FOURTEENTH EDITION
EDITED BY
Ronald Sakaguchi, DDS, MS, PhD, MBA
Professor, Division of Management School of Medicine
Professor, Division of Biomaterials and Biomechanics Department of Restorative Dentistry
School of Dentistry
Oregon Health & Science University Portland, OR
Jack Ferracane, PhD
Professor and Chair, Department of Restorative Dentistry Division Director, Biomaterials and Biomechanics School of Dentistry
Oregon Health & Science University Portland, OR
John Powers, PhD
Senior Vice President, Dental Consultants, Inc.
(publisher of The Dental Advisor) Ann Arbor, MI
Clinical Professor of Oral Biomaterials
Department of Restorative Dentistry and Prosthodontics UTHealth School of Dentistry
The University of Texas Health Science Center at Houston Houston, TX
Craig’s
RESTORATIVE DENTAL
MATERIALS
CRAIG’S RESTORATIVE DENTAL MATERIALS,
FOURTEENTH EDITION ISBN: 978-0-323-47821-2
Copyright © 2019 by Elsevier, Inc. All rights reserved.
No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further infor- mation about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website:
www.elsevier.com/permissions.
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Notices
Knowledge and best practice in this field are constantly changing. As new research and experience broaden our understanding, changes in research methods, professional practices, or medical treat- ment may become necessary.
Practitioners and researchers must always rely on their own experience and knowledge in evalu- ating and using any information, methods, compounds, or experiments described herein. In using such information or methods they should be mindful of their own safety and the safety of others, including parties for whom they have a professional responsibility.
With respect to any drug or pharmaceutical products identified, readers are advised to check the most current information provided (i) on procedures featured or (ii) by the manufacturer of each product to be administered, to verify the recommended dose or formula, the method and duration of administration, and contraindications. It is the responsibility of practitioners, relying on their own experience and knowledge of their patients, to make diagnoses, to determine dosages and the best treatment for each individual patient, and to take all appropriate safety precautions.
To the fullest extent of the law, neither the Publisher nor the authors, contributors, or editors, assume any liability for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instruc- tions, or ideas contained in the material herein.
Previous editions copyrighted 2012, 2006, 2002, 1997, 1993, 1989, 1985, 1980, 1975, 1971, 1968, 1964, and 1960 by Mosby, Inc., an affiliate of Elsevier Inc.
Library of Congress Cataloging-in-Publication Data
Names: Sakaguchi, Ronald L., editor. | Ferracane, Jack L., editor. | Powers, John M., 1946- editor Title: Craig’s restorative dental materials / edited by Ronald Sakaguchi, Jack Ferracane, John Powers Other titles: Restorative dental materials
Description: Fourteenth edition. | St. Louis, Missouri : Elsevier, [2019] | Includes bibliographical references and index.
Identifiers: LCCN 2017051980 | ISBN 9780323478212 (pbk. : alk. paper) Subjects: | MESH: Dental Materials | Dental Atraumatic Restorative Treatment
Classification: LCC RK652.5 | NLM WU 190 | DDC 617.6/95--dc23 LC record available at https://lccn.loc.gov/2017051980
Senior Content Strategist: Jennifer Flynn-Briggs
Senior Content Development Specialist: Ann Ruzycka Anderson Publishing Services Manager: Catherine Jackson
Book Production Specialist: Kristine Feeherty Design Direction: Renee Duenow
Printed in China
Last digit is the print number: 9 8 7 6 5 4 3 2 1
Dr. Robert G. Craig, who passed away on April 24, 2003.
Following in the footsteps of the first editor, Dr. Floyd Peyton, Dr. Craig served as the lead editor of nine editions of this text. Dr. Craig was the Marcus L. Ward Professor Emeritus of Dentistry at the University of Michigan, where he had been on the faculty since 1957. He applied his background in chemistry and engineering to research problems in dental materials and contributed to the education of thousands of predoctoral, postgraduate, and graduate students. This text, which is now translated in numerous languages, reflects his commitment to the dissemination of accurate,
current knowledge about dental materials in clinical practice.
We also dedicate this text to the many mentors and colleagues with whom we have collaborated.
Ron Sakaguchi Jack Ferracane John Powers
v Roberto R. Braga, DDS, MS, PhD
Professor
Department of Biomaterials and Oral Biology School of Dentistry
University of São Paulo São Paulo, Brazil
Chapter 5: Testing of Dental Materials and Biomechanics Chapter 13: Materials for Adhesion and Luting
Isabelle L. Denry, DDS, PhD Professor
Department of Prosthodontics and Dows Institute for Oral Health Research
The University of Iowa College of Dentistry Iowa City, IA
Chapter 11: Restorative Materials: Ceramics Jack L. Ferracane, PhD
Professor and Chair
Department of Restorative Dentistry Division Director
Biomaterials and Biomechanics School of Dentistry
Oregon Health & Science University Portland, OR
Chapter 3: Materials-Centered Treatment Design Chapter 6: Biocompatibility and Tissue Reaction to
Biomaterials
Chapter 8: Preventive and Intermediary Materials Chapter 10: Restorative Materials: Metals Sharukh S. Khajotia, BDS, MS, PhD Associate Dean for Research
University of Oklahoma College of Dentistry University of Oklahoma Health Sciences Center Oklahoma City, OK
Chapter 2: The Oral Environment David B. Mahler, PhD† Professor Emeritus
Division of Biomaterials and Biomechanics Department of Restorative Dentistry School of Dentistry
Oregon Health & Science University Portland, OR
Chapter 10: Restorative Materials: Metals
Grayson W. Marshall Jr., DDS, MPH, PhD, Odont.
Dr. h.c. (Malmö)
Distinguished Professor Emeritus and Professor (Recalled)
Division of Biomaterials and Bioengineering Department of Preventive and Restorative Dental
Sciences
University of California San Francisco San Francisco, CA
Chapter 2: The Oral Environment Sally J. Marshall, PhD
Distinguished Professor Emerita and Professor (Recalled)
Division of Biomaterials and Bioengineering Department of Preventive and Restorative Dental
Sciences
University of California San Francisco San Francisco, CA
Chapter 2: The Oral Environment John C. Mitchell, PhD
Professor and Assistant Dean for Research Midwestern University
College of Dental Medicine Glendale, AZ
Chapter 6: Biocompatibility and Tissue Reaction to Biomaterials
Chapter 15: Dental and Orofacial Implants Chapter 16: Tissue Engineering
Sumita B. Mitra, PhD
Corporate Scientist 3M Company (retired) St. Paul, MN
Partner
Mitra Chemical Consulting, LLC West St. Paul, MN
Chapter 9: Restorative Materials: Resin Composites and Polymers
Chapter 13: Materials for Adhesion and Luting Carmem S. Pfeifer, DDS, PhD
Associate Professor
Division of Biomaterials and Biomechanics Department of Restorative Dentistry School of Dentistry
Oregon Health & Science University Portland, OR
Chapter 4: Fundamentals of Materials Science
Chapter 5: Testing of Dental Materials and Biomechanics
Contributors
†Deceased.
