Use of the current edition of the electronic version of this book (eBook) is subject to the terms of the nontransferable, limited license granted on studentconsult.inkling.com. Access to the eBook is limited to the first individual who redeems the PIN, located on the inside cover of this book, at studentconsult.inkling.com and may not be transferred to another party by resale, lending, or other means.
Any screen.
Any time.
Anywhere.
Activate the eBook version of this title at no additional charge.
Unlock your eBook today.
Scratch off your code
Type code into “Enter Code” box Click “Redeem”
Log in or Sign up Go to “My Library”
It’s that easy!
Student Consult eBooks give you the power to browse and find content, view enhanced images, share notes and highlights—both online and offline.
For technical assistance:
email [email protected] call 1-800-401-9962 (inside the US) call +1-314-447-8200 (outside the US)
Scan this QR code to redeem your eBook through your mobile device:
n.
.
arge.
Place Peel Off Sticker Here
2015v1.0
1 2 3 4 5 6
Visitstudentconsult.inkling.com/redeem
Davidson’s
Essentials of
Medicine
This page intentionally left blank
Davidson’s
Essentials of 3rd Edition Medicine
Edited by
J. Alastair Innes PhD FRCP (Ed)
Consultant Physician and Honorary Reader in Respiratory Medicine
Western General Hospital Edinburgh, United Kingdom
For additional online content visit StudentConsult.com
Edinburgh London New York Oxford Philadelphia St Louis Sydney 2021
© 2021, Elsevier Limited. All rights reserved.
First edition 2009 Second edition 2016 Third edition 2020
No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with orga- nizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions.
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Notices
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds or experiments described herein. Because of rapid advances in the medi- cal sciences, in particular, independent verification of diagnoses and drug dosages should be made. To the fullest extent of the law, no responsibility is assumed by Elsevier, authors, editors or contributors for any injury and/
or damage to persons or property as a matter of products liability, negli- gence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
ISBN: 978- 0- 7020- 7875- 0 978- 0- 7020- 7876- 7
Executive Content Strategist: Laurence Hunter Content Development Specialist: Carole McMurray Content Coordinator: Susan Jansons
Project Manager: Louisa Talbott/Anne Collett Design: Brian Salisbury
Illustration Manager: Paula Catalano Illustrator: TNQ
Marketing Manager: Deborah Watkins Printed in the UK
Last digit is the print number: 9 8 7 6 5 4 3 2 1
Contents
Sir Stanley Davidson vi
Preface vii Acknowledgements viii Contributors to Davidson’s Principles and Practice of Medicine, 23rd Edition ix
List of abbreviations ivx
Picture credits xvi
1. Clinical decision making 1
2. Clinical therapeutics and prescribing 11
3. Poisoning 43
4. Acute medicine and critical illness 57
5. Infectious disease 99
6. Clinical biochemistry and metabolic medicine 187
7. Nephrology and urology 207
8. Cardiology 249
9. Respiratory medicine 311
10. Endocrinology 369
11. Diabetes mellitus 419
12. Gastroenterology 449
13. Hepatology 509
14. Haematology and transfusion medicine 553
15. Rheumatology and bone disease 593
16. Neurology 637
17. Medical ophthalmology 713
18. Dermatology 733
19. Ageing and disease 775
20. Oncology 785
21. Laboratory reference ranges 811
Index 821
Sir Stanley Davidson (1894–1981)
Davidson’s Principles and Practice of Medi- cine was the brainchild of one of the great Professors of Medicine of the 20th century.
Stanley Davidson was born in Sri Lanka and began his medical undergraduate training at Trinity College, Cambridge; this was inter- rupted by World War I and later resumed in Edinburgh. He was seriously wounded in battle, and the carnage and shocking waste of young life that he encountered at that time had a profound effect on his sub- sequent attitudes and values.
In 1930 Stanley Davidson was appointed Professor of Medicine at the University of Aberdeen, one of the first full- time Chairs of Medicine anywhere and the first in Scotland. In 1938 he took up the Chair of Medicine at Edinburgh and was to remain in this post until retirement in 1959. He was a renowned educator and a particularly gifted teacher at the bedside, where he taught that everything had to be questioned and explained. He himself gave most of the systematic lectures in Medicine, which were made available as typewritten notes that emphasised the essentials and far surpassed any textbook available at the time.
Principles and Practice of Medicine was conceived in the late 1940s with its origins in those lecture notes. The first edition, published in 1952, was a masterpiece of clarity and uniformity of style. It was of modest size and price, but sufficiently comprehensive and up to date to provide students with the main elements of sound medical practice. Although the format and presentation have seen many changes in 21 subsequent editions, Sir Stan- ley’s original vision and objectives remain. More than half a century after its first publication, his book continues to inform and educate students, doc- tors and health professionals all over the world.
Preface
In the 67 years since Davidson’s Principles and Practice of Medicine was first published, the profusion of molecular and genetic knowledge about disease, and of the number of diagnostic tests and possible treatments, has posed an increasing challenge to those seeking to summarise clinical medicine in a single textbook. An inevitable consequence has been a parallel growth in the physical size of all the major textbooks, including Davidson.
Davidson’s Essentials of Medicine seeks to complement the parent volume by helping those who also need portable information to study on the move – whether commuting, travelling between training sites or during remote attachments and electives. In this third edition, the entire content of Essentials has been comprehensively revised and updated in line with the core content from Davidson, while retaining a size which can easily accom- pany readers on their travels. Although the text is concise, every effort has been made to maximise readability and to avoid dry and unmemorable lists; the intention has been to produce a genuine miniature textbook. The text draws directly on the enormous depth and breadth of experience of the parent Davidson writing team and presents the essential elements in a format to suit hand luggage. Key Davidson illustrations have been adapted and retained, and new sections include chapters on Clinical therapeutics and prescribing, Acute medicine and critical care, Medical ophthalmology and Oncology.
In an age when on-line information is ever more accessible to doctors in training, most still agree that there is no substitute for the physical page when systematic study is needed. With this book, we hope that the proven value of the parent Davidson can be augmented by making the essential elements accessible while on the move.
J.A.I.
Edinburgh 2020
Acknowledgements
I am very grateful to the chapter authors of Davidson’s Principles and Practice of Medicine, without whom this project would have been impos- sible. I would also like to acknowledge the invaluable contribution of the team of assistant editors who helped to sift and select the relevant informa- tion during preparation of the first edition: Kenneth Baillie, Sunil Adwani, Donald Noble, Sarah Walsh, Nazir Lone, Jehangir Din, Neeraj Dhaun and Alan Japp.
I remain indebted to Nicki Colledge and Brian Walker for inviting me to help create Essentials and for their support and guidance in the early stages.
Thanks also to Laurence Hunter, Carole McMurray, Louisa Talbott and Anne Collett at Elsevier for their support and meticulous attention to detail.
Finally, I would like to thank Hester and all my family for their encour- agement and support during the preparation of this book, and to dedicate it to the memory of my father, James Innes, who worked with Stanley Davidson on the early editions of Davidson’s Principles and Practice of Medicine.
J.A.I.
Edinburgh 2020
Contributors to Davidson’s Principles and Practice of Medicine, 23rd Edition
The core of this book is based on the contents of Davidson’s Principles and Practice of Medicine, with material extracted and re-edited to make a uniform presentation to suit the format of this book. Although some chapters and topics have, by necessity, been cut or substantially edited, contributors of all chapters drawn upon have been acknowledged here in recognition of their input into the totality of the parent textbook.
