Review
Imaging
in
tuberculosis
Evangelia
Skoura
a,
Alimuddin
Zumla
b,
Jamshed
Bomanji
a,*
aInstituteofNuclearMedicine,UniversityCollegeHospitalsNHSTrust,LondonNW12BU,UKbDivisionofInfectionandImmunity,CentreforClinicalMicrobiology,UniversityCollegeLondon,andNIHRBiomedicalResearchCentre, UniversityCollegeLondonHospitals,London,UK
1. Introduction
Tuberculosis(TB)remainsaglobalemergencydespite substan-tial investment in health services over the past two decades. Patients withsputum-negative pulmonary TB (PTB) and extra-pulmonaryTB(EPTB)aredifficulttodiagnoseandmaybemissed atall pointsof care.Diagnostic imaging is challenging because signsofTBmaymimicthoseofotherdiseasessuchasneoplasmsor sarcoidosis.Clinicalsignsandsymptomsinaffectedadultscanbe non-specificandahighlevelofpre-testclinicalsuspicionbasedon history is fundamental in the diagnostic work-up. The global impactofTBisextremelyimportant,consideringthatanestimated 9.0millionpeopledevelopedTBin2013and1.5milliondiedfrom thedisease, accordingtotherecentWorld HealthOrganization (WHO)globaltuberculosisreport2014.
Early diagnosispromoteseffective treatment and leads toa reducedonwardtransmissionofTB.Thisarticlegivesareviewof imagingpatternsofchestTBasmaybedetectedonconventional radiographyandcomputedtomography(CT).Themainaimisto
improvetheradiologist’sfamiliaritywiththespectrumofimaging features of this disease in order to facilitate timely diagnosis. Furthermore, we consider the emerging role of alternative methodsofimaging,suchasmagneticresonanceimaging(MRI), whichcanbehelpfulandhighlyaccurateforabetterdefinitionof someofthesignsofTB.
Althoughnewimagingmethodsarenowbeingused, conven-tionalradiographyremainstheinitialmodalityforsuspectedPTBand formassscreeningpurposes.1CTandMRIarethemodalitiesofchoice for the evaluation of specific body parts.1 Positron emission tomography/computedtomographywiththeuseof18 F-fluorodeox-yglucose(18F-FDGPET/CT)isanon-invasiveimagingmethodthat has been used widely for the differentiation of malignant from benignlesions.However,18F-FDGalsoaccumulatesininflammatory cellssuchasneutrophils,activatedmacrophages,andlymphocytesat thesiteofinflammationorinfection.2Consequently,18F-FDGuptake isobservedinPTB,intuberculoma,andinotherTB-relatedlesions.3,4 UsingPET/CT,pulmonaryandextrapulmonaryTBinvolvementis assessedsimultaneously,withtime-andcost-savingimplications.
Although any organ of the body can be involved, the lung remainsthemostcommonlyinvolved organinTB. Theimaging appearancesofTB aredescribedbelowforboth pulmonaryand extrapulmonaryinvolvement.
ARTICLE INFO
Articlehistory:
Received14November2014
Receivedinrevisedform28November2014 Accepted1December2014
CorrespondingEditor:EskildPetersen, Aarhus,Denmark
Keywords:
Pulmonarytuberculosis Extrapulmonarytuberculosis Computedtomography Positronemissiontomography Fluorodeoxyglucose Magneticresonanceimaging
SUMMARY
Earlydiagnosisoftuberculosis(TB)isnecessaryforeffectivetreatment.InprimarypulmonaryTB,chest radiography remains the mainstay for the diagnosis of parenchymal disease, while computed tomography(CT)ismoresensitiveindetectinglymphadenopathy.Inpost-primarypulmonaryTB,CT isthemethodofchoicetorevealearlybronchogenicspread.Concerningcharacterizationoftheinfection asactiveornot,CTismoresensitivethanradiography,and18F-fluorodeoxyglucosepositronemission
tomography/CT(18F-FDGPET/CT)hasyieldedpromisingresultsthatneedfurtherconfirmation.The
diagnosisofextrapulmonaryTBsometimesremainsdifficult.Magneticresonanceimaging(MRI)isthe preferredmodalityinthediagnosisandassessmentoftuberculousspondylitis,while18F-FDGPETshows
superiorimageresolutioncomparedwithsingle-photon-emittingtracers.MRIisconsideredsuperiorto CTforthedetectionandassessmentofcentralnervoussystemTB.ConcerningabdominalTB,lymph nodesarebestevaluatedonCT,andthereisnoevidencethatMRIoffersaddedadvantagesindiagnosing hepatobiliarydisease.Asmetabolicchangesprecedemorphologicalones,theapplicationof18F-FDGPET/
CTwilllikelyplayamajorroleintheassessmentoftheresponsetoanti-TBtreatment.
ß2015TheAuthors.PublishedbyElsevierLtdonbehalfofInternationalSocietyforInfectiousDiseases. ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
* Correspondingauthor.
E-mailaddress:[email protected](J.Bomanji).