John M. Powers, PhD Senior Vice President
Dental Consultants, Inc. (publisher of The Dental Advisor)
Ann Arbor, MI
Clinical Professor of Oral Biomaterials Department of Restorative Dentistry and
Prosthodontics
UTHealth School of Dentistry
The University of Texas Health Science Center at Houston
Houston, TX
Chapter 12: Replicating Materials: Impression and Casting
Chapter 14: Digital Imaging and Processing for Restorations
Ronald L. Sakaguchi, DDS, MS, PhD, MBA Professor
Division of Management School of Medicine Professor
Division of Biomaterials and Biomechanics Department of Restorative Dentistry School of Dentistry
Oregon Health & Science University Portland, OR
Chapter 1: Role and Significance of Restorative Dental Materials
Chapter 3: Materials-Centered Treatment Design Chapter 4: Fundamentals of Materials Science
Chapter 5: Testing of Dental Materials and Biomechanics Chapter 7: General Classes of Biomaterials
Chapter 8: Preventive and Intermediary Materials Chapter 9: Restorative Materials: Resin Composites and
Polymers
Chapter 14: Digital Imaging and Processing for Restorations
vii The fourteenth edition of this classic textbook has been extensively updated to include many recent developments in dental biomaterials science and new materials for clinical use. The book continues to be designed for predoctoral dental students and also provides an excellent update of dental bioma- terials science and clinical applications of restorative materials for students in graduate programs and residencies.
Dr. Ron Sakaguchi returns as the lead editor of the fourteenth edition. Dr. Sakaguchi serves as pro- fessor in the Division of Management in the School of Medicine and professor, Division of Biomaterials and Biomechanics in the Department of Restorative Dentistry at Oregon Health & Science University (OHSU) in Portland, Oregon. He earned a BS in cyber- netics from the University of California Los Angeles (UCLA), a DDS from Northwestern University, an MS in prosthodontics from the University of Minnesota, a PhD in biomaterials and biomechanics from Thames Polytechnic (London, England; now the University of Greenwich), and an MBA summa cum laude in entrepreneurship from Babson College.
Dr. Jack Ferracane is a new co-editor of the four- teenth edition. Dr. Ferracane serves as professor and chair of the Department of Restorative Dentistry and division director of Biomaterials and Biomechanics at Oregon Health & Science University (OHSU) in Portland, Oregon. He earned a BS in biology from the University of Illinois and an MS and a PhD in biological materials from Northwestern University.
Dr. John M. Powers returns as a co-editor of the fourteenth edition. He served as the lead editor of the twelfth edition and contributed to the previous eight editions. Dr. Powers is clinical professor of oral biomaterials in the Department of Restorative Dentistry and Prosthodontics at the UTHealth School of Dentistry, The University of Texas Health Science Center at Houston, and senior vice presi- dent of Dental Consultants, Inc. (publisher of The Dental Advisor). Dr. Powers was formerly Director of the Houston Biomaterials Research Center. He earned a BS in chemistry and a PhD in mechanical
engineering and dental materials at the University of Michigan.
We thank our many chapter authors for their effort and expertise: Dr. Roberto Braga of the University of São Paulo; Dr. Isabelle Denry of the University of Iowa; Dr. Sharukh Khajotia of the University of Oklahoma; Dr. David Mahler of Oregon Health &
Science University; Drs. Grayson and Sally Marshall of the University of California San Francisco (UCSF);
Dr. John Mitchell of Midwestern University; Dr.
Sumita Mitra of Mitra Chemical Consulting, LLC, and many years at 3M ESPE; and Dr. Carmem Pfeifer of Oregon Health & Science University.
The organization of the fourteenth edition follows the format of the popular thirteenth edition. Chapters are organized by major clinical procedures. Chapter 3 has been extensively revised with a new focus on materials-centered treatment design. The treatment design approach proposed by Spear and Kokich is discussed where treatment planning starts with an assessment of overall esthetics, to which a consider- ation of function, structure, and biology are added.
A new table presents a summary of the approach with queries for each stage, and relevant materials and properties to be considered. The discussion of material and mechanical properties and their testing in Chapters 4 and 5 is updated and modernized to improve understanding. The history of amalgam and its fabrication now appears in the online companion to Chapter 10, along with other legacy metals and alloys. Tissue engineering materials have been exten- sively updated, with new figures, in Chapter 16.
A website accompanies this textbook. Included is the majority of the procedural, or materials han- dling, content that was in the twelfth and thirteenth editions. The website can be found at http://evolve.
elsevier.com/Sakaguchi/restorative/, where you will also find extensive text and graphics to supple- ment the print version of the book.
Ron Sakaguchi Jack Ferracane John Powers
Preface
ix
1
Role and Significance of Restorative Dental Materials,
1Scope of Materials Covered in Restorative Dentistry, 1
A Systems Approach to Restorative Materials, 2 Application of Various Sciences, 2
Future Developments in Biomaterials, 2
2
The Oral Environment,
5 Enamel, 5The Mineral, 8 Dentin, 9
Physical and Mechanical Properties, 12 The Dentin-Enamel Junction, 15 Oral Biofilms and Restorative Dental
Materials, 17
3
Materials-Centered Treatment Design,
23 Evidence-Based Dentistry, 23Patient Evidence, 23 Scientific Evidence, 23
Planning for Dental Treatment, 24
4
Fundamentals of Materials Science,
29 Mechanical Properties, 29Force, 29 Stress, 30
Stress-Strain Curves, 31 Viscoelasticity, 39
Dynamic Mechanical Properties, 42 Surface Mechanical Properties, 43 The Colloidal State, 45
Diffusion Through Membranes and Osmotic Pressure, 46
Adsorption, Absorption, and Sorption, 46 Surface Tension and Wetting, 47
Adhesion, 48 Optical Properties, 50
Color, 50
Measurement of Color, 50 Surface Finish and Thickness, 52
Opacity, Translucency, Transparency, and Opalescence, 53
Index of Refraction, 53 Optical Constants, 53 Thermal Properties, 56
Temperature, 56
Transition Temperatures, 56 Heat of Fusion, 57
Thermal Conductivity, 58 Specific Heat, 58
Thermal Diffusivity, 59
Coefficient of Thermal Expansion, 59 Electrical Properties, 60
Electrical Conductivity and Resistivity, 60 Dielectric Constant, 61
Electromotive Force, 61 Galvanism, 62
Electrochemical Corrosion, 63 Zeta-Potential, 63
Other Properties, 63
Tarnish and Discoloration, 63 Water Sorption, 64
Setting Time, 64 Shelf Life, 65 Summary, 65
5
Testing of Dental Materials and Biomechanics,
69Compressive Strength, 69 Flexure, 69
Flexural Strength, 69 Permanent Bending, 71 Diametral Tensile Strength, 71 Shear Strength, 71
Torsion, 72
Fatigue Strength, 73 Fracture Toughness, 73 Fractographic Analysis, 73 Tear Strength and Tear Energy, 75 Hardness, 75
Brinell Hardness Test, 76 Knoop Hardness Test, 76 Vickers Hardness Test, 76 Rockwell Hardness Test, 76 Barcol Hardness Test, 77 Shore A Hardness Test, 77 Nanoindentation, 77 Wear, 78
Contents
Setting Time, 79 Measurement, 79
Dynamic Mechanical Analysis, 79 Rheology, 80
Differential Scanning Calorimetry, 80 Spectrometric Techniques, 80 Pycnometry, 81