Brian J Angus BSc, DTM&H, FRCP, MD, FFTM(Glas)
Associate Professor, Nuffield Department of Medicine, University of Oxford, UK Quentin M Anstee BSc(Hons), PhD, MRCP
Senior Lecturer, Institute of Cellular Medicine, Newcastle University, Newcastle upon Tyne; Honorary Consultant Hepatologist, Freeman Hospital, Newcastle upon Tyne, UK
Leslie Burnett MBBS, PhD, FRCPA, FHGSA
Medical Director, Garvan Institute of Medical Research, Sydney; Conjoint Professor, St Vincent’s Clinical School, Faculty of Medicine, University of New South Wales; Honorary Professor in Pathology and Genetic Medicine, Faculty of Medicine, Sydney Medical School; Honorary Associate of the School of Information Technologies, University of Sydney, Australia
Mark Byers OBE, MRCGP, MCEM, MFSEM, DA(UK)
General Practitioner, Ministry of Defence, Royal Centre for Defence Medicine, University Hospitals Birmingham, UK
Harry Campbell MD, FRCPE, FFPH, FRSE
Professor of Genetic Epidemiology and Public Health, Centre for Global Health Research, Usher Institute of Population Health Sciences and Informatics, University of Edinburgh, UK
Gavin PR Clunie BSc, MD, FRCP
Consultant Rheumatologist and Metabolic Bone Physician, Cambridge University Hospitals NHS Foundation Trust, Addenbrooke’s Hospital, Cambridge, UK
Lesley A Colvin BSc, FRCA, PhD, FRCPE, FFPMRCA
Consultant, Department of Anaesthesia, Critical Care and Pain Medicine, Western General Hospital, Edinburgh; Honorary Professor in Anaesthesia and Pain Medicine, University of Edinburgh, UK
Bryan Conway MB, MRCP, PhD
Senior Lecturer, Centre for Cardiovascular Science, University of Edinburgh;
Honorary Consultant Nephrologist, Royal Infirmary of Edinburgh, UK Nicola Cooper FAcadMEd, FRCPE, FRACP
Consultant Physician, Derby Teaching Hospitals NHS Foundation Trust, Derby;
Honorary Clinical Associate Professor, Division of Medical Sciences and Graduate Entry Medicine, University of Nottingham, UK
Alison L Cracknell FRCP
Consultant, Medicine for Older People, Leeds Teaching Hospitals NHS Trust, Leeds; Honorary Clinical Associate Professor, University of Leeds, UK Dominic J Culligan BSc, MD, FRCP, FRCPath
Consultant Haematologist, Aberdeen Royal Infirmary, Aberdeen; Honorary Senior Lecturer, University of Aberdeen, UK
Graham G Dark FRCP, FHEA
Senior Lecturer in Medical Oncology and Cancer Education, Newcastle University, Newcastle upon Tyne, UK
Richard J Davenport DM, FRCPE, BMedSci
Consultant Neurologist, Royal Infirmary of Edinburgh and Western General Hospital, Edinburgh; Honorary Senior Lecturer, University of Edinburgh, UK David H Dockrell MD, FRCPI, FRCPG, FACP
Professor of Infection Medicine, Medical Research Council/University of Edinburgh Centre for Inflammation Research, University of Edinburgh, UK Emad El- Omar BSc(Hons), MD(Hons), FRCPE, FRSE
Professor of Medicine, St George and Sutherland Clinical School, University of New South Wales, Sydney, Australia
Marie Fallon MD, FRCP
St Columba’s Hospice Chair of Palliative Medicine, University of Edinburgh, UK David R FitzPatrick MD, FRCPE
Professor, Medical Research Council Human Genetics Unit, Institute of Genetics and Molecular Medicine, University of Edinburgh, UK
Neil R Grubb MD, FRCP
Consultant in Cardiology, Royal Infirmary of Edinburgh; Honorary Senior Lecturer in Cardiovascular Sciences, University of Edinburgh, UK
Sally H Ibbotson BSc(Hons), MD(with commendation), FRCPE Professor of Dermatology, University of Dundee, UK
J Alastair Innes BSc, PhD, FRCPE
Consultant, Respiratory Unit, Western General Hospital, Edinburgh; Honorary Reader in Respiratory Medicine, University of Edinburgh, UK
Sara J Jenks BSc(Hons), MRCP, FRCPath
Consultant in Metabolic Medicine, Department of Clinical Biochemistry, Royal Infirmary of Edinburgh, UK
Sarah L Johnston FCRP, FRCPath
Consultant Immunologist, Department of Immunology and Immunogenetics, North Bristol NHS Trust, Bristol, UK
David EJ Jones MA, BM, PhD, FRCP
Professor of Liver Immunology, Institute of Cellular Medicine, Newcastle University, Newcastle upon Tyne; Consultant Hepatologist, Freeman Hospital, Newcastle upon Tyne, UK
Peter Langhorne PhD, FRCPG
Professor of Stroke Care, Institute of Cardiovascular and Medical Sciences, University of Glasgow, UK
Stephen M Lawrie MD(Hons), FRCPsych, FRCPE(Hon) Professor of Psychiatry, University of Edinburgh, UK John Paul Leach MD, FRCPG, FRCPE
Consultant Neurologist, Institute of Neuroscience, Southern General Hospital, Glasgow; Head of Undergraduate Medicine and Honorary Associate Clinical Professor, University of Glasgow, UK
Gary Maartens MBChB, FCP(SA), MMed
Professor of Medicine, University of Cape Town, South Africa Lucy Mackillop BM, MA(Oxon), FRCP
Consultant Obstetric Physician, Oxford University Hospitals NHS Foundation Trust, Oxford; Honorary Senior Clinical Lecturer, Nuffield Department of Obstetrics and Gynaecology, University of Oxford, UK
Michael J MacMahon FRCA, FICM, EDIC
Consultant in Anaesthesia and Intensive Care, Victoria Hospital, Kirkcaldy, UK Rebecca Mann BMedSci MRCP, FRCPCh
Consultant Paediatrician, Taunton and Somerset NHS Foundation Trust, Taunton, UK
Lynn M Manson MD, FRCP, FRCPath
Consultant Haematologist, Scottish National Blood Transfusion Service, Edinburgh; Honorary Clinical Senior Lecturer, Department of Transfusion Medicine, Royal Infirmary of Edinburgh, UK
Sara E Marshall FRCP, FRCPath, PhD
Professor of Clinical Immunology, Medical Research Institute, University of Dundee, UK
Amanda Mather MBBS, FRACP, PhD
Renal Staff Specialist, Department of Renal Medicine, Royal North Shore Hospital, Sydney; Conjoint Senior Lecturer, Faculty of Medicine, University of Sydney, Australia
Simon R Maxwell BSc, MD, PhD, FRCP, FRCPE, FHEA
Professor of Pharmacology, Clinical Pharmacology Unit, University of Edinburgh, UK
David A McAllister MSc, MD, MRCP, MFPH
Wellcome Trust Intermediate Clinical Fellow and Beit Fellow, Senior Clinical Lecturer in Epidemiology, and Honorary Consultant in Public Health Medicine, University of Glasgow, UK
Rory J McCrimmon MD, FRCPE
Reader, Medical Research Institute, University of Dundee, UK Mairi McLean MRCP, PhD
Senior Clinical Lecturer in Gastroenterology, School of Medicine, Medical Sciences and Nutrition, University of Aberdeen; Honorary Consultant Gastroenterologist, Aberdeen Royal Infirmary, UK
Francesca EM Neuberger MRCP(UK)
Consultant Physician in Acute Medicine and Obstetric Medicine, Southmead Hospital, Bristol, UK
David E Newby BA, BSc(Hons), PhD, BM DM DSc, FMedSci, FRSE, FESC, FACC