ContentslistsavailableatScienceDirect
International
Journal
of
Infectious
Diseases
j o urn a l hom e pa ge : ww w. e l s e v i e r. c om/ l o ca t e / i j i d
http://dx.doi.org/10.1016/j.ijid.2014.12.007
1201-9712/ß2015TheAuthors.PublishedbyElsevierLtdonbehalfofInternationalSocietyforInfectiousDiseases.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Primary TB is due to first-time exposure to Mycobacterium
tuberculosis. At radiology, primary PTB manifests as four main
entities–parenchymal disease,lymphadenopathy, pleural effu-sion,andmiliarydisease–oranycombinationthereof.1
Chestradiographycontinuestobethemainstayofdiagnosis. Typically,parenchymaldiseasemanifestsasconsolidationinany lobe,withpredominanceinthelowerandmiddlelobes.6Inthese cases,thebacterialinfectionsaremuchmorelikelytobethecause of such radiological features and hence the findings are non-specific, although primary infection should be suspected in individualsat risk of exposure to TB. Multilobar consolidation canbeseeninalmost25%ofcases.1Inapproximatelytwo-thirdsof cases, the parenchymal lesion resolves without sequelae on conventionalradiography.6 Intheremainder,aradiologicalscar persiststhatcanbecalcifiedinupto15%,whilepersistent mass-likeopacitiescalledtuberculomasareseeninapproximately9%of cases.6 Frequently,the only radiologicalevidence suggestive of previousTBistheso-calledRankecomplex:thecombinationofa parenchymalscar,calcifiedornot(Ghonlesion),andcalcifiedhilar and/orparatracheallymphnodes.5Destructionandfibrosisofthe lungparenchymaresultintheformationoftractionbronchiectasis withinthefibroticregion.5
The most common abnormality in children is lymph node enlargement,whichisseenin90–95%ofcases;bycomparison,in adultsthepercentagereachesupto43%.7Rightparatrachealand hilarlymphnodesarethemostcommonsitesofnodal involve-ment,althoughinvolvementisbilateralinaboutathirdofcases.CT ismoresensitivethanplainradiographyindetectingtuberculous lymphadenopathy.Itreveals nodes oftenmeasuringmore than 2cm,withaverycharacteristic,butnotpathognomonic,‘rimsign’ that consists of a low-density centre, representing caseous necrosis, surrounded by a peripheral enhancing rim due to granulomatousinflammatorytissue.8,9
Incontrasttolymphadenopathy,theprevalenceof radiographi-callydetectableparenchymalinvolvementissignificantlylowerin childrenupto3yearsold(51%)thaninolderchildren,amongwhom the prevalence is similar to the reported percentage in adults (80%).7,8Also,evolutiontocavitarydiseaseisrareinchildren.5
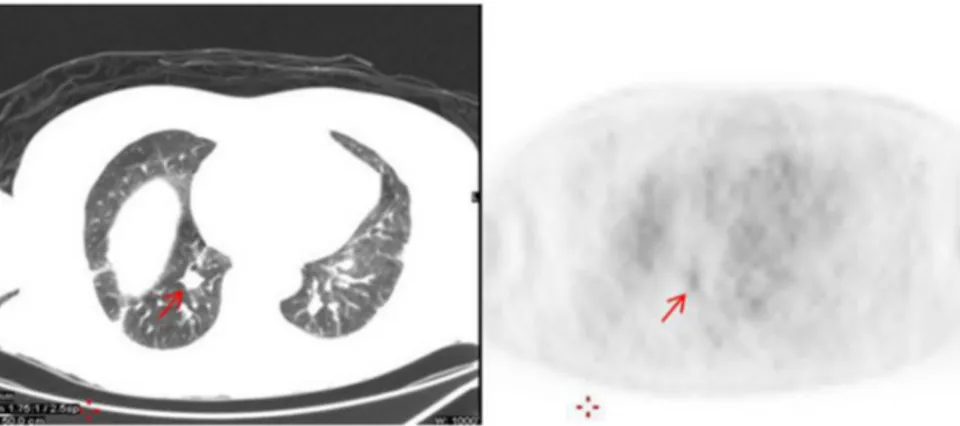
inability to distinguish tubercular from malignant lesions (Figure 1).11 Studies investigating the diagnostic value of dual time-point18F-FDGPET/CTimaginghaveshownlimitedpromise, but further investigations in larger series of patients are warranted.12,13
2.2. Post-primarytuberculosis
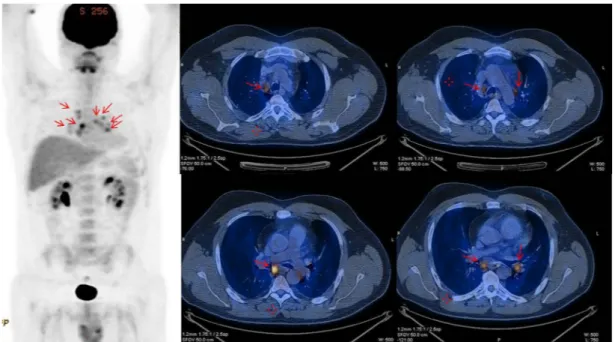
Post-primary PTB is one of the many terms (including reactivation,secondary,oradulthood)appliedtotheformofTB that develops and progresses under the influence of acquired immunity.5Themostcommonradiographicmanifestationof post-primary PTB is focal or patchy heterogeneous, poorly defined consolidationinvolvingtheapicalandposteriorsegmentsofthe upper lobes and the superior segments of the lower lobes (Figure2).14,15Inthemajorityofcases,morethanonepulmonary segmentisinvolved.6Cavitation,theradiologicalhallmarkofPTB, isradiographicallyevidentin20–45%ofpatients(Figure3),while air-fluidlevelsinthecavityoccurin10%ofcases.14,15Cavitation mayprogresstoendobronchialspreadandresultsinatypical ‘tree-in-bud’ distributionofnodules in additiontocavitation;this is consideredareliablemarkerofactiveTB.16High-resolutionCTis themethodofchoicetorevealearlybronchogenicspread,with 2-to 4-mm centrilobular nodules and sharply marginated linear branchingopacitiesaroundterminalandrespiratorybronchioles (tree-in-budsign).16Thetree-in-budsignistheconstellationof smallcentrilobularnodulesandconcomitantbranchingopacities, which mimics the branching pattern of a budding tree.17 The centrilobular nodulesare peripheral,spare thesubpleurallung, and denote the inflammatory lesions in the bronchioles and peribronchialalveoli.16,17Hilarormediastinallymphadenopathy isuncommoninpost-primaryPTB,seeninonly5–10%ofpatients (Figure4).18,19
Althoughpulmonarytuberculomasaremostoftentheresultof healedprimaryPTB,apulmonarytuberculomaisthemainoronly abnormalityonchestradiographsinapproximately5%ofpatients withreactivation.20TheCTscanshowsaroundorovalgranuloma, measuring from0.4 to 5cm in diameter,with a wall lined by
Figure1.Arrowsindicateamildly18
F-FDGavidrightlowerlobenodulemeasuring1.5cm(SUVmax2).Thedifferentialdiagnosisforthisnodulewouldincludecanceror