Bond Strength Test Methods, 81 Macroshear Bond Strength Tests, 82 Macrotensile Bond Strength Tests, 83 Microtensile Bond Strength Tests, 83 Microshear Bond Strength Tests, 83 Push-Out Tests, 83
Methods for Measuring Shrinkage and Stress During the Cure of Resin Composites, 83
Mercury Dilatometer, 83 Bonded Disk, 84 AcuVol, 84
Managing Accurate Resin Curing Test, 84
Cavity Configuration Factor (C-Factor), 84
Stress Analysis and Design of Dental Structures, 85
Polymerization Stress Test, 86 Tensilometer, 86
Tensometer, 87 Crack Analysis, 87
Specifications for Restorative Materials, 87 American Dental Association
Specifications, 88
American Dental Association Acceptance Program, 88
Index of Federal Specifications and Standards, 88
6
Biocompatibility and Tissue Reaction to Biomaterials,
91Measuring Biocompatibility, 91 In Vitro Tests, 92
Animal Tests, 94 Usage Tests, 94
Correlation Among In Vitro, Animal, and Usage Tests, 95
Using In Vitro, Animal, and Usage Tests Together, 96
Standards That Regulate the Measurement of Biocompatibility, 97
Biocompatibility of Dental Materials, 98 Reactions of Pulp, 98
Reaction of Other Oral Soft Tissues to Restorative Materials, 105
Summary, 108
7
General Classes of Biomaterials,
113 Metals and Alloys, 113Chemical and Atomic Structure of Metals, 113 Atomic Structure, 113
Physical Properties of Metals, 115 Polymers, 116
Basic Nature of Polymers, 116 Ceramics, 118
Composites, 120
8
Preventive and Intermediary Materials,
123Pit and Fissure Sealants, 123 Light-Cured Sealants, 123
Air Inhibition of Polymerization, 123 Properties of Sealants, 123
Clinical Studies, 125 Application of Sealants, 125 Glass Ionomers as Sealants, 126 Flowable Composites as Sealants, 126 Glass Ionomers to Prevent the Progression of
Caries, 127
Composition and Reaction, 127 Properties, 127
Resin-Modified Glass Ionomers, 128 Composition and Reaction, 129 Properties, 129
Manipulation, 130
Resin-Modified Glass Ionomers as Cavity Liners, 130
Calcium Hydroxide Cavity Liners, 130 Mineral Trioxide Aggregate, 131 Fluoride Varnishes, 131
Remineralization, 131
9
Restorative Materials: Resin Composites and Polymers,
135Multipurpose Resin Composites, 136 Composition, 136
Polymerization Reactions, 144 Packaging of Composites, 147 Properties of Composites, 147
Physical Properties, 147 Mechanical Properties, 151 Clinical Properties, 152
Composites for Special Applications, 153 Microfilled Composites, 153
Bulk Fill Composites, 154
Syringeable Composites, 154 Laboratory Composites, 155 Core Build-Up Composites, 155 Provisional Composites, 155 Glass Ionomers, 156
Components and Setting Reaction of Conventional Glass Ionomer, 156 Cermets, 157
Components and Setting Reactions of Resin-Modified Glass Ionomers, 158 Tri-Cure Glass Ionomer System, 159 Nanoionomer, 160
Packaging of Glass Ionomers, 161
Clinical Applications of Glass Ionomers, 161 Properties of Glass Ionomers, 161
Compomers, 163
Composition and Setting Reaction, 163 Properties, 164
Manipulation, 164 Light-Curing Units, 164
Quartz-Tungsten-Halogen Light-Curing Units, 164 Blue Light-Emitting Diodes, 164
Prosthetic Applications of Polymers, 165 Physical Form and Composition, 165 Athletic Mouth Protectors, 166
10
Restorative Materials: Metals,
171 Metals for Direct Placement: Amalgam, 171Composition and Morphology, 171
Amalgamation Processes: Admixed Alloys, 172 Physical and Mechanical Properties, 174 Bonding of Amalgam, 177
Dental Casting Alloys, 178 Types and Composition, 178
Metallic Elements Used in Dental Alloys, 180 Noble Alloys, 184
Base-Metal Alloys, 190 Wrought Alloys, 200
Microstructure, 200 Composition, 200 Properties, 201
Wrought Stainless Steel Alloys, 201 Wrought Nickel-Titanium Alloy, 203 Wrought Beta-Titanium Alloy, 204
11
Restorative Materials: Ceramics,
209 Classification of Dental Ceramics, 209Classification by Application, 209 Classification by Fabrication Method, 209 Classification by Crystalline Phase, 209 General Applications of Ceramics in Prosthetic
Dentistry, 210
Metal-Ceramic Crowns and Fixed Dental Prostheses, 210
All-Ceramic Crowns, Inlays, Onlays, and Veneers, 211
Mechanical and Thermal Properties of Dental Ceramics, 211
Toughening Mechanisms, 211 Test Methods, 212
Comparative Data, 213
Optical Properties of Dental Ceramics, 214 All-Ceramic Restorations, 215
Sintered All-Ceramic Materials, 215 Heat-Pressed All-Ceramic Materials, 216 Machinable All-Ceramic Materials, 217 Metal-Ceramic Restorations, 219
Requirements for a Metal-Ceramic System, 220
Metal-Ceramic Bonding, 221
Ceramics for Metal-Ceramic Restorations, 222 Effect of Design on Metal-Ceramic Restora-
tions, 224
Failure and Repair of Metal-Ceramic Restorations, 225
12
Replicating Materials: Impression and Casting,
229Purpose of Impression Materials, 229 Desirable Qualities, 229
Types of Impression Materials, 231 Alginate Hydrocolloids, 231
Elastomeric Impression Materials, 237 Occlusal Registration Materials, 250 Impression Trays, 250
Die, Cast, and Model Materials, 250 Desirable Qualities of a Cast or Die
Material, 250
Dental Plaster and Stone, 251 Epoxy Die Materials, 251
Comparison of Impression and Die Materials, 251
Gypsum Products, 252
Chemical and Physical Nature of Gypsum Products, 252
Properties, 255 Manipulation, 260 Casting Investments, 260
Properties Required of an Investment, 261 Composition, 261
Calcium Sulfate–Bonded Investments, 262 Effect of Temperature on Investment, 262 Thermal and Hygroscopic Casting
Investment, 265 Brazing Investment, 268
Investment for All-Ceramic Restorations, 268
13
Materials for Adhesion and Luting,
273 Principles of Adhesion, 273Adhesive Systems, 275
Bonding to Other Substrates, 280 Repair of Composite, Ceramic, and
Ceramic-Metal Restorations, 282 Classification and Characteristics of Luting
Agents, 282 Classification, 282 Biocompatibility, 283
Interfacial Sealing and Anticariogenic Activity, 283
Adhesion, 283
Mechanical Properties, 283 Handling Properties and
Radiopacity, 283
Viscosity and Film Thickness, 284 Solubility, 284
Esthetics, 284 Acid-Base Cements, 284
Zinc Oxide-Eugenol and Noneugenol Cements, 284
Glass Ionomer, 285
Resin-Modified Glass Ionomer, 287 Calcium Aluminate/Glass Ionomer
Cement, 289
Resin-Based Cements, 289 Resin Cements, 289
Self-Adhesive Resin Cements, 290 Resin Cements for Provisional
Restorations, 292
14
Digital Imaging and Processing for Restorations,
295Dental CAD/CAM Systems, 295 Digital Impressions, 296 Design Software, 297 Processing Devices, 298 Clinical Outcomes, 298
15
Dental and Orofacial Implants,
301 Classification, 301Endosseous Implant, 301
Osseointegration and Biointegration, 301 Factors Affecting the Endosteal Implant, 304
Geometry, 304
Magnitude of the Force, 304 Duration of the Force, 304 Type of Force, 305 Implant Diameter, 305 Implant Length, 305
Surfaces and Biocompatibility, 305 Ion Release, 306
Surfaces, 306
Surface Alterations, 306 Surface Coatings, 308
Implant Materials and Processing, 308 Challenges and the Future, 309
16
Tissue Engineering,
313 Autograft, 313Allograft, 313 Xenograft, 313 Alloplasts, 314
Strategies for Tissue Engineering, 314 Injection of Cells, 314
Guided Tissue Regeneration, 315 Cell Induction, 315
Cells Within Scaffold Matrices, 317 Stem Cells, 318
Biomaterials and Scaffolds, 320 Biological Materials, 320
Ceramic and Glass Materials, 320 Polymeric Materials, 321
Cell Culture Methods, 322
Tissue-Engineered Dental Tissues, 322
Appendix A: Conversion of Units,
327Index,
3311 Developments in materials science, stem cells, imag- ing, three-dimensional (3D) printing, and robotics have dramatically changed the way we look at the replacement of components of the human anatomy.