British Heart Foundation John Wheatley Professor of Cardiology, British Heart Foundation Centre for Cardiovascular Science, University of Edinburgh, UK John DC Newell- Price MA, PhD, FRCP
Reader in Endocrinology, Department of Human Metabolism, University of Sheffield, UK
John Olson MD, FRPCE, FRCOphth
Consultant Ophthalmic Physician, Aberdeen Royal Infirmary; Honorary Reader, University of Aberdeen, UK
Ewan R Pearson PhD, FRCPE
Clinical Reader, Medical Research Institute, University of Dundee, UK Paul J Phelan BAO, MD, FRCPE
Consultant Nephrologist and Renal Transplant Physician, Royal Infirmary of Edinburgh; Honorary Senior Lecturer, University of Edinburgh, UK
Stuart H Ralston MRCP, FMedSci, FRSE
Arthritis Research UK Professor of Rheumatology, University of Edinburgh;
Honorary Consultant Rheumatologist, Western General Hospital, Edinburgh, UK
Peter T Reid MD, FRCPE
Consultant Physician, Respiratory Medicine, Lothian University Hospitals, Edinburgh, UK
Jonathan AT Sandoe PhD, FRCPath
Associate Clinical Professor, University of Leeds, UK Gordon R Scott BSc, FRCP
Consultant in Genitourinary Medicine, Chalmers Sexual Health Centre, Edinburgh, UK
Alan G Shand MD, FRCPE
Consultant Gastroenterologist, Western General Hospital, Edinburgh, UK Robby M Steel MA, MD, FRCPsych
Consultant Liaison Psychiatrist, Department of Psychological Medicine, Royal Infirmary of Edinburgh; Honorary (Clinical) Senior Lecturer, Department of Psychiatry, University of Edinburgh, UK
Grant D Stewart BSc(Hons), FRCSE(Urol), PhD
University Lecturer in Urological Surgery, Academic Urology Group, University of Cambridge; Honorary Consultant Urological Surgeon, Department of Urology, Addenbrooke’s Hospital, Cambridge; Honorary Senior Clinical Lecturer, University of Edinburgh, UK
Peter Stewart MBBS, FRACP, FRCPA, MBA
Associate Professor in Chemical Pathology, University of Sydney; Area Director of Clinical Biochemistry and Head of the Biochemistry Department, Royal Prince Alfred and Liverpool Hospitals, Sydney, Australia
Mark WJ Strachan BSc(Hons), MD, FRCPE
Consultant Endocrinologist, Metabolic Unit, Western General Hospital, Edinburgh; Honorary Professor, University of Edinburgh, UK
David R Sullivan MBBS, FRACP, FRCPA, FCSANZ
Clinical Associate Professor, Faculty of Medicine, University of Sydney;
Physician and Chemical Pathologist, Department of Clinical Biochemistry Royal Prince Alfred Hospital, Sydney, Australia
Shyam Sundar MD, FRCP(London), FAMS, FNASc, FASc, FNA Professor of Medicine, Institute of Medical Sciences, Banaras Hindu University, Varanasi, India
Victoria R Tallentire BSc(Hons), DipMedEd, MRCP, MD
Consultant Physician, Western General Hospital, Edinburgh; Honorary Senior Lecturer, University of Edinburgh, UK
Katrina Tatton- Brown BA, MD, FRCP(Paeds)
Consultant and Reader in Clinical Genetics and Genomic Education, South West Thames Regional Genetics Service, St George’s Universities Hospital NHS Foundation Trust, London, UK
Simon HL Thomas MD, FRCP, FRCPE
Professor of Cellular Medicine, Institute of Cellular Medicine, Newcastle University, Newcastle upon Tyne, UK
Henry G Watson MD, FRCPE, FRCPath
Consultant Haematologist, Aberdeen Royal Infirmary, UK Julian White MB, BS, MD, FACTM
Head of Toxinology, Women’s and Children’s Hospital, North Adelaide;
Professor, University of Adelaide, Australia John PH Wilding DM, FRCP
Professor of Medicine, Obesity and Endocrinology, University of Liverpool, UK Miles D Witham PhD, FRCPE
Clinical Senior Lecturer in Ageing and Health, University of Dundee, UK
List of abbreviations
ABGs arterial blood gases ACE angiotensin- converting
enzyme
ACTH adrenocorticotrophic hormone
ADH antidiuretic hormone AIDS acquired immuno-
deficiency syndrome ANA antinuclear antibody ANCA antineutrophil
cytoplasmic autoantibody ANF antinuclear factor ANP atrial natriuretic peptide APECED Autoimmune
polyendocrinopathy- candidiasis-ectodermal dystrophy
APS Antiphospholipid syndrome APTT activated partial
thromboplastin time ARDS acute respiratory
distress syndrome ASO antistreptolysin O AST aspartate
aminotransferase AXR abdominal X- ray BCG Calmette–Guérin
bacillus BMI body mass index BP blood pressure CK creatine kinase CNS central nervous system CPAP continuous positive
airways pressure CRH corticotrophin-
releasing hormone
CRP C- reactive protein CSF cerebrospinal fluid CT computed tomo-
graphy/tomogram CVP central venous
pressure CXR chest X- ray DEXA dual- energy X- ray
absorptiometry DIC disseminated intra-
vascular coagulation DIDMOAD diabetes insipidus,
diabetes mellitus, optic atrophy, deafness dsDNA double- stranded
deoxyribonucleic acid DVT deep venous
thrombosis ECG electrocardiography/
electrocardiogram ELISA enzyme- linked
immuno sorbent assay ERCP endoscopic retrograde
cholangiopancreat- ography
ESR erythrocyte sedimenta- tion rate
FBC full blood count FDA Food and Drug Admin-
istration FEV1/FVC forced expiratory
volume in 1 sec/forced vital capacity
FFP fresh frozen plasma 5- HT 5- hydroxytryptamine;
serotonin FOB faecal occult blood GI gastrointestinal
List of abbreviations
GMC General Medical Council GU genitourinary
HDL high- density lipoprotein HDU high- dependency unit HIV human immuno-
deficiency virus HLA human leucocyte
antigen
HRT hormone replacement therapy
ICU intensive care unit IL interleukin IM intramuscular INR International Normalised
Ratio IV intravenous
IVU intravenous urogram/
urography JVP jugular venous
pressure
LDH lactate dehydrogenase LDL low- density lipoprotein LFTs liver function tests MRA magnetic resonance
angiography MRC Medical Research
Council
MRCP magnetic resonance cholangiopancreat- ography
MRI magnetic resonance imaging
MRSA meticillin- resistant Staphylococcus aureus
MSU mid- stream sample of urine
NG nasogastric NICE National Institute
for Health and Care Excellence NIV non- invasive
ventilation NSAID non- steroidal anti-
inflammatory drug PA postero- anterior PCR polymerase chain
reaction
PE pulmonary embolism PET positron emission
tomography PTH parathyroid hormone RBC red blood count RCT randomised controlled
clinical trial SPECT single- photon
emission computed tomography STI sexually transmitted
infection TB tuberculosis TFTs thyroid function tests TNF tumour necrosis factor U&Es urea and electrolytes USS ultrasound scan VTE venous
thromboembolism WBC/WCC white blood/cell count WHO World Health
Organization
Picture credits
We are grateful to the following individuals and organisations for permis- sion to reproduce the figures and boxes listed below.
