Ectopic Pregnancy
Editor
Ectopic Pregnancy
A Clinical Casebook
Editor Togas Tulandi
Department of Obstetrics and Gynecology
McGill University Montreal Québec Canada
ISBN 978-3-319-11139-1 ISBN 978-3-319-11140-7 (eBook) DOI 10.1007/978-3-319-11140-7
Library of Congress Control Number: 2014959416 Springer Cham Heidelberg New York Dordrecht London
© Springer International Publishing Switzerland 2015
This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on micro- films or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar meth- odology now known or hereafter developed.
The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use.
The publisher, the authors and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publica- tion. Neither the publisher nor the authors or the editors give a warranty, express or implied, with respect to the material contained herein or for any errors or omissions that may have been made.
Printed on acid-free paper
Springer International Publishing is part of Springer Science+Business Media (www.springer.com)
v
There have been many reviews and books on ectopic pregnancy.
So, why produce another book? In fact, a casebook on ectopic preg- nancy is unique and has never been published. More importantly, due to advances in the management of ectopic pregnancy, clini- cians, and researchers are not always current with their knowledge.
In this book, we presented real cases that were treated by our expert contributors. Each chapter contains a case report, a discus- sion about diagnosis and assessment, and management of the case followed by images. At the end of the chapter, we provide clinical pearls and pitfalls about the topic.
The book starts with risk factors related to ectopic pregnancy, and human chorionic gonadotropin (hCG) discriminatory zone.
It is followed by “Pregnancy of unknown location” and “Ecto- pic pregnancy after in-vitro fertilization.” Chapters 5–7 deal with medical and surgical treatments of ectopic pregnancy. For medical treatment, patient compliance is crucial and discussed in Chap. 8.
Inadvertent methotrexate administration to a woman with an intra- uterine pregnancy and its implication is discussed in Chaps. 9 and 10. Different types of ectopic pregnancy including the rare types and their management are discussed in Chaps. 10–20. The last chapter discusses fertility after an ectopic pregnancy.
This concise casebook on ectopic pregnancy is for practicing physicians, obstetricians and gynecologists, residents and fellows
in Obstetrics and Gynecology, and allied health care professionals.
Readers will gain an understanding of many aspects of different types of ectopic pregnancy and their management. We also hope that this book will be helpful in preparing students for examina- tion, and directing new investigations and the clinical management of patients.
vi Preface
Professor of Obstetrics and Gynecology, and Milton Leong Chair in Reproductive Medicine McGill University
Editor Togas Tulandi MD, MHCM
vii
1 Identification of Risk Factors of Ectopic Pregnancy ... 1 Ali Ardehali, Ishwari Casikar and George Condous
2 Discriminatory Serum hCG Level for Ectopic
Pregnancy ... 11 Ishai Levin and Shiri Shinar
3 Pregnancy of Unknown Location ... 19 Shabnam Bobdiwala and Tom Bourne
4 Ectopic Pregnancy After In Vitro Fertilization ... 27 Lisa Caronia, Rebecca Flyckt and Tommaso Falcone
5 Surgical Treatment of Ectopic Pregnancy ... 33 Jillian Main and Camran Nezhat
6 Bleeding Ectopic Pregnancy ... 41 M. Jean Uy-Kroh
7 Medical Treatment of Ectopic Pregnancy ... 49 Togas Tulandi
8 Compliance with Methotrexate Treatment
for Ectopic Pregnancy ... 55 Ishai Levin and Benny Almog
9 Inadvertent Methotrexate Administration ... 61 Togas Tulandi and Senem Ates
10 Effect of Methotrexate Treatment for Ectopic
Pregnancy on Current and Subsequent Pregnancy ... 69 Shirin Namouz-Haddad and Gideon Koren
11 Interstitial Pregnancy ... 77 Margaret Dziadosz, Ana Monteagudo
and Ilan E. Timor-Tritsch
12 Cervical Pregnancy ... 85 Abdulrahman Alserri and Togas Tulandi
13 Ovarian Ectopic Pregnancy ... 93 Warren J. Huber and Gary N. Frishman
14 Cesarean Scar Pregnancy ... 101 Marcos Cordoba, Ana Monteagudo