The replacement of tooth structure lost to disease and injury continues to be a large part of general dental practice. Restorative dental materials are the foundation for the replacement of tooth structure.
Form and function are important considerations in the replacement of lost tooth structure. Although tooth form and appearance are aspects most easily recognized, function of the teeth and supporting tissues contributes greatly to the quality of life. The links between oral and general health are widely accepted. Proper function of the elements of the oral cavity, including the teeth and soft tissues, is needed for eating, speaking, swallowing, and proper breathing.
Restorative dental materials make the reconstruction of the dental hard tissues possible. In many areas, the development of dental materials has progressed more rapidly than for other anatomical prostheses. Because of their long-term success, patients often expect dental prostheses to outperform the natural materials they replace. The application of materials science is unique in dentistry because of the complexity of the oral cavity, which includes bacteria, high forces, ever changing pH, and a warm, fluid environment. The oral cavity is con- sidered to be the harshest environment for a material in the body. In addition, when dental materials are placed directly into tooth cavities as restorative materials, there are very specific requirements for manipulation of the material. Knowledge of materials science and biomechanics is very important when choosing materi- als for specific dental applications and when designing the best solution for restoration of tooth structure and replacement of teeth.
A review of the history of dentistry may be found on the book’s website at http://evolve.elsevier.com/
sakaguchi/restorative.
SCOPE OF MATERIALS COVERED IN RESTORATIVE DENTISTRY
Restorative dental materials include representa- tives from the broad classes of materials: met- als, polymers, ceramics, and composites. Dental materials include such items as resin composites, cements, glass ionomers, ceramics, noble and base metals, amalgam alloys, gypsum materials, cast- ing investments, impression materials, denture base resins, and other materials used in restorative procedures. The demands for material character- istics and performance range from high flexibility required by impression materials to high stiffness required in crowns and fixed dental prostheses.
Materials for dental implants require integration with bone. Some materials are cast to achieve excellent adaptation to existing tooth structure, whereas others are machined to produce very reproducible dimensions and structured geom- etries. When describing these materials, physi- cal and chemical characteristics are often used as criteria for comparison. To understand how a material works, we study its chemical structure, its physical and mechanical characteristics, and how it should be manipulated to produce the best performance.
Most restorative materials are characterized by physical, chemical, and mechanical parameters that are derived from test data. Improvements in these characteristics might be attractive in labo- ratory studies, but the real test is the material’s performance in the mouth and the ability of the material to be manipulated properly by the den- tal team. In many cases, manipulative errors can negate the technological advances for the mate- rial. It is therefore very important for the dental team to understand fundamental materials science and biomechanics to select and manipulate dental materials appropriately.
1
Role and Significance of Restorative
Dental Materials
A SYSTEMS APPROACH TO RESTORATIVE MATERIALS
The practice of clinical dentistry depends not only on a complete understanding of the various clinical techniques but also on an appreciation of the funda- mental biological, chemical, and physical principles that support the clinical applications. It is important to understand the “how” and “why” associated with the function of natural and synthetic dental materials.
A systems approach to assessing the chemical, physical, and engineering aspects of dental materi- als and oral function, along with the physiological, pathological, and other biological studies of the tis- sues that support the restorative structures, provides the best patient outcomes. This integrative approach, when combined with the best available scientific evi- dence, clinician experience, patient preferences, and patient modifiers, results in the best patient-centered care.
APPLICATION OF VARIOUS SCIENCES
In the chapters that follow, fundamental characteris- tics of materials are presented along with numerous practical examples of how the basic principles relate to clinical applications. Test procedures and fabrica- tion techniques are discussed briefly but not empha- sized. Many of the details of manipulation are found on the book’s website at http://evolve.elsevier.com/
sakaguchi/restorative.
A more complete understanding of fundamental principles of materials and mechanics is important for the clinician to design and provide a progno- sis for restorations. For example, the prognosis of long-span fixed dental prostheses, or bridges, is dependent on the stiffness and fracture resistance of the materials. When considering esthetics, the hardness of the material is an important property because it influences the ability to polish the mate- rial. Some materials release fluoride when exposed to water, which might be beneficial in high-caries- risk patients. When selecting a ceramic for in-office fabrication of an all-ceramic crown, the machining characteristic of ceramics is important. Implants have a range of bone and soft tissue adaptations that are dependent on surface texture, coatings, and implant geometry. These are just a few examples of the many interactions between the clinical perfor- mance of dental materials and fundamental scien- tific principles.
The toxicity of and tissue reactions to dental mate- rials are receiving more attention as a wider variety of materials are being used and as federal agencies demonstrate more concern in this area. A further indication of the importance of the interaction of
materials and tissues is the development of recom- mended standard practices and tests for the biologi- cal interaction of materials through the auspices of the American Dental Association (ADA).
After many centuries of dental practice, we con- tinue to be confronted with the problem of replacing tooth tissue lost by either accident or disease. In an effort to constantly improve our restorative capa- bilities, the dental profession will continue to draw from materials science, product design, engineering, biology, chemistry, and the arts to further develop an integrated practice of dentistry.
FUTURE DEVELOPMENTS IN BIOMATERIALS
In the United States about 50% of adults aged 20 to 64 have lost at least one permanent tooth to an accident, periodontal disease, a failed root canal, or tooth decay. In adults aged 65 and older, almost 19%
have lost all of their natural teeth. That number is twice as large for adults aged 75 and over than for adults aged 65 to 74 (CDC/NCHS, National Health and Nutrition Examination Survey, 2011–2012). For children aged 5 to 19 years, 18% have untreated den- tal caries. For adults aged 20 to 44, that number is 27%. The demand for restorative care is tremendous.
Advances in endodontology and periodontology enable people to retain teeth longer, shifting restor- ative care from replacement of teeth to long-term restoration and maintenance. Development of suc- cessful implant therapies has encouraged patients to replace individual teeth with fixed, single-tooth restorations rather than with fixed or removable dental prostheses. For those patients with good access to dental care, single-tooth replacements with implants are becoming a more popular option because they do not involve the preparation of adjacent teeth as for a fixed, multiunit restoration.
Research into implant coatings, surface textures, graded properties, alternative materials, and new geometries will continue to grow. For those with less access, removable prostheses will continue to be used.
An emphasis on esthetics continues to be popular among consumers, and this will continue to drive the development and sales of tooth-whitening systems and esthetic restorations. There appears to be an emerging trend for a more natural looking appear- ance with some individuality as opposed to the uniform, sparkling white dentition that was previ- ously requested by many patients. This will encour- age manufacturers to develop materials that mimic natural dentition even more closely by providing the same depth of color and optical characteristics of natural teeth.
With the aging of the population, restorations for exposed root surfaces and worn dentitions will become more common. These materials will need to function in an environment with reduced sali- vary flow and atypical salivary pH and chemistry.
Adhesion to these surfaces will be more challenging.
This segment of the population will be managing multiple chronic diseases with many medications and will have difficulty maintaining an adequate regimen of oral home care. Restorative materials will be challenged in this difficult environment.