Chapter 5
Clinical examination of patients with infectious disease (p. 99) Splinter haemorrhages inset: Dr Nick Beeching, Royal Liverpool Univer- sity; Roth’s spots inset: Prof. Ian Rennie, Royal Hallamshire Hospital, Sheffield. Fig. 5.11 Malaria retinopathy inset: Dr Nicholas Beare, Royal Liverpool University Hospital; blood films insets, P. vivax and P. falciparum:
Dr Kamolrat Silamut, Mahidol Oxford Research Unit, Bangkok, Thailand.
Box 5.20 WHO. Severe falciparum malaria. In: Severe and complicated malaria. 3rd edn. Trans Roy Soc Trop Med Hyg 2000; 94 (suppl. 1): S1–41 Chapter 6
Fig. 6.3 Adapted from Flenley D. Lancet 1971; 1: 1921 Chapter 7
Clinical examination of the kidney and urinary tract (p. 207) Chapter 8
Clinical examination of the cardiovascular system (p. 249) Splinter haemorrhage, jugular venous pulse, malar flush and tendon xanthomas insets: Newby D, Grubb N. Cardiology: An Illustrated Colour Text. Edin- burgh: Churchill Livingstone; 2005. Fig. 8.4 Resuscitation Council (UK).
Fig. 8.18 NICE Clinical Guideline 127, Hypertension; August 2011) Box 8.7 European Society of Cardiology Clinical Practice Guidelines: Atrial Fibrillation (Management of) 2010 and Focused Update (2012). Eur Heart J 2012; 33: 2719–2747
Chapter 9
Clinical examination of the respiratory system (p. 311) Idiopathic kyphoscoliosis inset: Dr I. Smith, Papworth Hospital, Cambridge. Fig. 9.8 Adapted from Detterbeck FC, Boffa DJ, Tanoue LT. The new lung cancer staging system. Chest 2009; 136:260–271). Fig. 9.9 Johnson N McL.
Respiratory Medicine. Oxford: Blackwell Science; 1986 Chapter 10
Fig. 10.3 Toxic multinodular goitre inset: Dr P.L. Padfield, Western General Hospital, Edinburgh
Chapter 12
Fig. 12.3 Hayes P, Simpson K. Gastroenterology and Liver Disease.
Edinburgh: Churchill Livingstone; 1995 Chapter 13
Clinical examination of the abdomen for liver and biliary disease (p. 509) Spider naevi inset: Hayes P, Simpson K. Gastroenterology and liver disease. Edinburgh: Churchill Livingstone; 1995. Aspiration inset:
Strachan M. Davidson’s clinical cases. Edinburgh: Churchill Livingstone;
2008 (Fig. 65.1). Palmar erythema inset: Martin P. Approach to the patient with liver disease. In: Gold L and Schafter AI. Goldman’s Cecil Medicine.
24th edn. Philadelphia: WB Saunders; 2012 (Fig. 1148- 2, p. 954) Chapter 14
Blood disease Box 14.6 From Wells PS. New Engl J Med 2003; 349:
1227; copyright © 2003 Massachusetts Medical Society Chapter 16
Fig. 16.7 Courtesy of Dr B Cullen. Fig. 16.10 Courtesy of Dr A. Farrell and Professor J. Wardlaw
Chapter 18
Skin disease Fig. 18.13 White GM, Cox NH. Diseases of the skin.
London: Mosby; 2000; copyright Elsevier Chapter 19
Comprehensive geriatric assessment (p. 775) Wasted hand and kyphosis insets: Afzal Mir M. Atlas of Clinical Diagnosis. 2nd edn.
Edinburgh: Saunders; 2003. Box 19.5 Hodkinson HM, Evaluation of a mental test score for assessment of mental impairment in the elderly Age and Ageing 1972; 1(4): 233–238
Chapter 20
Clinical examination of the cancer patient (p. 785)
This page intentionally left blank
How doctors think, reason and make decisions is arguably their most critical skill.
Knowledge is necessary, but not sufficient, for good safe care.
The problem of diagnostic error
It is estimated that the diagnosis is wrong in 10% to 15% of cases in many specialties, causing much preventable morbidity.
Diagnostic error has been defined as ‘a situation in which the clinician has all the information necessary to make the diagnosis but then makes the wrong diagnosis’. Root causes include:
• No fault—for example, rare or atypical presentation.
• System error—for example, results not available, poorly trained staff.
• Human cognitive error—for example, inadequate data gathering, errors in reasoning.
Clinical reasoning
‘Clinical reasoning’ describes the thinking and decision- making processes associated with clinical practice. Errors may occur because of lack of knowledge, misinterpretation of diagnostic tests and cognitive bias (e.g.
accepting another’s diagnosis unquestioningly). Other key elements include patient- centred evidence- based medicine and shared decision making with patients and/or carers.
Clinical skills and decision making
Despite diagnostic technology, the history remains crucial; studies show that physicians make a diagnosis in 70% to 90% of cases from the history alone.
Additional knowledge is needed for correct interpretation of the history and examination. For example, students learn that meningitis presents with headache, fever and meningism (photophobia, nuchal rigidity). However, the frequency with which patients present with particular features and the diagnostic weight of each feature are important in clinical reasoning.
The likelihood ratio (LR) is the probability of a finding in someone with a disease (judged by a diagnostic standard, e.g. lumbar puncture in menin- gism) divided by the probability of that finding in someone without disease.
1
Clinical decision making
An LR greater than 1 increases the probability of disease; an LR of less than 1 reduces that probability. For example, in a person presenting with headache and fever, the clinical finding of nuchal rigidity (neck stiffness) may carry little diagnostic weight, because many patients with meningitis do not have classical signs of meningism (LR of around 1).
LRs do not determine the prior probability of disease, only how a single clinical finding changes it. Clinicians have to take all available information from the history and physical examination into account. If the prior prob- ability is high, a clinical finding with an LR of 1 does not change this.
‘Evidence- based history and examination’ is a term used to describe how clinicians incorporate knowledge about the prevalence and diagnostic weight of clinical findings into the history and physical examination.
Use and interpretation of diagnostic tests
No diagnostic test is perfect. To correctly interpret test results requires understanding of the following factors:
Normal values
Many quantitative measurements in populations have a Gaussian or
‘normal’ distribution, in which the normal range is defined as that which includes 95% of the population (±2 SD around the mean). Because 2.5% of the normal population will be above, and 2.5% below the range, it is better described as the ‘reference range’ rather than the ‘normal range’.
Results in abnormal populations also have a Gaussian distribution, with a different mean and standard deviation, although sometimes there is overlap with the reference range. The greater the difference between the result and the limits of the reference range, the higher the chance of disease.
Clinical context can affect interpretation. For example, a normal PaCO2 in the context of a severe asthma attack indicates life- threatening asthma.
A low ferritin level in a young menstruating woman is not considered to be pathological.
Factors other than disease that influence results
These include:
• age • ethnicity • pregnancy • sex • technical factors (e.g., high K+ in haemolysed sample).
Operating characteristics
Tests may be affected or rendered nondiagnostic by: • Patient motivation and technique (e.g. spirometry) • Operator skill • Patient’s body habitus and clinical state (e.g. echocardiography) • Paroxysmal illness (e.g. nor- mal EEG between fits in epilepsy) • The incidental discovery of a benign abnormality
Test results should always be interpreted in the light of the patient’s his- tory and examination.
1
Sensitivity and specificity
Sensitivity is the ability to detect true positives; specificity is the ability to detect true negatives. Even a very good test with 95% sensitivity will miss 1 in 20 people with the disease. Every test therefore has ‘false positives’ and
‘false negatives’ (Box 1.1).
A very sensitive test detects most cases of disease but generates abnor- mal findings in healthy people. A negative result reliably excludes disease, but a positive result does not mean disease is present. Conversely, a very specific test may miss significant pathology, but can firmly establish the diagnosis if positive. Clinicians need to know the sensitivity and specificity of the tests they use.