and Ilan E. Timor-Tritsch
15 Abdominal Pregnancy ... 109 Amanda Ecker MD and Richard Guido MD
16 Intramural Pregnancy ... 115 Maria Memtsa and Davor Jurkovic
17 Heterotopic Pregnancy ... 123 Mallory Stuparich and Kimberly A. Kho
18 Retroperitoneal Ectopic Pregnancy ... 131 Ana Monzo-Miralles, Alicia Martinez-Varea
and Antonio Pellicer
19 Ectopic Molar Pregnancy ... 139 Atif Zeadna and Togas Tulandi
viii Contents
ix
20 Rudimentary Uterine Horn Pregnancy... 145 Mette Petri Lauritsen and Marianne Johansen
21 Fertility After Tubal Ectopic Pregnancy ... 153 Perrine Capmas, Jean Bouyer and Hervé Fernandez
Index ... 163
xi
Contributors
Benny Almog MD Lis Maternity Hospital, Tel Aviv Sourasky Medical Center Affiliated to Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel
Abdulrahman Alserri MD McGill University Health Center, Montreal, QC, Canada
Ali Ardehali MD Acute Gynaecology, Early Pregnancy and Advanced Endosurgery Unit, Nepean Centre for Perinatal Care, Nepean Clinical School, Nepean Hospital, University of Sydney, Penrith, Sydney, Australia
Senem Ates MD McGill University Health Center, Montreal, QC, Canada
Shabnam Bobdiwala MD Queen Charlotte and Chelsea Hospital, Imperial College London, London, UK
Tom Bourne MD, PhD Queen Charlotte and Chelsea Hospital, Imperial College London, London, UK
Jean Bouyer MD Centre of research in Epidemiology and population health (CESP), Inserm, Le Kremlin Bicêtre, France Perrine Capmas MD Service de Gynécologie Obstétrique, Hôpital Bicêtre, GHU Sud, AP-HP, Le Kremlin Bicêtre Cedex, France Centre of research in Epidemiology and population health (CESP), Inserm, Le Kremlin Bicêtre, France
Univ Paris Sud, Le Kremlin Bicêtre, France
Lisa Caronia MD Cleveland Clinic, Cleveland, OH, USA Ishwari Casikar MD Acute Gynaecology, Early Pregnancy and Advanced Endosurgery Unit, Nepean Centre for Perinatal Care, Nepean Clinical School, Nepean Hospital, University of Sydney, Penrith, Sydney, Australia
George Condous MBBS, MD Acute Gynaecology, Early Pregnancy and Advanced Endosurgery Unit, Nepean Centre for Perinatal Care, Nepean Clinical School, Nepean Hospital, University of Sydney, Penrith, Sydney, Australia
Marcos Cordoba MD Department of Obstetrics and Gynecology, Division of Maternal Fetal Medicine, New York University School of Medicine, New York, NY, USA
Margaret Dziadosz MD Department of Obstetrics and Gynecology, New York University School of Medicine, New York, NY, USA Amanda Ecker MD Magee-Womens Hospital of UPMC, Pittsburgh, PA, USA
Tommaso Falcone MD Cleveland Clinic, Cleveland, OH, USA Hervé Fernandez MD, PhD. Service de Gynécologie Obstétrique, Hôpital Bicêtre, GHU Sud, AP-HP, Le Kremlin Bicêtre Cedex, France
Centre of research in Epidemiology and population health (CESP), Inserm, Le Kremlin Bicêtre, France
Univ Paris Sud, Le Kremlin Bicêtre, France BICETRE, Le Kremlin Bicetre, France
Rebecca Flyckt MD Cleveland Clinic, Cleveland, OH, USA Gary N. Frishman MD Women and Infants Hospital, Providence, RI, USA
Richard Guido MD Magee-Womens Hospital of UPMC, Pittsburgh, PA, USA
Warren J. Huber III, MD, PhD Women and Infants Hospital, Providence, RI, USA
Marianne Johansen MD Department of Obstetrics, Copenhagen University Hospital Rigshospitalet, Copenhagen, Denmark
Davor Jurkovic MD Department of Obstetrics and Gynecology, University College Hospital, London, UK
Gynaecology Diagnostic and Outpatient Treatment Unit,, University College Hospital, London, UK
Kimberly A. Kho MD, MPH Department of Obstetrics and Gynecology, University of Texas Southwestern Medical Center, Dallas, TX, USA
Gideon Koren MD The Hospital for Sick Children, Toronto, ON, Canada
Mette Petri Lauritsen MD The Fertility Clinic, Copenhagen University Hospital Rigshospitalet, Copenhagen, Denmark
Ishai Levin MD Lis Maternity Hospital, Tel Aviv Sourasky Medical Center Affiliated to Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel
Jillian Main MD Stanford University Medical Center, OBGYN, Palo Alto, CA, USA
Alicia Martinez-Varea MD Obstetrics & Gynecology, La Fe University Hospital, Valencia, Spain
Maria Memtsa MD Department of Obstetrics and Gynecology, University College Hospital, London, UK