The interaction between the fields of biomaterials and molecular biology is growing rapidly. Advances in tissue regeneration will accelerate. Developments in nanotechnology are having a major impact on materials science. The properties we currently understand at the macro and micro levels will be very different at the nano level. Biofabrication and bioprinting methods are creating new structures and materials. This is a very exciting time for materials research, and clinicians will have much to look for- ward to in the near future as this body of research develops new materials for clinical applications.
Bibliography
Centers for Disease Control and Prevention and National Center for Health Statistics. National Health and Nutrition Examination Study. 2011–2012.
Choi CK, Breckenridge MT, Chen CS. Engineered materials and the cellular microenvironment: a strengthening inter- face between cell biology and bioengineering. Trends Cell Biol. 2010;20(12):705–714.
Denry I, Kelly JR. Emerging ceramic-based materials for dentistry. J Dent Res. 2014;93(12):1235–1242.
Horowitz RA, Coelho PG. Endosseous implant: the journey and the future. Compend Contin Educ Dent.
2010;31(7):545–547.
Jones JR, Boccaccini AR. Editorial: a forecast of the future for biomaterials. J Mater Sci Mater Med. 2006;17:963–964.
Nakamura M, Iwanaga S, Henmi C, Arai K, Nishiyama Y. Biomatrices and biomaterials for future develop- ments of bioprinting and biofabrication. Biofabrication.
2010;2(1):014110.
Rekow ED, Fox CH, Watson T, Petersen PE. Future inno- vation and research in dental restorative materials. Adv Dent Res. 2013;25(1):2–7.
U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (CDC) and National Center for Health Statistics (NCHS). Health, United States; 2015.
U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General—Executive Summary. Rockville, MD: U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health;
2000.
5 The tooth contains three specialized calcified tissues:
enamel, dentin, and cementum (Fig. 2.1). Enamel is unique in that it is the most highly calcified tissue in the body and contains the least organic content of any of these tissues. Enamel provides the hard outer cov- ering of the crown that allows efficient mastication.
Dentin and cementum, like bone, are vital, hydrated, biological composite structures formed mainly of a collagen type I matrix reinforced with the calcium phosphate mineral called apatite. Dentin forms the bulk of the tooth and is joined to the enamel at the dentin-enamel junction (DEJ). The dentin of the tooth root is covered by cementum that provides connection of the tooth to the alveolar bone via the periodontal ligament. Although the structure of these tissues is often described in dental texts, the properties are often discussed only superficially. However, these proper- ties are important with regard to the interrelationships of the factors that contribute to the performance neces- sary for the optimum function of these tissues.
In restorative dentistry we are interested in pro- viding preventive treatments that will maintain tissue integrity and replace damaged tissues with materials that ideally will mimic the natural appear- ance and performance of those tissues when neces- sary. Thus knowledge of the structure and properties of these tissues is desirable both as a yardstick to measure the properties and performance of restor- ative materials and as a guide to the development of materials that will mimic their structure and func- tion. In addition, many applications, such as dental bonding, require us to attach synthetic materials to the calcified tissues, and these procedures rely on detailed knowledge of the structure and properties of the adhesive tissue substrates.
ENAMEL
Fig. 2.1 shows a schematic diagram of a posterior tooth sectioned to reveal the enamel and dentin
components. Enamel forms the hard outer shell of the crown and as the most highly calcified tissue is well suited to resisting wear due to mastication.
Enamel is formed by ameloblasts starting at the DEJ and proceeding outward to the tooth surface.
The ameloblasts exchange signals with odontoblasts located on the other side of the DEJ at the start of the enamel and dentin formation, and the odontoblasts move inward from the DEJ as the ameloblasts form- ing enamel move outward to form the enamel of the crown. Most of the enamel organic matrix composed of amelogenins and enamelins is resorbed during tooth maturation to leave a calcified tissue that is largely composed of mineral and a sparse organic matrix. The structural arrangement of enamel forms keyhole-shaped structures known as enamel prisms or rods that are about 5 μm across, as seen in Fig. 2.2.
The overall composition is about 96% mineral by weight, with 1% lipid and protein and the remainder
2
The Oral Environment
Enamel Dentin
Pulp
Inner cervical
Outer
Inner
FIG. 2.1 Schematic diagram of a tooth cut longitudi- nally to expose the enamel, dentin, and the pulp cham- ber. On the right side are illustrations of dentin tubules as viewed from the top, which show the variation in the tubule number with location. At the left is an illustration of the change in direction of the primary dentin tubules as secondary dentin is formed. (From Marshall SJ, Balooch M, Breunig T, et al. Human dentin and the dentin-resin adhesive interface. Acta Mater. 1998;46:2529–2539.)
being water. The organic portion and water probably play important roles in tooth function and pathology, and it is often more useful to describe the composition on a volume basis. On that basis we see the organic components make up about 3% and water 12% of the structure. The mineral is formed and grows into very long crystals of hexagonal shape about 40 nm across;
these crystals have not been synthetically duplicated.
There is some evidence that the crystals may span the whole enamel thickness, but this is difficult to prove because most preparation procedures lead to frac- ture of the individual crystallites. It appears that they are at least thousands of nanometers long. If this is true, then enamel crystals provide an extraordinary
“aspect” ratio (length-to-width ratio) for a nanoscale material, and they are very different from the much smaller dentin crystals. The crystals are packed into enamel prisms or rods that are about 5 μm across, as shown in Fig. 2.2. These prisms are revealed easily by
acid etching and extend in a closely packed array from the DEJ to the enamel surface and lie roughly perpen- dicular to the DEJ, except in cuspal areas where the rods twist and cross, known as decussation, which may increase fracture resistance. About 100 crystals of the mineral are needed to span the diameter of a prism, and the long axes of the crystals tend to align them- selves along the prism axes, as seen in Fig. 2.2.
The crystals near the periphery of each prism deviate somewhat from the long axis toward the interface between prisms. The deviation in the tail of the prism is even greater. The individual crys- tals within a prism are also coated with a thin layer of lipid and/or protein that plays important roles in mineralization, although much remains to be learned about the details. Recent work suggests that this protein coat may lead to increased toughness of the enamel. The interfaces between prisms, or inter- rod enamel, contain the main organic components Interrod
enamel Head Tail
A B
40.0
30.0
20.0
10.0
0 10.0 20.0 30.0 40.00
C
FIG. 2.2 Enamel microstructure showing a schematic diagram of keyhole-shaped enamel prisms or rods about 5 μm in diameter (B). Atomic force microscopy images showing prism cross sections (A) and along axes of the prisms (C).
Crystallite orientation deviates in the interrod and tail area, and the organic content increases in the interrod area. (Modified from Habelitz S, Marshall SJ, Marshall GW, et al. Mechanical properties of human dental enamel on the nanometer scale. Arch Oral Biol. 2001;46:173–183.)
of the structure and act as passageways for water and ionic movement. These areas are also known as prism sheaths. These regions are of vital importance in etching processes associated with bonding and other demineralization processes, such as caries.
Etching of enamel with acids such as phosphoric acid, commonly used in enamel bonding, eliminates smear layers associated with cavity preparation,
dissolves persisting layers of prismless enamel in deciduous teeth, and differentially dissolves enamel crystals in each prism. The pattern of etched enamel is categorized as type 1 (preferential prism core etch- ing; Fig. 2.2A), type 2 (preferential prism periphery etching; Fig. 2.3C), and type 3 (mixed or uniform).