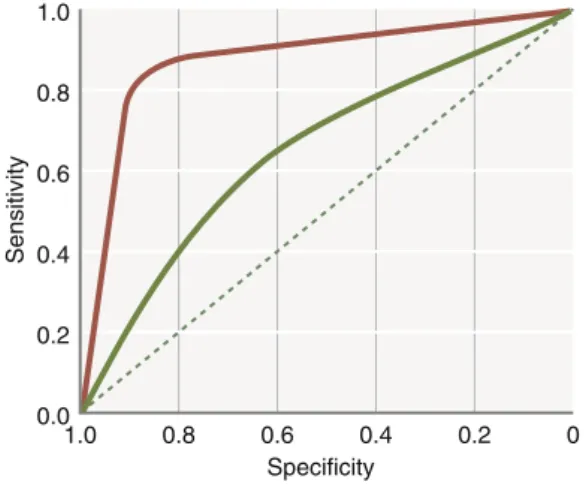
In choosing how a test is used, there is a trade- off between sensitivity and specificity. This is illustrated by the receiver operating characteristic curve of the test (Fig. 1.1).
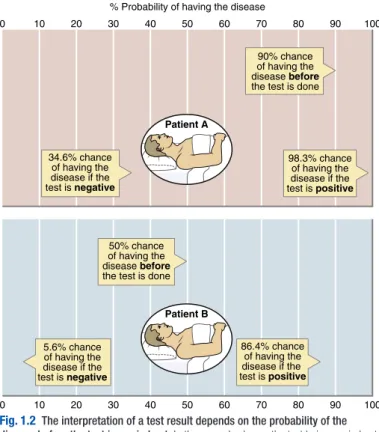
An extremely important concept is this: the probability that a person has a disease depends on both the pretest probability and the sensitivity and specificity of the test. In a patient whose history suggests a high pretest probability of disease, a normal test result does not exclude the condition, but in a low- probability patient, it makes it very unlikely. This principle is illustrated in Fig. 1.2.
Prevalence of disease
The prevalence of disease in the patient’s population subgroup should inform the doctor’s estimate of pretest probability. Prevalence also influences the chance that a positive test result indicates disease.
Consider a test with a false- positive rate of 5% for a disease whose prevalence is 1:1000. If 1000 people are tested, there will be 51 posi- tive results: 50 false positives and one true positive. The chance that a person found to have a positive result actually has the disease is only 1/51, or 2%.
Predictive values combine sensitivity, specificity and prevalence, allow- ing doctors to address the question: ‘What is the probability that a per- son with a positive test actually has the disease?’. This is illustrated in Box 1.2.
1.1 Sensitivity and specificity
Disease No disease
Positive test A B
(True positive) (False positive)
Negative test C D
(False negative) (True negative) Sensitivity = A/(A+C) × 100
Specificity = D/(D+B) × 100
Dealing with uncertainty
Clinicians must frequently deal with uncertainty. By expressing uncertainty as probability, new information from diagnostic tests can be incorporated more accurately. However, intuition and subjective estimates of probability can be unreliable.
Knowing the patient’s true state is often unnecessary in clinical deci- sion making. The requirement for diagnostic certainty depends on the pen- alty for being wrong. Different situations require different levels of certainty before starting treatment. How we communicate uncertainty to patients will be discussed later in this chapter (p. 8).
The treatment threshold combines factors such as the risks of the test and the risks versus benefits of treatment. A less effective or high risk test increases the treatment threshold.
Cognitive biases
Human thinking and decision making are prone to error. Cognitive biases are subconscious errors that lead to inaccurate judgement and illogical interpretation of information.
Humans have two distinct types of processes when it comes to thinking and decision making: type 1 and type 2 thinking.
1.0 0.8 0.6 0.4 0.2
0.01.0 0.8 0.6 Specificity
0.4 0.2 0
Sensitivity
Fig. 1.1 Receiver operating characteristic graph illustrating the trade- off between sensitivity and specificity for a given test. The curve is generated by
‘adjusting’ the cut- off values defining normal and abnormal results, calculating the effect on sensitivity and specificity and then plotting these against each other. The closer the curve lies to the top left- hand corner, the more useful the test. The red line illustrates a test with useful discriminant value, and the green line illustrates a less useful, poorly discriminant test.
1
Type 1 and type 2 thinking
Cognitive psychology identifies two distinct processes when it comes to decision making: intuitive (type 1) and analytical (type 2). This has been termed ‘dual process theory’. Box 1.3 explains this in more detail.
Psychologists estimate that we spend 95% of our daily lives engaged in type 1 thinking—the intuitive, fast, subconscious mode of decision making.
Learning to drive involves moving from the deliberate, conscious, slow and effortful first lesson to the automatic, fast and effortless process of an expe- rienced driver. The same applies to medical practice, and intuitive thinking is highly efficient in many circumstances; however, in others it is prone to error.
Patient A
90% chance of having the disease before the test is done
34.6% chance of having the disease if the test is negative
0 10 20 30 40 50
% Probability of having the disease
60 70 80 90 100
0 10 20 30 40 50 60 70 80 90 100
98.3% chance of having the disease if the test is positive
Patient B 50% chance of having the disease before the test is done
86.4% chance of having the disease if the test is positive 5.6% chance
of having the disease if the test is negative
Fig. 1.2 The interpretation of a test result depends on the probability of the disease before the test is carried out. In the example shown, the test being carried out has a sensitivity of 95% and a specificity of 85%. Patient A has very characteristic clinical findings, which make the pretest probability of the condition for which the test is being used very high—estimated as 90%. Patient B has more equivocal findings, such that the pretest probability is estimated as only 50%. If the result in Patient A is negative, there is still a significant chance that he has the condition for which he is being tested; in Patient B, however, a negative result makes the diagnosis very unlikely.
Clinicians use both type 1 and type 2 thinking. When encountering a familiar problem, clinicians employ pattern recognition and reach a differ- ential diagnosis quickly (type 1 thinking). When encountering a problem that is more complicated, they use a slower, systematic approach (type 2 thinking). Both types of thinking interplay—they are not mutually exclusive in the diagnostic process. Errors can occur in both type 1 and type 2 think- ing; for example, people can apply the wrong rules or make errors in their application while using type 2 thinking. However, it has been argued that the common cognitive biases encountered in medicine tend to occur when clinicians are engaged in type 1 thinking.
Common cognitive biases in medicine
These include:
• Overconfidence bias—the tendency to believe we know more than we actually do • Availability bias—the likelihood of diagnosing recently seen conditions • Ascertainment bias—seeing what we expect to see • Confir- mation bias—only looking for evidence to support a theory, not to refute it
1.2 Predictive values: ‘What is the probability that a person with a positive test actually has the disease?’
Disease No disease
Positive test A B
(True positive) (False positive)
Negative test C D
(False negative) (True negative) Positive predictive value = A/(A+B) × 100
Negative predictive value = D/(D+C) × 100
1.3 Type 1 and type 2 thinking
Type 1 Type 2
Intuitive, heuristic (pattern recognition) Analytical, systematic
Automatic, subconscious Deliberate, conscious
Fast, effortless Slow, effortful
Low/variable reliability High/consistent reliability
Vulnerable to error Less prone to error
Highly affected by context Less affected by context High emotional involvement Low emotional involvement
Low scientific rigour High scientific rigour
• Commission bias—the assumption that doing something is better than
1
waiting • Omission bias—the belief that doing nothing is better rather than causing harm.