inflammatorygranulomatoustissueorencapsulatedbyconnective tissue.21Tuberculomascancavitate,whilecalcificationisfoundin 20–30%ofthem.21In80%ofcases,satellitelesionsareobservedin theimmediatevicinityofthe mainlesion.5Becauseofincreased glucosemetabolismcausedbyactivegranulomatousinflammation, tuberculomasmayaccumulate18F-FDG.22Maximumstandardized uptakevalues(SUVmax)tendnottobesignificantlydifferentfor tuberculousandmalignantlesions.23,24Onestudyhassuggested that unlike 18F-FDG PET, the 11C-choline PET scan can help to differentiate between lung cancer and tuberculoma, because tuberculomashowslowtraceruptakeon11C-cholinePETscan.25
2.3. Radiologicalpatternsinprimaryand/orpost-primaryPTB
Miliary pulmonary disease affects between 1% and 7% of patients withallforms ofTB.6 Itis usually seenin theelderly, infants, and immunocompromised persons.6 Initially, standard radiographsarenormalin25–40%ofcases.26CTcandemonstrate miliarydiseasebeforeitbecomesradiographicallyapparent,and its characteristic findings consist of innumerable 1- to 3-mm-diameternodules randomly distributed throughout both lungs, oftenassociatedwithintra-andinterlobularseptalthickening.14,27 Thenodulesusually resolvewithin2–6monthswithtreatment, withoutscarringorcalcification; however,theymaycoalesceto formfocalordiffuseconsolidation.6
A pleural effusion is seen in approximately one-fourth of patients with primary PTB and in 18% of post-primary PTB.26 Although, usually observed in association with parenchymal
and/ornodaldisease,pleuraleffusionhasbeenreportedtobethe only radiographicfinding indicative of primaryPTB in approxi-mately5%ofadultcases.26Pleuraleffusionisusuallyunilateraland onthesamesideastheprimaryfocusofPTB,whilecomplications suchaseffusion,empyema,andbronchopleuralfistulaarerare.6The CT scan of patientswith post-primary pleuraleffusiontypically shows smooth thickening of visceral and parietal pleura.28 Ultrasonographyoftendemonstratesacomplexseptatedeffusion.6 Fibrothorax with diffusepleuralthickening,but without pleural effusiononCT,suggestsinactivity.29The18F-FDGPET/CTscanmay demonstratediffuselyintense18F-FDGuptakeinthickenedpleura thatcanbeconfusedwithpleuralmesothelioma.30
2.4. DifferentiationbetweenactiveandinactiveTB
TBmakesitspresencefeltonimaginglongaftertheresolution of disease.Sometimes a questionthat needstobe answeredis whethertheinfectionisactiveornot.Activediseaseisingeneral characterizedbythepresenceofcentrilobularnodules,tree-in-bud pattern, thick-walled cavities, consolidation, miliary nodules, pleural effusions, or necrotic lymphadenopathy.1 Resolution to thin-walledsmoothcavities,fibrosis,andparenchymal,nodal,or pleuralcalcificationsoftendenotesinactivedisease.1
Chestradiographsmaybenormalorshowonlymildor non-specificfindingsinpatientswithactivedisease.26Thediagnosisof PTBwithradiographyisinitiallycorrectinonly49%ofallcases: 34% for primaryand 59% for post-primaryPTB.26On theother hand,CTcancorrectlydiagnose91%ofcasesofPTBandcorrectly Figure2.Trans-axialCTsectionshowingapatchy,heterogeneous,poorlydefinedconsolidationwithcavitatinglesionintheupperlobeoftherightlung.
Figure3.Leftpanel:CTimageshowinga1.61.2-cmcavitatinglesion(arrow)intheupperlobeoftherightlung.Rightpanel:thislesionshowsmild18
F-FDGuptakeonthe PETscan(smallarrow)(SUVmax2.2).Bottomleftpanel:Fused18F-FDGPET/CTimageshowingthesamecavitatingavidlesion(arrow).
characterize 80% of patients withactive disease and 89% with inactivedisease.31
CT is more sensitive than radiography in the detection and characterization of both parenchymal disease and mediastinal lymphadenopathy.9,32Inastudythatcomparedthetwomethods, high-resolutionCTshowedcavitiesin58%ofpatientswithactive PTB,whereaschestradiographsinonly22%.32Thediagnosisofactive PTBwasbasedonpositiveacid-fastbacilliinsputumandchangeson serialradiographsobtainedduringtreatment.32CTmayalsoshow pleuraldiseasethat isnot evidenton chestradiographyand be helpfulintheevaluationofpleuralcomplications.33
CT featurespredictiveofhighlyinfectious/activePTB include the following:34 (1) consolidation involving the apex or the posteriorsegmentoftherightupperlobeortheapico-posterior segmentof the leftupper lobe, (2) consolidation involving the superiorsegmentoftherightorleftlowerlobe,(3)acavitylesion, (4)clustersofnodules,and(5)absenceofcentrilobularnodules. High-resolutionCTisbetterthanchestradiographyinpredicting activePTB,withasensitivityof96%versus48%.35
Ithasbeenreported that18F-FDG PETisabletodifferentiate activePTBfromoldorinactivedisease,asactivetuberculomahas significantly higher SUVmax values compared with inactive tuberculoma.3When a SUV
maxof 1.05(at 60min) wasusedas thecut-off, thesensitivity andspecificity were100%and 100%, respectively.3Arecentstudyconcludedthat18F-FDGPET/CThas the potential to become a tool for monitoring the treatment responseinselectedcasesofEPTBormultidrugresistance.36An interestingstudyofpatientswithradiographiclesionssuggestive ofoldhealed TBaimedtogatherinformation onthemetabolic statusofTBlesionsusing18F-FDGPET/CTimaging.37Theauthors showedthatpatients with oldhealed TB lesionswitha higher SUVmaxmaybeathigherriskofactiveTB.37Furtherinvestigationis neededtoconfirmtheseresults.