Sometimes these patterns appear side by side on the same tooth surface (Fig. 2.3E). No differences in
C D
E 25 m
A B
FIG. 2.3 Etching enamel. (A) Gel etchant dispensed on the enamel portion of the preparation. (B) Frosty appearance after etching, rinsing, and drying. (C) Magnified view of etch pattern with preferential prism periphery etch (type 1). (D) Bonding agent revealed after dissolving enamel. (E) Mixed etch patterns showing type 1 (light prisms with dark periphery) and type 2 (dark cores with light periphery) etching on the same surface. (C and D, After Marshall GW, Olson LM, Lee CV.
SEM Investigation of the variability of enamel surfaces after simulated clinical acid etching for pit and fissure sealants. J Dent Res.
1975;54:1222–1231; E, After Marshall GW, Olson LM, Lee CV. SEM Investigation of the variability of enamel surfaces after simu- lated clinical acid etching for pit and fissure sealants. J Dent Res. 1975;54:1222–1231; E, from Marshall GW, Marshall SJ, Bayne SC.
Restorative dental materials: scanning electron microscopy and x-ray microanalysis. Scanning Microsc. 1988;2:2007–2028.)
micromechanical bond strength of the different etch- ing patterns have been established. In a standard cav- ity preparation for a composite, the orientation of the enamel surfaces being etched could be perpendicular to enamel prisms (perimeter of the cavity outline), oblique cross section of the prisms (beveled occlusal or proximal margins), and axial walls of the prisms (cavity preparation walls). During the early stages of etching, when only a small amount of enamel crystal dissolution occurs, it may be difficult or impossible to detect the extent of the process. However, as the etching pattern begins to develop, the surface etched with phosphoric acid develops a frosty appearance (Fig. 2.3B), which has been used as the traditional clinical indicator for sufficient etching. This rough- ened surface provides the substrate for infiltration of bonding agents that can be polymerized after pen- etration of the etched enamel structure so that they form micromechanical bonds to the enamel when polymerized. With self-etching bonding agents, this frosty appearance cannot be detected.
There are two other important structural varia- tions of enamel. Near the DEJ the enamel prism struc- ture is not as well developed in the very first enamel formed, so that the enamel very close to the DEJ may appear aprismatic or without the prism-like structure.
Similarly, on the outer surface of the enamel, at com- pletion of the enamel surface, the ameloblasts degen- erate and leave a featureless layer, called prismless enamel, on the outer surface of the crown. This layer is more often observed in deciduous teeth and is often worn off in permanent teeth. However, if present, this causes some difficulty in getting an effective etching pattern and may require roughening of the surface or additional etching treatments. The outer surface of the enamel is of great clinical significance because it is the surface subjected to daily wear and undergoes
repeated cycles of demineralization and remineral- ization. As a result of these cycles, the composition of the enamel crystals may change, for example, as a result of exposure to fluoride. Thus the properties of the enamel might be expected to vary from the exter- nal to the internal surface. Such variations, including a thin surface veneer of fluoride-rich apatite crystals, create differences in the enamel properties within the enamel. Enamel is usually harder at the occlusal and cuspal areas and less hard nearer the DEJ. Fig. 2.4 shows an example of the difference in hardness.
THE MINERAL
The mineral of all calcified tissues is a highly defec- tive relative of the mineral hydroxyapatite (HA).
The biological apatites of calcified tissues are differ- ent from the ideal HA structure in that the defects and chemical substitutions generally make them weaker and more soluble in acids. HA has the simple formula Ca10(PO4)6(OH)2, with an ideal molar ratio of calcium to phosphorus (Ca/P) of 1.67 and a hex- agonal crystal structure. The apatite of enamel and dentin has a much more variable composition that depends on its formative history and other chemi- cal exposures during maturity. Thus the mineral in enamel and dentin is a calcium-deficient, carbonate- rich, and highly substituted form related to HA.
Metal ions such as magnesium (Mg) and sodium (Na) may substitute for calcium, whereas carbonate substitutes for the phosphate and hydroxyl groups.
These substitutions distort the structure and make it more soluble. Perhaps the most beneficial substitu- tion is the fluorine (F) ion, which substitutes for the hydroxyl group (OH) in the formula and makes the structure stronger and less soluble. Complete sub- stitution of F for (OH) in HA yields fluoroapatite mineral, Ca10(PO4)6(F)2, which is much less soluble than HA or the defective apatite of calcified tissues.
It is worth noting that HA has attracted considerable attention as an implantable calcified tissue replace- ment. It has the advantage of being a purified and stronger form of the natural mineral and releases no harmful agents during biological degradation. Its major shortcoming is that it is extremely brittle and sensitive to porosity or defects, and therefore it frac- tures easily in load-bearing applications.
The approximate carbonate contents of the enamel and dentin apatites are significantly different, about 3% and 5% carbonate, respectively. All other fac- tors being equal, this would make the dentin apatite more soluble in acids than the enamel apatite. Things are not equal, however, and the dentin apatite crys- tals are much smaller than the enamel crystals. This means that the dentin crystals present a higher sur- face area to attacking acids and contain many more Buccal
Hardness (GPa) Lingual
6 5.5 5 4.5 4 3.5 3 2.5 FIG. 2.4 Nanoindentation mapping of the mechani- cal properties of human molar tooth enamel. (From Cuy JL, Mann AB, Livi KJ, et al. Nanoindentation mapping of the mechanical properties of human molar tooth enamel. Arch Oral Biol. 2002;47(4):281–291.)
defects per unit volume and thus exhibit consider- ably higher solubility. Finally, as discussed further below, the dentin mineral occupies only about 50%
of the dentin structure, so there is not as much apatite in the dentin as there is in the enamel. All of these factors multiply the susceptibility of dentin to acid attack and provide insight into the rapid spread of caries when it penetrates the DEJ.
DENTIN
Dentin is a complex hydrated biological com- posite structure that forms the bulk of the tooth.
Furthermore, dentin is modified by physiological, aging, and disease processes that result in differ- ent forms of dentin. These altered forms of dentin may be the precise forms that are most important in restorative dentistry. Some of the recognized varia- tions include primary, secondary, reparative or ter- tiary, sclerotic, transparent, carious, demineralized, remineralized, and hypermineralized. These terms reflect alterations in the fundamental components of the structure as defined by changes in their arrange- ment, interrelationships, or chemistry. A number of these may have important implications for our ability to develop long-lasting adhesion or bonds to dentin.
Primary dentin is formed during tooth develop- ment. Its volume and conformation, reflecting tooth form, vary with the size and shape of the tooth.
Dentin is composed of about 50 volume percent (vol%) carbonate-rich, calcium-deficient apatite;
30 vol% organic matter, which is largely type I col- lagen; and about 20 vol% fluid, which is similar to plasma. Other noncollagenous proteins are thought to be involved in dentin mineralization and other functions such as controlling crystallite size and orientation. The role of noncollagenous proteins in biomineralization or simpler molecules that can mimic some of their functions may lead to dentin remineralization methods; however, these functions and possibilities are not discussed further in this text.