Ana Monteagudo MD Department of Obstetrics and Gynecology, Division of Maternal Fetal Medicine, New York University School of Medicine, New York, NY, USA
Department of Obstetrics and Gynecology, New York University School of Medicine, New York, NY, USA
Ana Monzo-Miralles MD Obstetrics & Gynecology, La Fe University Hospital, Valencia, Spain
Shirin Namouz-Haddad MD The Hospital for Sick Children, Toronto, ON, Canada
xiii Contributors
Camran Nezhat MD Stanford University Medical Center, OBGYN, Palo Alto, CA, USA
Antonio Pellicer MD Obstetrics & Gynecology, La Fe University Hospital, Valencia, Spain
Shiri Shinar MD Lis Maternity Hospital, Tel Aviv Sourasky Medical Center Affiliated to Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel
Mallory Stuparich MD Department of Obstetrics and Gynecology, University of Texas Southwestern Medical Center, Dallas, TX, USA
Ilan E. Timor-Tritsch MD Department of Obstetrics and Gynecology, Division of Maternal Fetal Medicine, New York University School of Medicine, New York, NY, USA
Department of Obstetrics and Gynecology, New York University School of Medicine, New York, NY, USA
Togas Tulandi MD, MHCM McGill University Montreal, QC, Canada
M. Jean Uy-Kroh MD Department of Obstetrics and Gynecology, Women’s Health Institute, Cleveland Clinic, Cleveland, OH, USA Atif Zeadna MD McGill University Health Center, Montreal, QC, Canada
Soroka University Medical Center, Beersheba, Israel
1
Chapter 1
Identification of Risk Factors of Ectopic Pregnancy
Ali Ardehali, Ishwari Casikar and George Condous
© Springer International Publishing Switzerland 2015 T. Tulandi (ed.), Ectopic Pregnancy,
DOI 10.1007/978-3-319-11140-7_1 A. Ardehali () · I. Casikar · G. Condous
Acute Gynaecology, Early Pregnancy and Advanced Endosurgery Unit, Nepean Centre for Perinatal Care, Nepean Clinical School, Nepean Hospital, University of Sydney, Penrith, Sydney, Australia
e-mail: [email protected]
Case Study
The patient was a 29-year-old African-descent woman who presented to the emergency department (ED) with low abdominal pain and nausea. Her pain started 20 h prior to her presentation. The pain had gradually become worse and had radiated to her shoulder tip and was associated with increasing nausea. She had also expe- rienced some per vaginal (PV) spotting and a few episodes of diar- rhea during the previous 2–3 days. She initially thought she was starting to menstruate as she also had some breast tenderness. She had no history of abnormal PV discharge.
She smoked approximately 30 cigarettes per day and was a social drinker. She was currently not on any contraception as she was trying to conceive. She had commenced sexual activity at age of 16, with her first husband. She had had two vaginal births at 17 and 20 years of age. She admitted to having had multiple sexual partners from the age of 21 to 26 while she was divorced from her first husband. She had also had two surgical terminations for
unwanted pregnancies during that time. She had a laparoscopy at 23 years of age for a right-sided dermoid cyst and there had been evidence of pelvic inflammatory disease (PID). A vaginal swab taken at time confirmed chlamydia infection and she had been ap- propriately treated. She migrated to Australia from Africa, at the age of 21, as a refugee with her husband and two children.
On examination, she was noted to be pale, and appeared to be in moderate discomfort with a pulse of 102 beats per minute, blood pressure 98/54, afebrile, and saturating at 97 % on room air. Her body mass index (BMI) was 19. Apart from the three laparoscopic scars on her abdomen, she had tenderness, guarding, and rebound pain in the right iliac fossa. Speculum examination demonstrated small amount of blood at the cervical os. Bimanual examination revealed a significant right adnexal tenderness; she was uncomfort- able with cervical excitation.
Her hemoglobin (Hgb) was 100 g/L with microcytic and hypo- chromic picture, white blood cell (WBC) 11.6 × 109/L, and platelet count 286 × 109/L. A urinalysis was positive for blood, ketones, and human chorionic gonadotropin (hCG).