3. Extrapulmonarytuberculosis
Despite recent advancesin imaging, the diagnosisof extra-pulmonary involvement sometimes remains difficult.38 The
imagingofsomefrequentextrapulmonarysitesofTBisreviewed below.
3.1. Musculoskeletaltuberculosis
Approximately50%ofcasesofskeletalTBinvolvethespine.6 Spondylodiscitis, also known as Pott’s disease, is the most commonform.39Theinfectionbeginsin subchondralboneand spreadsslowlytotheintervertebraldiskspaceandtheadjacent vertebralbodies,commonlyinthelowerdorsalandupperlumbar spine.40Failuretoidentifyandtreattheseareasofinvolvementat anearlystagemayleadtoseriouscomplicationssuchasvertebral collapse, spinal compression, and spinal deformity.38 Plain radiographyis normalearly inthedisease.1Thefirst signmay bedemineralizationoftheendplateswithresorptionandlossof densemargins.Asthediseaseprogresses,radiographywillshow progressivevertebralcollapsewithanteriorwedgingandgibbus formation.1 MRI is the preferred imaging modality in the diagnosis and assessment of tuberculous spondylitis.41,42 Be-causeoftheoftenmultifocalnatureofspinalTB,theMRIimaging oftheentirespinalcolumncouldbemoreeffectiveintheearly diagnosisofthedisease.43IncasesofspinalTB,thespinalcordis susceptible tomyelopathy secondary tocompression from an epidural abscess.6 The collapsed vertebra along with the epiduralcollection/abscessisalsobestevaluatedonMRI.6After antibioticadministrationisinitiated,repeatimagingisadvisedat approximately 4-weekintervals orat any time ifneurological deteriorationoccurs.44
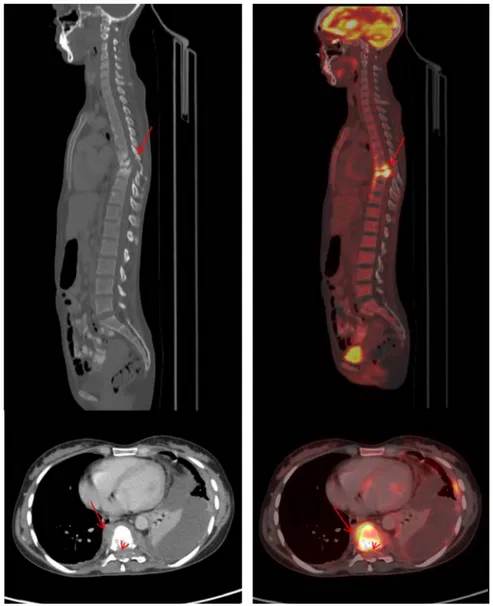
Astubercularlesionsdemonstratehigh18F-FDG uptake,18 F-FDGPET/CTis apromisingtechniqueforthediagnosisofspinal infection(Figures 5and6).45–48Aninterestingfindingwasthat 63.6% of patients with spinal TB had clinically occult non-contiguous multifocal skeletal involvement at the time of whole-body18F-FDGPET/CTscan.49
Besidesthespine,anypartofthemusculoskeletalsystemcan becomeinvolved,butthelargejointsofthelowerlimbsaremost commonlyaffected. Imagingfindings in musculoskeletalTB are oftennon-specific.MRI isthemostsensitive modality forearly diagnosisandcompletedelineationofthedisease.1
Figure4.Leftpanel:Multipleintensityprojectionimageshowing18
F-FDGuptakeinthemediastinalandbilateralhilarlymphnodes(arrows).Rightpanel:Multiplefused trans-axialsection18
3.2. Centralnervoussystem(CNS)tuberculosis
TBoftheCNSisahighlydevastatingformofthedisease.Various forms of involvement of the CNS are observed: parenchymal, meningeal, calvarial,spinal, or any combination thereof.1 MRIis generallyconsideredsuperiortoCTindetectingandassessingCNS TB.50Parenchymalinvolvementismostfrequentlyseenintheformof atuberculoma,whichmaybesingleormultiple.Inthepaediatricage groupitisseenmorefrequentlyinthecerebellum,whereasinadults ithasapredilectionforthecerebralhemispheresandbasalganglion. TheappearanceofatuberculomavariesonMRIdependingonits stageofmaturation.50,51Anon-caseatinggranulomaishyperintense onT2andhypointenseonT1andshowssolidenhancement,whilea solidcaseatinggranulomaisusuallyhypointenseonbothT1andT2 images.OnCT,tuberculomasappearasroundorlobulatedsofttissue masses with varying attenuation and homogeneous or ring enhancement.1Miliary TBis oftenassociatedwithTB meningitis and presents as small (<2mm) foci of hyperintensity on T2 acquisitions,whileaftergadoliniumadministration,T1imagesshow numerous,round, small,homogeneous,enhancinglesions.50 Con-trast-enhanced MRI is also superior toCT for the evaluationof meningitisanditscomplications,includinghydrocephalus.1
3.3. Abdominaltuberculosis
Abdominallymphadenopathyisthemostcommon manifesta-tionofabdominalTB,seenin55–66%ofpatients,andmayormay not be associated with other abdominal organ involvement.52 AbdominallymphnodesarebestevaluatedonCT,whichreveals enlargednodeswithhypoattenuatingcentresand hyperattenuat-ing enhancing rims.52,53 On MRI, the appearance is typically hypointenseon T1 images, whereas onT2 images thesignal is generallyhyperintenseorwithperipherallow-intensitysignal.1
Hepatic TB can be classified into local, miliary TB, or tuberculomas.54MiliaryTBisthemostcommonformofliverTB andisapartofgeneralizeddisease;innumerablesmallnodulesare foundontheliverwhichmayormaynotbeseenonCT,buton ultrasoundusuallypresentasbrightliverorspleenpatternsinthe formofadiffuseincreaseinechogenicity.54