The major components are distributed into distinc- tive morphological features to form a vital and com- plex hydrated composite in which the morphology varies with location and undergoes alterations with age or disease. The tubules, one distinct and impor- tant feature of dentin, represent the tracks taken by the odontoblastic cells from the DEJ or cementum at the root to the pulp chamber and appear as tunnels piercing the dentin structure (Fig. 2.5). The tubules converge on the pulp chamber, and therefore tubule density and orientation vary from location to location (see Fig. 2.1). Tubule number density is lowest at the DEJ and highest at the predentin surface at the junc- tion to the pulp chamber, where the odontoblastic cell bodies lie in nearly a close-packed array. Lower
tubule densities are found in the root. The contents of the tubules include odontoblast processes, for all or part of their course, and fluid. The extent of the odontoblast process is still uncertain, but evidence is mounting that it extends to the DEJ. For most of its course, the tubule lumen is lined by a highly mineral- ized cuff of peritubular dentin approximately 0.5 to 1 μm thick (Fig. 2.6). Because the peritubular dentin forms after the tubule lumen has been formed, some argue that it may be more properly termed intratubu- lar dentin and contains mostly apatite crystals with little organic matrix. A number of studies have con- cluded that the peritubular dentin does not contain collagen and therefore might be considered a sepa- rate calcified tissue. The tubules are separated by intertubular dentin composed of a matrix of type I collagen reinforced by apatite (see Figs. 2.5 and 2.6).
This arrangement means that the amount of intertu- bular dentin varies with location. The apatite crystals are much smaller (approximately 5 × 30 × 100 nm) than the apatite found in enamel and contain about 5% carbonate. The small crystallite size, defect struc- ture, and higher carbonate content lead to the greater dissolution susceptibility described above.
Estimates of the size of tubules, the thickness of the peritubular region, and the amount of intertubu- lar dentin have been made in a number of studies.
Calculations for occlusal dentin as a function of posi- tion from these data show that the percentage tubule area and diameter vary from about 22% and 2.5 μm near the pulp to 1% and 0.8 μm at the DEJ, respec- tively. Intertubular matrix area varies from 12% at the
30kv 2.00kx 5.0 959
FIG. 2.5 Scanning electron microscopy image of nor- mal dentin showing its unique structure as seen from two directions. At the top is a view of the tubules, each of which is surrounded by peritubular dentin. Tubules lie between the dentin-enamel junction and converge on the pulp chamber. The perpendicular surface at the bottom shows a fracture surface revealing some of the tubules as they form tunnel-like pathways toward the pulp. The tubule lumen normally contains fluid and processes of the odontoblastic cells. (From Marshall GW. Dentin: microstructure and charac- terization. Quintessence Int. 1993;24:606–617.)
predentin to 96% near the DEJ, whereas peritubular dentin ranges from over 60% down to 3% at the DEJ.
Tubule densities are compared in Table 2.1 based on work by various investigators. It is clear that the structural components will vary considerably over their course and necessarily result in location-depen- dent variations in morphology, distribution of the structural elements, and important properties such as permeability, moisture content, and available surface area for bonding. They may also affect bond strength, hardness, and other properties.
Because the odontoblasts come to rest just inside the dentin and line the walls of the pulp chamber after tooth formation, the dentin-pulp complex can be considered a vital tissue. This is different from mature enamel, which is acellular. Over time, sec- ondary dentin forms and the pulp chamber gradu- ally becomes smaller. The border between primary and secondary dentin is usually marked by a change in orientation of the dentin tubules. Furthermore, the odontoblasts react to form tertiary dentin in response to insults such as caries or tooth preparation, and this form of dentin is often less well organized than the primary or secondary dentin.
Early enamel carious lesions may be reversed by remineralization treatments. However, effective remineralization treatments are not yet available for dentin, and therefore the current standard of care dictates surgical intervention to remove highly dam- aged tissue and then restoration as needed. Thus it is important to understand altered forms of dentin and the effects of such clinical interventions.
When dentin is cut or abraded by dental instru- ments, a smear layer develops and covers the sur- face and obscures the underlying structure (Fig.
2.7). The bur cutting marks are shown in Fig. 2.7A and at higher magnification in Fig. 2.7B. Fig. 2.7C shows the smear layer thickness from the side and the development of smear plugs as the cut dentin debris is pushed into the dentin tubule lumen. The advantages and disadvantages of the smear layer have been extensively discussed for several decades.
It reduces permeability and therefore aids in main- taining a drier field, and it reduces infiltration of nox- ious agents into the tubules and perhaps the pulp.
However, it is now generally accepted that it is a hin- drance to dentin bonding procedures and therefore is normally removed or modified by some form of acid conditioning.
Acid etching or conditioning allows for removal of the smear layer and alteration of the superficial dentin, opening channels for infiltration by bond- ing agents. Fig. 2.8 shows what happens in such an etching treatment. The tubule lumens widen as the peritubular dentin is preferentially removed because it is mostly mineral with sparse protein.
The widened lumens form a funnel shape that is not very retentive.
Fig. 2.9 shows these effects in a slightly different way. Unetched dentin in Fig. 2.9A (top) has small tubules and peritubular dentin, which is removed in A
Peritubular dentin
Intertubular dentin
B
P
I
20 kv 5.0 kx 2.00 956
FIG. 2.6 Fracture surface of the dentin. (A) Viewed from the occlusal direction. (B) Viewed longitudinally. Peritubular (P; also called intratubular) dentin forms a cuff or lining around each tubule. The tubules are separated from one another by intertubular dentin (I). (Courtesy G.W. Marshall.)
TABLE 2.1 Comparison of mean numerical Density of Tubules in Occlusal Dentin
Outer Dentin Middle Dentin Inner Dentin 15,000/mm2 35,000/mm2 65,000/mm2 20,000/mm2 35,000/mm2 43,000/mm2 24,500/mm2 40,400/mm2 51,100/mm2 18,000/mm2 39,000/mm2 52,000/mm2 From data reported in Marshall GW. Dentin: microstructure and charac- terization. Quintessence Int. 1993;24:606–617.
the treated dentin at the exposed surface after etch- ing (bottom). The two-dimensional network of colla- gen type I fibers is shown after treatment in Fig. 2.9A.
Fig. 2.9B shows progressive demineralization of a dentin collagen fibril in which the external mineral and proteins are slowly removed to reveal the typical banded pattern of type I collagen. In Fig. 2.9C, this pattern is seen at high magnification of the treated dentin shown in Fig. 2.9A.
If the demineralized dentin is dried, the remain- ing dentin matrix shrinks and the collagen fibrils become matted and difficult to penetrate by bonding agents. This is shown in Fig. 2.10, which compares demineralized and dried dentin with demineralized and hydrated dentin.
Most restorative procedures involve dentin that has been altered in some way. Common alterations include formation of carious lesions that form vari- ous zones and include transparent dentin that forms under the caries-infected dentin layer. Transparent dentin results when the dentin tubules become filled
with mineral, which changes the refractive index of the tubules and produces a translucent or transpar- ent zone.
Fig. 2.11 shows a section through a tooth with a carious lesion, which has been stained to reveal its zones. The gray zone under the stained and severely demineralized dentin is the transparent layer (Fig.
2.11A). Fig. 2.11B shows the transparent dentin in which most of the tubule lumens are filled with min- eral. After etching, as shown in Fig. 2.11C, the peri- tubular dentin is etched away, but the tubules retain plugs of the precipitated mineral, which is more resistant to etching. This resistance to etching makes bonding more difficult.
Several other forms of transparent dentin are formed as a result of different processes. A second form of transparent dentin results from bruxism.
An additional form of transparent dentin results from aging as the root dentin gradually becomes transparent. In addition, noncarious cervical lesions, often called abfraction or notch lesions, form at the A
B C
SL
S.P.
FIG. 2.7 Smear layer formation. (A) Bur marks on dentin preparation. (B) Higher magnification showing smear layer surface and cutting debris. (C) Section showing smear layer (SL) and smear plugs (S.P.). (A and B, from Marshall GW, Marshall SJ, Bayne SC. Restorative dental materials: scanning electron microscopy and x-ray microanalysis. Scanning Microsc. 1988;2:2007–
2028; C, from Pashley DH, Tao L, Boyd L, et al. Scanning electron microscopy of the substructure of smear layers in human dentine.