The mark of a well- calibrated thinker is the ability to recognise what mode of thinking is being employed and to anticipate and recognise situations in which cognitive biases and errors are more likely to occur.
Human factors
The science of ‘human factors’ is the study of the limitations of human performance, and how technology, the work environment and team com- munication can adapt for this to reduce diagnostic and other types of error.
For example, performance is adversely affected by factors such as poorly designed processes and equipment, frequent interruptions and fatigue.
The areas of the brain required for type 2 processing are most affected by things like fatigue and cognitive overload, and the brain reverts to type 1 processing to conserve cognitive energy.
In focusing on what we are trying to see to filter out distractions, we may not notice the unexpected. In a team context, what is obvious to one person may be completely missed by someone else. Safe and effective team communication therefore requires us to never assume and to verbal- ise things, even though they may seem obvious.
Reducing errors in clinical decision making
Knowledge and experience do not eliminate errors. Instead, there are a number of ways in which we can act to reduce errors in clinical decision making. Examples are:
• Adopting ‘cognitive debiasing strategies’.
• Using clinical prediction rules and other decision aids.
• Engaging in effective team communication.
Cognitive debiasing strategies
There are some simple and established techniques that can be used to avoid cognitive biases and errors in clinical decision making.
History and physical examination
A thorough history and physical examination are essential, and bias and error will result if these are carried out inadequately.
Problem lists and differential diagnosis
The ability to identify key clinical data and create a problem list is a key step in clinical reasoning. Some problems (e.g. low serum potassium) require action, but not necessarily a differential diagnosis. Other problems (e.g.
vomiting) require a differential diagnosis. The process of generating a prob- lem list ensures nothing is missed and helps avoid anchoring on a particular diagnosis too early.
Mnemonics and checklists
These are used frequently in medicine to reduce reliance on fallible human memory. ABCDE (airway, breathing, circulation, disability, exposure/exami- nation; sometimes prefixed with ‘C’ for ‘control of any obvious problem’) is probably the most successful checklist in medicine, and is commonly used during stressful assessment of critically ill patients.
Red flags and ROWS (rule out worst case scenario)
These are strategies that force doctors to consider serious diseases that can present with common symptoms. Red flags in back pain are listed in (Box 15.3, p. 597). Considering and investigating for possible pulmonary embolism in patients who present with pleuritic chest pain and breathless- ness is a common example of ruling out a worst- case scenario, as pulmo- nary embolism can be fatal if missed.
Using clinical prediction rules and other decision aids
Clinical prediction rules use the patient’s symptoms, signs and other data to determine the numerical probability of a disease or an outcome. They only work for the population used to create the rule.
Commonly used examples include the Wells score in suspected deep vein thrombosis (see Box 4.7, p. 71), the GRACE score in acute coronary syndromes (see Box 8.12, p. 284) and the CURB- 65 score in community- acquired pneumonia (see Fig 9.6, p. 335).
Patient- centred evidence- based medicine and shared decision making
This requires the application of best- available research evidence while tak- ing individual patient factors into account, including both clinical and non- clinical factors (e.g. the patient’s social circumstances, values and wishes).
As this chapter has described, clinicians frequently deal with uncertainty/
probability. Clinicians need to be able to explain the risks and benefits of treatment accurately and understandably. Providing the relevant statistics is seldom sufficient, because a patient’s perception of risk may be influenced by irrational factors and individual values.
Avoid nebulous terms such as ‘common’ and ‘rare’. Whenever possible, clinicians should quote numerical information using consistent denomina- tors (e.g. ‘90 out of 100 patients who have this operation feel much better, one will die during the operation and two will suffer a stroke’). Visual aids can be used to present complex statistical information (Fig. 1.3).
Studies demonstrate a correlation between effective clinician–patient communication and improved health outcomes. If patients feel they have been listened to and understand the problem and proposed treatment plan, they are more likely to follow the plan and less likely to re- attend.
1
Feel better No difference Stroke Dead
Fig. 1.3 Visual portrayal of benefits and risks. The image refers to an operation that is expected to relieve symptoms in 90% of patients, but cause stroke in 2% and death in 1%. (From Edwards A, Elwyn G, Mulley A. Explaining risks: turning numerical data into meaningful pictures. BMJ 2002; 324:827–830. With permission from the BMJ Publishing Group.)
This page intentionally left blank
Prescribing medicines is the major tool used by doctors to restore or preserve the health of patients. Therapeutic benefits must be weighed against cost, adverse effects and interactions. Harm can also result from injudicious prescribing decisions and prescribing errors. The increasing number of available drugs and treatment indications, together with the complexity of individual treatment regimens (‘polypharmacy’), are challenging for the modern prescriber. This chapter outlines the principles and practice of good prescribing (Box 2.1).
Principles of clinical pharmacology
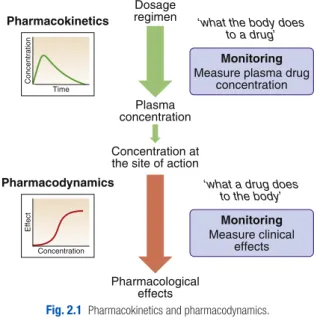
Prescribers need to understand what the drug does to the body (pharmaco- dynamics) and what the body does to the drug (pharmacokinetics, Fig. 2.1).
Most drugs are synthetic small molecules, but the same principles apply to
‘biological’ therapies, including peptides, proteins and monoclonal antibodies.
2
Clinical therapeutics and prescribing
2.1 Steps in good prescribing • Make a diagnosis
• Consider factors that might influence the patient’s response to therapy (age, con- comitant drug therapy, renal and liver function etc.)
• Establish the therapeutic goala • Choose the therapeutic approacha
• Choose the drug and its formulation (the ‘medicine’) • Choose the dose, route and frequency
• Choose the duration of therapy
• Write an unambiguous prescription (or ‘medication order’) • Inform the patient about the treatment and its likely effects • Monitor treatment effects, both beneficial and harmful • Review/alter the prescription
aThese steps in particular take the patient’s views into consideration, thereby establishing a therapeutic partnership (shared decision making to achieve ‘concordance’).
Pharmacodynamics
Drug targets and mechanisms of action
Drugs usually either stimulate or block the function of a specific molecu- lar target relevant to a particular disease (Box 2.2). Other drugs have less selective chemical properties, such as chelators (e.g. for iron overload), osmotic agents (for cerebral oedema) or general anaesthetics (which alter the biophysical properties of membranes). The interaction of drugs with receptors depends on:
• Affinity: how well the drug binds to a receptor, reflecting the ‘molecular fit’ and the strength of the bond. Some such interactions are irreversible, attributed to a strong affinity or because the drug modifies its target.
• Selectivity: how well the drug binds to one target relative to another.
Drugs that target one receptor subtype commonly also affect other subtypes. For example, ‘cardioselective’ β- blockers have antianginal effects (β1), but may also cause bronchospasm (β2).
• Agonists bind to receptors, producing a response proportional to the agonist concentration and the proportion of receptors occupied.
Partial agonists cannot produce a maximal response, even when all receptors are occupied.
• Antagonists bind to a receptor without initiating a response. Competi- tive antagonists compete with endogenous ligands to occupy recep- tors, and their potency depends on the relative affinities and concen- trations of drug and ligand. Noncompetitive antagonists inhibit agonist effects by affecting other mechanisms (e.g. postreceptor signalling).
Dosage regimen
Plasma concentration Concentration at the site of action
Pharmacological effects
Pharmacokinetics ‘what the body does to a drug’
Monitoring Measure plasma drug
concentration
‘what a drug does to the body’
Monitoring Measure clinical
effects
Concentration Time
Pharmacodynamics
Concentration
Effect
Fig. 2.1 Pharmacokinetics and pharmacodynamics.