Calcificationinthehepatic regionon plainradiographymay occasionallybeseeninlocalhepaticTB.54OnCT,livertuberculoma appears asa non-enhancing, central,low-densitylesion witha slightly enhancing peripheral rim,while liver calcificationscan also be demonstrated. MRI offers no added advantage in diagnosinghepatobiliaryTB.55
Figure5.CT(leftpanel)and18F-FDGPET/CTfusedimages(rightpanel):trans-axialandsagittalsections.Moderatetointense18F-FDGuptakeisseeninaparavertebralsoft
tissuemasslesionextendingfromthelevelofT7–T10vertebraewithassociatedlyticscleroticchangesinT7–T9vertebraeandcollapseoftheT8vertebra(arrows).Thelesion infiltratesintothespinalcanalattheleveloftheT8vertebraandinvolvesthespinalcord(smallarrow).Thelesionisseentoextendalongtheleftcostalmargin,withfaint18
F-FDGuptakeandfociofcalcification,likelyrepresentingacoldabscess(courtesyofProf.B.R.Mittal).
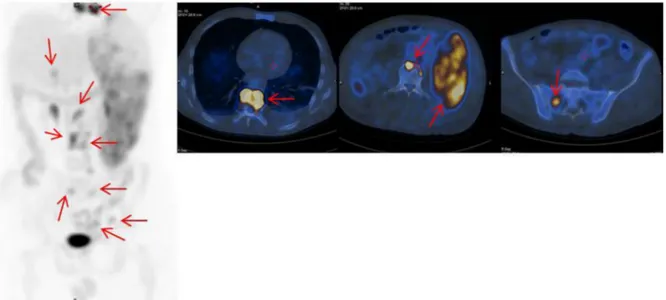
Few reports are available on 18F-FDG PET/CT imaging in abdominalTB,showingthattheappearanceofabdominalTB is non-specificandvaried(Figure6).56–58
4. Assessmentoftreatmentresponse
Thisispotentiallythemostimportantclinicalapplicationof18 F-FDGPET/CTinTB.Duringanti-TBtreatment,somebacillus-negative tuberculomasdonotdecreaseinsizeandmayevenincrease,making itdifficultfor thephysiciantodecidewhetherornottomodify treatment.Inthesecases,18F-FDGPET/CTimagingmayhelp,asthe changes in glycolytic activity within the inflammatory lesion, measured by 18F-FDG uptake, correlate well with the clinical markersofresponse.49Severalstudieshaveconfirmedthevalueof
18F-FDGPET/CTinthefollow-upandevaluationofthetreatment response,especiallyinpatientswithextrapulmonaryinvolvement andwhendrugresistanceisprevalent.57,59–63In pulmonaryand extrapulmonary TB, a decrease of approximately one-third in SUVmaxhasbeenreportedafter1monthofanti-TBtreatmentwhen thereisagoodresponse.60InitialdatahasshownthatSUV
max(both earlyand delayed)ofinvolvedlymphnodes andthe numberof involved lymph node basins are significantly higher in non-respondersthan inresponders.64Thesefindingswarrantfurther confirmationinlargercohortsofpatients.
After4 monthsofanti-TBtreatment18F-FDGPET/CTcanalso evaluatethetreatmentresponseinpatientswithhighsensitivityand specificity,usingthevalueof4.5astheSUVmaxcut-off.62
Otherauthorshaveaimedtomonitorthemetabolicchangesin spinalTB during the course oftherapy.49 Themean changesin SUVmax at various time points – from baseline to 6, 12, and 18months,from6to12months,from6to18months,andfrom12to 18months–werecalculatedandfoundtobehighlysignificant(p -value<0.001).4918F-FDGPET/CTalsoshowsencouragingresultsfor theprognosis anddetection ofresidual diseasein patientswith spinalinfection,particularlywhenMRIisunconvincingin distin-guishingbetweendegenerativechangesandinfection.65
5. TuberculosisinHIVpatients
The diagnosis of active PTB is a majorchallenge, especially in individuals with severe immunosuppression, such as those
co-infected with HIV. Such patients characteristically demon-strateanatypicalradiographic pattern,forexamplemiddleand lower lunginvolvement, absence of cavity formation, presence oflymphadenopathyandpleuraleffusions,oramiliarypattern.38 TheradiographicappearanceofHIV-associatedPTB hasbeen foundtobedependentonthelevelofimmunosuppressionatthe time of overt disease.66 Radiologicalmanifestations in patients with a CD4 T-lymphocyte count of <200/mm3 show a higher incidenceofmediastinalorhilarlymphnodeenlargement,alower prevalenceofcavitation,andoftenextrapulmonaryinvolvement comparedwithHIVpatientswithaCD4T-lymphocytecountof
200/mm3.66AstudyperformedtodeterminetheCTspectrumof PTBinHIVpatientsshowednodularopacities(in78.5%ofcases), consolidation(46.4%),lymphadenopathy(35.7%),pleuraleffusion (35.7%), ground glass opacity (21.4%), and cavitation (21.4%).67 Otherauthorshavereportedthatfeaturesofpost-primaryPTBare patchyconsolidationwithinvolvementatunusualsites.68 Cavita-tionis less common atlower CD4counts.Patients withsevere immunosuppression have an increased incidence of miliary pulmonary disease, withdiffuse, randomly distributed nodules onCT.69Mediastinalandhilarlymphadenopathyoccursin75–77% ofcasesandismorecommonlyseeninHIV-positivethanin HIV-negativepatients.68Extrapulmonarylocalizationsarefrequentin HIV-infected patients and may involve brain, pericardium, gastrointestinal tract, peritoneum, and genitourinary tract.70 Currently thereareno datatosupporttheuseof 18F-FDGPET/ CTinthispatientgroup.