Arch Oral Biol. 1988;33(4):265–270.)
enamel-cementum or enamel-dentin junction, usu- ally on facial or buccal surfaces. Their etiology is not clear at this point; their formation has been attrib- uted to abrasion, tooth flexure, and erosion, or some combination of these processes. Nonetheless, these lesions occur with increasing frequency with age, and the exposed dentin becomes transparent as the tubules are filled. Fig. 2.12 shows examples of trans- parent dentin in which the tubule lumens are com- pletely filled.
The properties of the transparent dentin may dif- fer from one to another depending on the processes that lead to deposit of the mineral in the tubules.
Several studies have shown that elastic properties of the intertubular dentin are not altered by aging, although the structure may become more suscepti- ble to fracture. Similarly, arrested caries will contain transparent dentin and this has often been called scle- rotic dentin, a term that implies it may be harder than normal dentin. However, other studies have shown that the elastic properties of the intertubular dentin
may actually be unaltered or lower than normal dentin.
Physical and Mechanical Properties
The marked variations in the structural elements of dentin when located within the tooth imply that the properties of dentin will vary considerably with location. That is, variable structure leads to variable properties.
Because one major function of tooth structure is to resist deformation without fracture, it is useful to have knowledge of the forces that are experienced by teeth during mastication. Measurements have given values on cusp tips of about 77 kg distributed over the cusp tip area of 0.039 cm2, suggesting a stress of about 200 MPa.
Difficulties in Testing
In Table 2.2, values are presented for some important properties of enamel and dentin. The wide spread
5 10 15
5 10 15
5 10 15
C
B
D
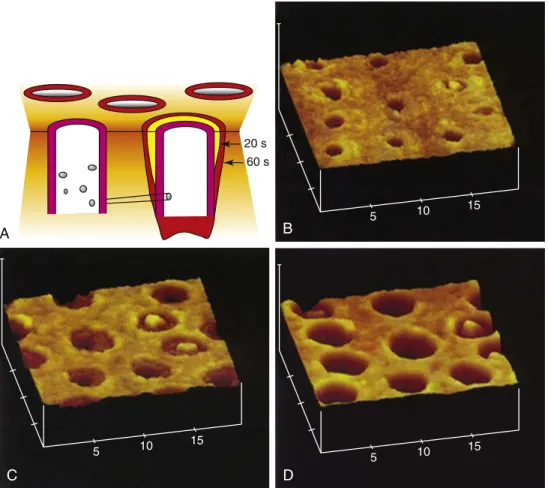
20 s 60 s
A
FIG. 2.8 Stages of dentin demineralization. (A) Schematic showing progressive stages of dentin demineralization.
(B–D) Atomic force microscopy images showing stages of etching. The etching leads to wider lumens as peritubular dentin is dissolved and funnel-shaped openings are formed. (B–D, from Marshall GW. Dentin: microstructure and characterization.
Quintessence Int. 1993;24:606–617.)
FIG. 2.9 Etching of dentin removes mineral from the intertubular dentin matrix leaving a collagen-rich layer and widening the dentin tubule orifices.
(A) After etching, the tubule lumens are enlarged and the collagen network sur- rounding the tubules can be seen after fur- ther treatment. (B) Isolated dentin collagen fiber is slowly demineralized revealing the typical 67-nm repeat pattern of type I col- lagen. (C) High magnification view of col- lagen fibers in (A). (A and C, from Marshall GW, Yucel N, Balooch M, et al. Sodium hypo- cholorite alterations of dentin and dentin col- lagen. Surf Sci. 2001;491:444–455; B, modified from Balooch M, Habelitz S, Kinney JH, et al.
Mechanical properties of mineralized collagen fibrils as influenced by demineralization. J Struct Biol. 2008;162:404–410.)
A
Unetched
Treated
B
484 s
360 s
0 s 100 nm
C
600 400 200
A B
FIG. 2.10 Demineralized dentin is sensitive to moisture and shrinks on drying. (A) Demineralized dentin undergoes shrinkage when air dried, forming a collapsed layer of collagen that is difficult to infiltrate with resin-bonding agents. (B) When kept moist, the collagen network is open and can be penetrated by bonding agents. (From Marshall GW, Marshall SJ, Kinney JH, et al. The dentin substrate: structure and properties related to bonding. J Dent. 1997;25:441–458.)
A
Trans
B
10 20
30 40
C
10 20
30 40
FIG. 2.11 Transparent dentin associated with carious lesions. (A) Carious lesion showing dentin carious zones revealed by staining, including the grayish transparent zone. (B) Atomic force microscopy of carious transparent dentin before etch- ing. (C) After etching, the tubule lumens remain filled even as the peritubular dentin is etched away. (A, from Zheng L, Hilton JF, Habelitz S, et al. Dentin caries activity status related to hardness and elasticity. Eur J Oral Sci. 2003;111(3):243–252; B and C, from Marshall GW, Chang JY, Gansky SA, et al. Demineralization of caries-affected transparent dentin by citric acid: an atomic force microscopy study. Dent Mater. 2001;17:45–52.)
15kv 2.0kx 5.00 523
A B 15kv 2.00kx 5.0 519
FIG. 2.12 Transparent dentin. (A) Viewed from the facial direction. (B) Viewed longitudinally. The transparent dentin results from filling of the tubules with mineral deposits that alter the optical properties of the tooth. (Courtesy G.W. Marshall.)
of values reported in the literature is remarkable.
Some of the reasons for these discrepancies should be appreciated and considered in practice or when reading the literature.
First, human teeth are small, and therefore it is difficult to get large specimens and hold them, mak- ing the use of standard mechanical testing such as tensile, compressive, or shear tests difficult. When testing bonded teeth, the problem is even more com- plicated, and special tests have been developed to obtain insights into these properties. From the previ- ous discussion of structural variations, it is also clear that testing such small inhomogeneous specimens means that the properties will not be uniform.
Another problem is the great variation in struc- ture in both tissues. Enamel prisms are aligned generally perpendicular to the DEJ, whereas dentin tubules change their number density with depth as they course toward the pulp chamber. Preparing a uniform sample with the structures running all in one direction for testing is challenging. In addition, properties generally vary with direction and loca- tion, and the material is not isotropic; therefore the best a single value can tell you is some average value for the material.
Storage and time elapsed since extraction are also important considerations. Properties that exist in a natural situation or in situ or in vivo are of greatest interest. Clearly this condition is almost impossible to achieve in most routine testing, so changes that have occurred as a result of storage conditions prior to testing must be considered. It is also important to consider biological hazards because extracted teeth must be treated as potentially infective. How do you sterilize the teeth without altering their properties?
Autoclaving undoubtedly alters the properties of proteins and is therefore not appropriate for dentin, and it might also affect enamel.
Finally, the fluid content of these tissues must be considered. Moisture is a vital component of both tissues, and in vivo conditions cannot be replicated if the tissues have been desiccated (see Fig. 2.10).
This becomes a critically important consideration in bonding to these tissues, as is discussed further in Chapter 13. In contrast to the importance of this issue is the issue of convenience. It is much more difficult to test the tissues in a fully hydrated condition than in a dry condition. All of these factors and a number of others, such as temperature of testing, will influ- ence the results and contribute to a spread in the val- ues reported for the properties.
Despite these limitations, some generalizations about the properties of these tissues are useful (see Table 2.1). Root dentin is generally weaker and softer than cor