My Management
A. My clinical management is based mainly on physical examina- tion and not on history of risk factors.
B. Identification of risk factors alerts me to identify patients who are at risk to have an ectopic pregnancy (EP).
C. Knowing risk factors for EP is important for academic medicine and not for patient management.
Diagnosis and Assessment
In the last three decades, we have witnessed significant changes in the diagnosis and management of EP. The key factors contributing to this change are increased awareness of EPs, tertiary-level early
3
pregnancy units (EPUs), introduction of high-resolution transvagi- nal ultrasound probes and availability of accurate and rapid serum hCG assays [1]. However, EP is still the most common cause of pregnancy-related deaths and morbidity worldwide, and accounts for 54 % of first-trimester maternal deaths in the UK, and 3–4 % of all mortalities related to pregnancy [2, 3]. This is despite the fact that the mortality from EP has significantly dropped over the past few decades [4].
About 6–16 % of all women who present to an emergency de- partment with first-trimester bleeding or pain or both have EP [5].
Due to the nature of pathology of EP and the absence of a single di- agnostic test, early diagnosis can be challenging in emergency and general practice settings. In the most recent confidential enquiry into maternal deaths in the UK during 2006–2008, gastrointestinal symptoms, particularly diarrhea and dizziness in early gestation, are important indicators of EP. These features need to be empha- sized to all clinical staff in the primary-care setting [1]. Although transvaginal ultrasound scans (TVS) and the rapid availability of quantitative hCG levels have significantly improved the early di- agnosis and optimal management of EP [6–8], a high index of sus- picion of this condition in the first presentation remains the key to early diagnosis and achieving the best outcome.
Management
A detailed history along with a focused physical examination and a quick office test can guide the clinician toward early diagnosis of EP. Detailed TVS performed by an experienced operator can then confirm the diagnosis [9, 10].
The gradual onset of and progressive abdominal pain, and subsequent radiation to the shoulder tip, in addition to mild tachycardia, pallor, and abdominal examination findings, indicate intraperitoneal bleeding. More importantly, the occurrence of diar- rhea in the preceding 2–3 days is an important historical factor [2].
The patient’s past medical and surgical history revealed several risk factors, which suggested EP in the list of differential diagnoses.
1 Identification of Risk Factors of Ectopic Pregnancy
These risk factors are smoking, multiple sexual partners, laparo- scopic evidence of PID and confirmed chlamydia swab, and two surgical terminations of pregnancy (Fig. 1.1).
Differential Diagnosis
• Ectopic pregnancy
• Threatened or incomplete miscarriage
• Appendicitis
• Urinary tract infection
• Ovarian torsion
• Pelvic inflammatory disease
• Urinary calculus
• Gastroenteritis
• Ruptured or hemorrhagic ovarian cyst
Our patient had been trying to conceive for the last 6 months and now had a positive urine pregnancy test. Therefore, all the compli- cations of early pregnancy including ectopic and early miscarriage
Fig. 1.1 a Ultrasonographic image of tubal ectopic pregnancy (EP) with both embryonic pole and yolk sac visible within the gestational sac. b Same tubal EP demonstrating cardiac activity using M-Mode (viable EP)
5
should be considered. A quantitative serum hCG would be helpful to confirm the urine test and also as a tool to estimate the age of pregnancy along with the TVS. More importantly, serial serum hCG levels can be measured as well as TVS examination during the con- servative management and follow up of patients diagnosed with EP.
The mild tachycardia and relatively low blood pressure, in addition to abdominal tenderness, peritonitis, blood in vagina, and adnexal tenderness, are indicative of clinical instability and potential rup- ture of EP and the urgency of diagnosis and management.
Risk Factors for EP There are several studies published regard- ing EP and its risk factors. However, only about 50 % of women diagnosed with an EP have identifiable risk factors. Recognition of these risk factors can assist the clinicians not only in the early diag- nosis of EP but also in reducing the risk of morbidity and mortality of massive intra-abdominal hemorrhage. Most papers have catego- rized the risk factors to high, medium, and low risks, although there are variations depending on the epidemiology of the study. Below, we have reviewed the most widely accepted factors for EP. [11, 12].