Funding:None.
Ethicalapproval:Ethicalapprovalwasnotrequired.
Conflictofinterest:Allauthorshavenocompetingintereststo
declare.
References
1.BomanjiJB,GuptaN,GulatiP,DasCJ.Imagingintuberculosis.In:KaufmannSH, RubinE,ZumlaA,editors.Clinicaltuberculosis.NewYork:ColdSpringHarbor LaboratoryPress;2014.
2.Jones HA, ClarkRJ, Rhodes CG, SchofieldJB, Krausz T,Haslett C. Invivo measurementofneutrophilactivityinexperimentallunginflammation.AmJ RespirCritCareMed1994;149:1635–9.
3.KimIJ,LeeJS,KimSJ,KimYK,JeongYJ,JunS,etal.Double-phase18F-FDG PET-CTfordeterminationofpulmonarytuberculomaactivity.EurJNuclMedMol Imaging2008;35:808–14.
Figure6.Multipleintensityprojectionimage(leftpanel)andfusedtrans-axialsection18
F-FDGPET/CTimages(rightpanel)showing18
F-FDGuptakeinmultiplelymphnodes (SUVmax6.8)(portahepatis,portacaval,para-aortic,retroperitoneal,bilateralinternaliliac,leftexternaliliac,andleftinguinal(arrows))andheterogeneous18F-FDGuptakein
thegrosslyenlargedspleen(SUVmax10.2)(arrow)andinbones(T8vertebracoupledwithparavertebralsofttissueuptake(SUVmax17.6),L3vertebralbodyanteriorly(SUVmax
4.HahmCR,ParkHY,JeonK,UmSW,SuhGY,ChungMP,etal.Solitarypulmonary nodules caused by Mycobacterium tuberculosis and Mycobacterium avium complex.Lung2010;188:25–31.
5.VanDyckP,VanhoenackerFM,VandenBrandeP,DeSchepperAM.Imagingof pulmonarytuberculosis.EurRadiol2003;13:1771–85.
6.BurrillJ,WilliamsCJ,BainG,ConderG,HineAL,MisraRR.Tuberculosis:a radiologicreview.Radiographics2007;27:1255–7.
7.LeungAN,MullerNL,PinedaPR,FitzGeraldJM.Primarytuberculosisin child-hood:radiographicmanifestations.Radiology1992;182:87–91.
8.PomboF,RodriguezE,MatoJ,Perez-FontanJ,RiveraE,ValvuenaL.Patternsof contrastenhancementoftuberculouslymphnodesdemonstratedbycomputed tomography.ClinRadiol1992;46:13–7.
9.KimWS,MoonWK,KimIO,LeeHJ,ImJG,YeonKM,etal.Pulmonary tubercu-losisinchildren:CTevaluation.AmJRoentgenol1997;168:1005–9.
10.SoussanM,BrilletPY,MekinianA,KhafagyA,NicolasP,VessieresA,BraunerM. PatternsofpulmonarytuberculosisonFDG-PET/CT.EurJRadiol2012;81:2872–6.
11.LiY, SuM,LiF, KuangA,TianR. Thevalueof (18)F-FDG-PET/CTinthe differentialdiagnosisof solitary pulmonarynodules inareas witha high incidenceoftuberculosis.AnnNuclMed2011;25:804–11.
12.YenRF,ChenKC,LeeJM,ChangYC,WangJ,ChengMF,etal.18F-FDGPETforthe lymphnodestagingofnon-smallcelllungcancerinatuberculosis-endemic country:isdualtimepointimagingworththeeffort?EurJNuclMedMolImaging 2008;35:1305–15.
13.RazakHR,Geso M,AbdulRahimN,NordinAJ.Imaging characteristicsof extrapulmonarytuberculosislesionsondualtimepointimaging(DTPI)of FDGPET/CT.JMedImagingRadiatOncol2011;55:556–62.
14.LeungAN.Pulmonarytuberculosis:theessentials.Radiology1999;210:307–22.
15.KryslJ,Korzeniewska-KoselaM,MullerNL,FitzGeraldJM.Radiologicfeatures ofpulmonarytuberculosis:anassessmentof188cases.CanAssocRadiolJ 1994;45:101–7.
16.LeeKS,ImJG.CTinadultswithtuberculosisofthechest:characteristicfindings androleinmanagement.AJRAmJRoentgenol1995;164:1361–7.
17.Verma N, Chung JH, Mohammed TL. Tree-in-bud sign. J Thorac Imaging 2012;27:W27.
18.Curvo-SemedoL,TeixeiraL,Caseiro-AlvesF.Tuberculosisofthechest.EurJ Radiol2005;55:158–72.