2
Dose–response relationships
Plotting the logarithm of drug dose against drug response typically pro- duces a sigmoidal dose–response curve (Fig. 2.2). Increases in dose produce increasing responses, but only within a particular range; further increases produce little extra effect. Drug responses are characterised by:
• Efficacy: the extent to which a drug produces a specific response when all available receptors are occupied. Efficacy is maximal for a full agonist; a partial agonist at the same receptor shows lower efficacy.
• Therapeutic efficacy: the effect of the drug on a desired biological end- point. Used to compare drugs acting via different mechanisms (e.g.
diuresis following loop diuretics versus thiazides).
• Potency: the amount of drug required for a given response. More potent drugs act at lower doses.
2.2 Examples of target molecules for drugs
Drug target Description Examples
Receptors Channel- linked receptors
Ligand binding controls a
‘ligand- gated’ ion channel
Nicotinic acetylcholine receptor
GPCRs Ligand binding affects a ‘G-
protein’ that mediates signal transduction
β- adrenoceptors Opioid receptors Kinase- linked receptors Ligand binding activates
intracellular protein kinase, triggering phosphorylation
Insulin receptor Cytokine receptors Transcription factor
receptors Intracellular; ligand binding promotes or inhibits gene transcription
Steroid receptors Retinoid receptors Other targets
Voltage- gated ion
channels Mediate electrical signalling in
muscle and nervous system Na+ and Ca2+ channels
Enzymes Catalyse biochemical
reactions; drugs interfere with binding of substrate
ACE
Xanthine oxidase Transporter proteins Carry ions or molecules across
cell membranes Na+/K+ ATPase Cytokines/other
signalling molecules Small proteins that are important in cell signalling, especially immune responses
Tumour necrosis factors Interleukins
Cell surface antigens Block recognition of cell
surface molecules CD20, CD80
ACE, Angiotensin-converting enzyme; GPCR, G-protein-coupled receptor.
The dose–response relationship varies between patients because of variations in pharmacokinetics and pharmacodynamics. The prescriber cannot know the dose–response curve for individuals, so most drugs are licensed within a dose range predicted to reach close to the top of the dose–response curve in most patients.
Therapeutic index
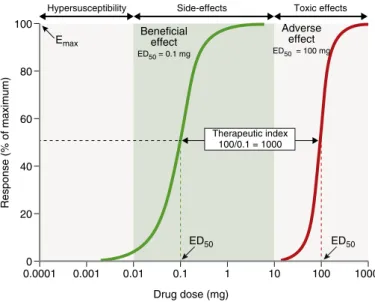
Adverse effects of drugs, like beneficial effects, are often dose- related, although the dose–response curve for adverse effects is shifted to the right (Fig. 2.2). The ratio of the dose effective in 50% of patients to the dose causing adverse effects in 50% is called the ‘therapeutic index’. Many drugs have multiple adverse effects, so the therapeutic index is usually based on those that require dose reduction or discontinuation. For most drugs, the therapeutic index is greater than 100, but some have therapeutic indices of less than 10 (e.g. digoxin, warfarin, insulin, phenytoin, opioids).
These must be titrated to maximise benefits while avoiding toxicity.
Desensitisation and withdrawal effects
Desensitisation means that the response to a drug diminishes with repeated dosing. Sometimes the response can be restored by increasing the dose;
however, the tissues may ultimately become completely refractory to the drug.
Hypersusceptibility Side-effects 100
80
60
40
20
0.00010 0.001 0.01 0.1 1 10 100 1000
Therapeutic index 100/0.1 = 1000
Drug dose (mg)
Response (% of maximum)
Toxic effects Adverse
effect ED50 = 100 mg Beneficial
effect ED50 = 0.1 mg Emax
ED50 ED50
Fig. 2.2 Dose–response curve. The green curve represents the beneficial effect of the drug. The dose or concentration producing half the maximum response (Emax/2) is the ED50 (or EC50). The red curve is the dose–response relationship for the key adverse effect, which occurs at higher doses. Adverse effects occurring above the therapeutic range are called ‘toxic effects’, whereas those occurring within the therapeutic range are ‘side effects’.
2
• Tachyphylaxis describes very rapid desensitisation, sometimes with the initial dose. This implies depletion of chemicals necessary for the drug to act (e.g. a stored neurotransmitter) or receptor phosphorylation.
• Tolerance describes a gradual loss of response over days to weeks.
This implies changes in receptor numbers or counter- regulatory physi- ological changes offsetting the drug’s effect.
• Drug resistance means the loss of effectiveness of an antimicrobial or chemotherapy drug.
• A reduced response may also be caused by lower drug concentra- tions as a result of altered pharmacokinetics (see later).
When drugs induce chemical, hormonal and physiological changes that offset their actions, discontinuation may cause ‘rebound’ withdrawal effects (Box 2.3).
2.3 Examples of drugs with withdrawal effects
Drug Symptoms Signs Treatment
Alcohol Anxiety, panic, paranoid delusions, visual and auditory hallucinations
Agitation, delirium, tremor, tachycardia, ataxia, disorientation, seizures
Treat immedi- ate withdrawal syndrome with benzodiazepines Barbiturates,
benzodiazepines Similar to alcohol Similar to alcohol Substitute long- acting benzodiaze- pine, then gradually wean off Glucocorticoids Weakness, fatigue,
anorexia, weight loss, nausea, vom- iting, diarrhoea, abdominal pain
Hypotension, hypoglycaemia
Prolonged therapy suppresses the HPA axis, causing ad- renal insufficiency;
gradual withdrawal required
Opioids Rhinorrhoea,
sneezing, yawn- ing, lacrimation, abdominal and leg cramps, nausea, vomiting, diarrhoea
Dilated pupils Transfer addicts to long- acting agonist methadone
SSRIs Dizziness, sweat-
ing, nausea, insomnia, tremor, delirium, night- mares
Tremor Reduce slowly to
avoid withdrawal effects
HPA, Hypothalamic pituitary adrenal; SSRI, selective serotonin reuptake inhibitor.
Pharmacokinetics
Understanding ‘what the body does to the drug’ allows the optimal admin- istration route and dose regimen to be chosen, and explains the majority of inter- individual variation in drug responses.
Drug absorption and routes of administration
How drug molecules access the blood stream depends on the route of administration (Fig. 2.3). ‘Bioavailability’ describes the proportion of the dose that reaches the systemic circulation.
Enteral (gastrointestinal) administration
• Oral: this is simple and convenient for patients, but the effect of an oral dose may be altered by ineffective swallowing, gastric acid, food binding, disease affecting intestinal absorption and by enteric or liver metabolism (‘first- pass metabolism’).
• Buccal, intranasal and sublingual: these routes allow rapid absorption into the systemic circulation, bypassing the complexities of oral admin- istration. Commonly used for nitrates in angina.
• Rectal: occasionally used when the oral route is compromised by nausea, vomiting or unconsciousness (e.g. diazepam in status epilepticus).
Interstitial fluid
Intracellular fluid
Kidney Liver
Parenteral Mouth
Stomach
Small intestine
Large intestine Rectum
Buccal
Excretion in urine
Excretion in faeces
Portal venous system Intestinal wall enzymes
Liver enzymes Metabolism
Circulating plasma
Rectal Oral
Fig. 2.3 Pharmacokinetics summary. Most drugs are taken orally, absorbed from the in- testine and conveyed to the liver by the portal system, where they may undergo first- pass metabolism and/or excretion in bile. The active drug then enters the systemic circulation, from which it may diffuse (or sometimes be actively transported) into the interstitial and intracellular fluid compartments. Drug in the plasma undergoes liver metabolism and renal excretion. Drugs excreted in bile may be reabsorbed, creating an enterohepatic circula- tion. First- pass metabolism in the liver is avoided if drugs are administered via the buccal or rectal mucosa, or by injection.
