and dental properties of antibacterial polymeric dental restorative composites containing alkylated ammonium chloride derivatives. J Polym Res Taiwan 2001; 1: 49–57.
41. Leung D, Spratt DA, Pratt en J, Gulabivala K, Mordan NJ, Young AM. Chlorhexidine-releasing methacrylate dental composite materials. Biomaterials 2005; 34: 7145–53. 42. Bouschlicher MR, Reindhardt JW, Vargas MA. Surface
treatment techniques for resin composite repair. Am J Dent 1997; 10: 279-83.
43. Fúcio Z, Carvalho FG, Sobrinho LC, Sinhoreti M,
Puppin-Rontani RM. The infl uence of 30-day-old Streptococcus
mutans biofi lm on the surface of esthetic restorative
materials--An in vitro study. J Dent 2008; 36: 833-9. 44. Göpferich A. Mechanisms of polymer degradation and
erosion. Biomaterials 1996; 17: 103-14.
45. Soderholm KJ. Degradation of glass fi ller in experimental