19.RodriguezE,SolerR,Juffe´ A,Salgado L.CTandMRfindingsinacalcified myocardial tuberculoma of the left ventricle. J Comput Assist Tomogr 2001;25:577–9.
20.SochockyS.Tuberculomaofthelung.AmRevTuberc1958;78:403–10.
21.LeeKS,SongKS,LimTH,KimPN,KimIY,LeeBH.Adult-onsetpulmonary tuberculosis:findingsonchestradiographsandCTscans.AmJRoentgenol 1993;160:753–8.
22.GooJM,ImJG,DoKH,YeoJS,SeoJB,KimHY,etal.Pulmonarytuberculoma evaluatedbymeansofFDGPET:findingsin10cases.Radiology2000;216: 117–21.
23.SathekgeMM,MaesA,PottelH,StoltzA,vandeWieleC.Dualtime-pointFDG PET-CTfordifferentiatingbenignfrommalignantsolitarypulmonarynodules inaTBendemicarea.SAfrMedJ2010;100:598–601.
24.ChenCJ,LeeBF,YaoWJ,ChengL,WuPS,ChuCL,etal.Dual-phase18F-FDGPET inthediagnosisofpulmonarynoduleswithaninitialstandarduptakevalueless than2.5.AJRAmJRoentgenol2008;191:475–9.
25.HaraT,KosakaN,SuzukiT,KudoK,NiinoH.Uptakeratesof 18F-fluorodeox-yglucoseand11C-cholineinlungcancerandpulmonarytuberculosis:a posi-tronemissiontomographystudy.Chest2003;124:893–901.
26.JeongYJ,LeeKS.Pulmonarytuberculosis:up-to-dateimagingand manage-ment.AJRAmJRoentgenol2008;191:834–44.
27.KwongJS,CarignanS,KangEY,MullerNL,FitzGeraldJM.Miliarytuberculosis: diagnosticaccuracyofchestradiography.Chest1996;110:339–42.
28.YilmazMU,Kumcuoglu Z,UtkanerG, YalnizO, ErkmenG. CTfindingsof tuberculouspleurisy.IntJTubercLungDis1998;2:164–7.
29.KimY, Song KS,Goo JM,Lee JS,Lee KS,Lim TH. Thoracic sequelaeand complicationsoftuberculosis.Radiographics2001;21:839–58.
30.YehCL,ChenLK,ChenSW,ChenYK.AbnormalFDGPETimagingintuberculosis appearinglikemesothelioma:anatomicdelineationbyCTcanaidindifferential diagnosis.ClinNuclMed2009;34:815–7.
31.LeeKS,HwangJW,ChungMP,KimH,KwonOJ.UtilityofCTintheevaluationof pulmonarytuberculosisinpatientswithoutAIDS.Chest1996;110:977–84.
32.ImJG,ItohH,ShimYS,LeeJH,AhnJ,HanMC,etal.Pulmonarytuberculosis:CT findings—earlyactive disease andsequentialchangewith antituberculous therapy.Radiology1993;186:653–60.
33.HulnickDH, Naidich DP, McCauley DI. Pleural tuberculosisevaluated by computedtomography.Radiology1983;149:759–65.
34.YehJJ,ChenSC,TengWB,ChouCH,HsiehSP,LeeTL,etal.Identifyingthemost infectiouslesionsinpulmonarytuberculosisbyhigh-resolutionmulti-detector computedtomography.EurRadiol2010;20:2135–45.
35.RanigaS,ParikhN,AroraA.IsHRCTreliableindeterminingdiseaseactivityin pulmonarytuberculosis.IndianJRadiolImaging2006;16:221–8.
36.HeysellSK,ThomasTA,SifriCD,RehmPK,HouptER.18-Fluorodeoxyglucose positronemissiontomographyfortuberculosisdiagnosisandmanagement:a caseseries.BMCPulmMed2013;13:14.
37.JeongYJ,PaengJC,NamHY,LeeJS,LeeSM,YooCG,etal.(18)F-FDG positron-emissiontomography/computedtomographyfindingsofradiographiclesions suggestingoldhealedtuberculosis.JKoreanMedSci2014;29:386–91.
38.VorsterM,SathekgeMM,BomanjiJ.Advancesinimagingoftuberculosis:the roleof18F-FDGPETandPET/CT.CurrOpinPulmMed2014;20:287–93.
39.MartiniM,OuahesM.Boneandjointtuberculosis:areviewof652cases. Orthopedics1988;11:861–6.
40.WeaverP,LifesoR.Theradiologicaldiagnosisoftuberculosisoftheadultspine. SkeletalRadiol1984;12:178–86.
41.HoffmanEB,CrosierJH,CreminBJ.Imaginginchildrenwithspinaltuberculosis: acomparisonofradiography,computedtomographyandmagneticresonance imaging.JBoneJointSurgBr1993;75:233–9.
42.ModicMT,FeiglinDH,PirainoDW,BoumphreyF,WeinsteinMA,Duchesneau PM,etal.Vertebralosteomyelitis:assessmentusingMR.Radiology1985;157: 157–66.
43.Akman S,SirvanciM,TaluU, GogusA,HamzaogluA.Magneticresonance imagingoftuberculousspondylitis.Orthopedics2003;26:69–73.
44.GabrielliA,LayonAJ,YuM.Chapter73:Neurologicalinfections.In:Civetta, Taylor,andKirby’s(Eds)manualofcriticalcare2012,LippincottWilliams& Wilkins;Philadelphia.
45. LeeIS,LeeJS,KimSJ,JunS,SuhKT.Fluorine-18-fluorodeoxyglucosepositron emissiontomography/computedtomographyimaginginpyogenicand tu-berculousspondylitis:preliminarystudy.JComputAssistTomogr2009;33: 587–92.