2
Parenteral administration
• Intravenous: this route enables the entire dose to enter the systemic circulation reliably, unaffected by absorption or first- pass metabolism.
It is ideal when a high plasma concentration is needed quickly (e.g.
benzylpenicillin for meningococcal meningitis).
• Intramuscular: easier than the IV route (e.g. adrenaline (epinephrine) for anaphylaxis), but absorption is less predictable.
• Subcutaneous: this is ideal for self- administered parenteral drugs (e.g.
insulin, heparin).
• Transdermal patches: these enable a drug to be absorbed through the skin into the circulation (e.g. oestrogens, nicotine, nitrates).
Other routes of administration
• Topical: direct administration to the site of action (e.g. skin, eye, ear).
Achieves sufficient concentration at this site while minimising systemic exposure and adverse effects.
• Inhaled: administration allows direct delivery to the airways (e.g. salbuta- mol, beclometasone). However, a significant proportion of the dose may be absorbed from the lung or swallowed and can reach the systemic circu- lation. Correct use of a metered- dose inhaler is difficult for many patients. A
‘spacer’ device or a breath- powered dry powder inhaler can improve drug delivery. Nebulisers use pressurised oxygen or air to generate an aerosol from liquid drug that can be inhaled directly with a mouthpiece or mask.
Drug distribution
Distribution is the process by which drug molecules move into and out of the blood. It is influenced by molecular size, lipid solubility, plasma protein binding, affinity for surface- bound drug transporters and binding to molecular targets and other cellular proteins. Most drugs diffuse passively from the plasma to the interstitial fluid until the concentrations equalise. As the plasma concentration falls through metabolism or excretion, the drug diffuses back from the intersti- tium into the blood and is eliminated, unless additional doses enter the plasma.
Volume of distribution, Vd
This is the volume into which a drug appears to have distributed following intravenous injection. It is calculated as follows:
Vd= Dose given / Intial plasma concentration
Drugs that bind to plasma proteins (e.g. warfarin) have a Vd below 10 L;
those that enter the interstitial fluid but not the cells (e.g. gentamicin) have a Vd of 10 to 30 L. Lipid- soluble and tissue- bound drugs (e.g. digoxin) may have a Vd of greater than 100 L. Drugs with a larger Vd have longer half- lives than those with a smaller Vd, and take longer to reach steady state on repeated administration.
Drug elimination Drug metabolism
Metabolism is the process by which drugs are altered from a lipid- soluble form suitable for absorption and distribution to a more water- soluble form that is necessary for excretion. Some drugs, known as ‘prodrugs’, are inac- tive when administered but are converted to an active metabolite in vivo.
Phase I metabolism most commonly involves oxidation by the cytochrome P450 family of enzymes in the endoplasmic reticulum of hepatocytes.
Phase II metabolism involves combining phase I metabolites with an endogenous substrate to form an inactive conjugate that is much more water- soluble, thereby enabling renal excretion.
Drug excretion
Renal excretion is the usual route of elimination for drug metabolites of low molecular weight that have sufficient water- solubility to avoid tubular reabsorption. Drugs bound to plasma proteins are not filtered by the glom- eruli. Urine is more acidic than plasma, so some drugs (e.g. salicylates) become un- ionised in the kidneys and tend to be reabsorbed. Alkalina- tion of the urine can hasten excretion (e.g. after a salicylate overdose). For other drugs (e.g. methotrexate, penicillin), active secretion into the proximal tubule lumen is the main mechanism of excretion.
Faecal excretion is the predominant route for drugs with high molecular weight, those that are excreted in the bile after hepatic glucuronide conju- gation and those that are not absorbed after enteral administration. After biliary excretion, some lipid- soluble drugs are reabsorbed in the small intes- tine, returning to the liver via the portal vein (‘enterohepatic circulation’), thus prolonging the residence of the drug in the body.
Elimination kinetics
The net removal of drug from the circulation by metabolism and excretion is described as ‘clearance’, that is, the volume of plasma that is completely cleared of drug per unit time.
For most drugs, elimination is a high capacity process that does not become saturated, so elimination is proportional to drug concentration.
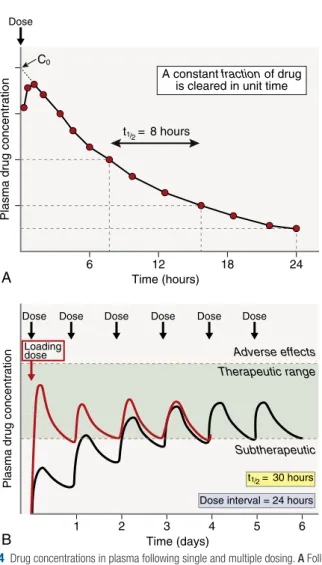
This results in ‘first- order’ kinetics, in which the time that it takes for the plasma drug concentration to halve (half- life, t1/2) is constant, causing an exponential decline in concentration (Fig. 2.4A). In this situation, a doubled dose leads to a doubled concentration at all time points.
For a few common drugs (e.g. phenytoin, alcohol), the elimination capac- ity is saturated within the usual dose range (‘zero- order’ kinetics). In this situation, if the rate of administration exceeds the maximum rate of elimina- tion, the drug accumulates progressively, with serious toxicity.
Repeated dose regimens
The goal of therapy is usually to maintain drug concentrations within the therapeutic range (see Fig. 2.2) over several days (e.g. antibiotics), or even for months or years (e.g. antihypertensives, lipid- lowering drugs). This requires the correct dose and frequency of administration.
As illustrated in Fig 2.4B, the time taken to reach therapeutic concentra- tions depends on the half- life of the drug. Typically, it takes approximately five half- lives to reach a steady state in which drug elimination equals drug administration, and drug concentrations stay within the therapeutic range.
This means the effects of a new dose of a drug with a long half- life (e.g.
digoxin, which has a half- life of 36 hours) may not be known for several days. In contrast, drugs with a short half- life (e.g. dobutamine) have to be given continuously by infusion but reach a steady state within minutes.
2
Time (hours)
A constant fraction of drug is cleared in unit time
t1/2 = 8 hours C0
Plasma drug concentration
6 12 18 24
A
B
Loading dose Dose Dose
Dose Dose Dose Dose Dose
Subtherapeutic
Dose interval = 24 hours Time (days)
Plasma drug concentration
1 2 3 4 5 6
Therapeutic range Adverse effects
t1/2 = 30 hours
Fig. 2.4 Drug concentrations in plasma following single and multiple dosing. A Following a single IV dose, the time required for the plasma drug concentration to halve (half- life, t1/2) is constant throughout the elimination process. B With multiple dosing, the peak, average and trough concentrations rise progressively if each dose is administered before the previous dose is entirely cleared (black line). For most of the first 3 days, drug concen- trations are below the therapeutic range. This can be overcome by using a larger loading dose (red line) to achieve a steady state more rapidly.
For drugs with a long half- life, a large initial ‘loading dose’ can be given to achieve a therapeutic concentration rapidly, which is then maintained by subsequent doses. A steady state actually involves fluctuations in drug concentrations, with peaks after administration and troughs before the next dose. Manufacturers recommend dosing regimens that create, for most patients, troughs inside the therapeutic range and peaks low enough to avoid adverse effects. The optimal dose interval is a compromise between patien