46.GratzS,Do¨rnerJ,FischerU,BehrTM,Be´he´ M,AltenvoerdeG,etal.18F-FDG hybridPETinpatientswithsuspectedspondylitis.EurJNuclMedMolImaging 2002;29:516–24.
47.Rivas-GarciaA,Sarria-EstradaS,Torrents-OdinC,Casas-GomilaL,FranquetE. ImagingfindingsofPott’sdisease.EurSpineJ2013;22(Suppl4):567–78.
48.KimSJ,LeeJS,Suh KT,KimIJ,KimYK.Differentiationoftuberculousand pyogenicspondylitisusingdoublephaseF-18FDGPET.OpenMedImagingJ 2008;2:1–6.
49.DurejaS,SenIB,AcharyaS.PotentialroleofF18FDGPET-CTasanimaging biomarkerforthenoninvasiveevaluationinuncomplicatedskeletal tubercu-losis:aprospectiveclinicalobservationalstudy.EurSpineJ2014[Epubaheadof print].
50.TrivediR,SaksenaS,GuptaRK.Magneticresonanceimagingincentralnervous systemtuberculosis.IndianJRadiolImaging2009;19:256–65.
51.CelsoL,daCruzJrH,DominguesRC.Intracranialinfections. In:AtlasSW, editor.Magneticresonanceimagingofthebrainandspine.4thed.,Philadelphia: LippincottWilliams&Wilkins;2009.p.929–1026.
52.Leder RA, Low VH. Tuberculosis of the abdomen. Radiol Clin North Am 1995;33:691–705.
53.DentonT,HossainJ.AradiologicalstudyofabdominaltuberculosisinaSaudi population,withspecialreferencetoultrasoundandcomputedtomography. ClinRadiol1993;47:409–14.
54.ChaudharyP.Hepatobiliarytuberculosis.AnnGastroenterol2014;27:207–11.
55.ReedDH,NashAF,ValabhjiP.Radiologicaldiagnosisandmanagementofa solitarytuberculoushepaticabscess.BrJRadiol1990;63:902–4.
56.TakalkarAM,BrunoGL,ReddyM,LilienDL.IntenseFDGactivityinperitoneal tuberculosismimicsperitonealcarcinomatosis.ClinNuclMed2007;32:244–6.
57.TianG,XiaoY,ChenB,XiaJ,GuanH,DengQ.FDGPET/CTfortherapeutic responsemonitoringinmulti-sitenon-respiratorytuberculosis.Acta Radiol 2010;51:1002–6.
58.JeffryL,KerrouK,CamatteS,LelievreL,MetzgerU,RobinF,etal.Peritoneal tuberculosisrevealedbycarcinomatosisonCTscananduptakeatFDG-PET. BJOG2003;110:1129–31.
59.ParkIN,RyuJS,ShimTS.Evaluationoftherapeuticresponseoftuberculoma usingF-18FDGpositronemissiontomography.ClinNuclMed2008;33:1–3.
60.MartinezV,Castilla-LievreMA,Guillet-CarubaC,GrenierG,FiorR,DesarnaudS, et al.(18)F-FDGPET/CT intuberculosis:an early non-invasivemarker of therapeuticresponse.IntJTubercLungDis2012;16:1180–5.
61.ParkYH,YuCM,KimES,JungJO,SeoHS,LeeJH,etal.Monitoringtherapeutic responseinacaseofextrapulmonarytuberculosisbyserialF-18FDGPET/CT. NuclMedMolImaging2012;46:69–72.
62.SathekgeM,MaesA,D’AsselerY,VorsterM,GongxekaH,VandeWieleC. Tuberculouslymphadenitis:FDGPETandCTfindingsinresponsiveand non-responsivedisease.EurJNuclMedMolImaging2012;39:1184–90.
63.Hofmeyr A, LauWF, SlavinMA. Mycobacterium tuberculosis infectionin patients withcancer,theroleof18-fluorodeoxyglucosepositron emission tomographyfordiagnosisandmonitoringtreatmentresponse.Tuberculosis (Edinb)2007;87:459–63.
64.SathekgeM,MaesA,KgomoM,StoltzA,VandeWieleC.Useof18F-FDGPETto predictresponsetofirst-linetuberculostaticsinHIV-associatedtuberculosis.J NuclMed2011;52:880–5.
65.KimSJ,KimIJ,SuhKT,KimYK,LeeJS.Predictionofresidualdiseaseofspine infectionusingF-18FDGPET/CT.Spine(PhilaPa1976)2009;34:2424–30.
66.LeungAN,BraunerMW,GamsuG,Mlika-CabanneN,BenRomdhaneH,Carette MF,etal.Pulmonarytuberculosis:comparisonofCTfindingsin HIV-seroposi-tiveandHIV-seronegativepatients.Radiology1996;198:687–91.
67.AtwalSS,PuranikS,MadhavRK,KsvA,SharmaBB,GargaUC.Highresolution computed tomography lung spectrum in symptomatic adultHIV-positive patientsinSouth-EastAsiannation.JClinDiagnRes2014;8:RC12–6.
68.FengF,Yu-xinS, Gan-linX,YingZ,Hong-zhouLu, Zhi-yongZ.Computed tomography inpredictingsmear-negative pulmonarytuberculosis inAIDS patients.ChinMedJ2013;126:3228–33.
69.AllenCM,Al-JahdaliHH,IrionKL,GhanemSA,GoudaA,KhanAN.Imaginglung manifestationsofHIV/AIDS.AnnThoracMed2010;5:201–16.
70.RaviglioneMC,NarainJP,KochiA.HIV-associatedtuberculosisindeveloping countries:clinicalfeatures,diagnosis,andtreatment.BullWorldHealthOrgan 1992;70:515–26.