Previous EP and Tubal Surgery Previous EP is one of the high risk factors and the incidence increases among people who have had a history of an EP. A woman who has had two prior EPs has a tenfold increased in future EP. This could be due to the tubal dysfunction as the main pathology or secondary to the treatment of EP. The recurrence rate of EP after surgical or nonsurgical management has been reported from 8 to 15 % and 15 % after conservative manage- ment [13, 14]. The risk of EP also increases in women who have had a history of any type of pelvic surgery. For example, previous appendectomy increases the risk of EP by twofold [15]. Among the group of women for whom tubal sterilization has failed, pregnancy can result in an EP rate as high as 33 %. Among these patients, the risk of EP is higher in those less than 30 years of age [13].
PID, Infections, and Multiple Sexual Partners The growing rate of EP is strongly associated with the increasing rate of PID. The incidence of EP increased by more than twofold from 1970 to 1985
1 Identification of Risk Factors of Ectopic Pregnancy
from 7 to 16 per 1000 and then declined by 30 % from 1985 to 1997. This was explained by the increase and decline of PID within those periods [16]. It has also been proven that having multiple sexual partners is a strong risk factor for EP with the odds ratio of 2.1 [17]; but the association between PID and number of sexual partners has to be considered [18, 19].
In a European study, 65 % of women with EP had suffered from tubal salpingitis. A history of tubal pathology or tubal surgery has been shown to increase the risk of EP with the odds ratio of 3.8–21.0 and 21.0, respectively [20]. Overall, the history of genital infections, including sexually transmitted disease, PID, and/or any tubal pathology or surgery, is a high risk factor for tubal EP.
Smoking There are several studies which have confirmed the increased risk of EP in smokers. The risk of EP increases by three- fold to fourfold in women who smoke more than one packet of cigarettes per day. The level of risk has been proven to be vari- able depending on the number of cigarettes smoked. Smoking more than 20 cigarettes a day increases the risk of EP more than smoking 1–5 cigarettes a day with the odds ratio 1.7–3.5 [14, 21, 22].
Infertility It has been proven that the duration of infertility is associated with increased risk of EP with an adjusted odd ratio of 2.7 for more than 2 years of infertility [21]. The rate of EP is 2–3 % higher in patients undergoing an in vitro fertilization (IVF) [20]. In addition, treatment with gonadotropin and other drugs such as clo- miphene in IVF pregnancy increases the incidence of EP. This can also be due to dysfunction of the fallopian tubes [23–26]. The rate of heterotopic pregnancy in the assisted reproductive population could be up to 1 in 100 to 1 in 45 [27, 28].
Other Causes There are other proven risk factors for EP such as diethylstilbestrol (DES) exposure, intrauterine contracep- tive devices, surgical termination of pregnancy, and age. In utero exposure to DES increases the relative risk of EP by 3.84. Intra- uterine contraceptive devices (IUCD) such as copper IUCD and Mirena intra-uterine system (IUS) decrease the risk of an EP, but if pregnancy does occur with the device in situ, the risk of EP is
7
higher. Of the 0.5 per 100 Mirena IUS users who become pregnant in 5 years (cumulatively), half are EPs. Regular vaginal douching three to four times per month can increase the risk of PID as a high risk factor for EP by three to four times. Women aged 35–44 years have three times risk of EP compared to younger women.
Surgical terminations of pregnancy, spontaneous miscarriages, and older age have all also been shown to increase the risk of EP [11, 21, 29–35].
Types of EP More than 90–98 % of EPs are tubal pregnancies. EP can also be found in the cervix, ovaries, interstitial tube, cesarean scar, the horn of a bicornuate pregnancy (cornual), or abdomen.
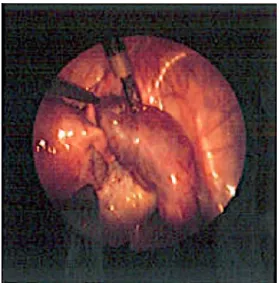
About 2–3 % of EPs are implanted in the interstitial portion of the tube (interstitial EP). If the ectopic is implanted in one horn of bicornuate uterus, it is called cornual. Of all EPs, 1 % is cervical, 1–3 % is ovarian, and 1–2 % is abdominal pregnancies. Cesarean scar EP is another rare type of EP, the incidence of which is increas- ing. [36–40] (Fig. 1.2).
Fig. 1.2 Laparoscopic image of right tubal ectopic pregnancy with significant hemoperitoneum
1 Identification of Risk Factors of Ectopic Pregnancy
Outcome
A TVS confirmed the diagnosis of a right-sided ruptured right tubal EP with blood noted in the pouch of Douglas and Morison’s pouch for which the patient had urgent laparoscopic salpingectomy.
Clinical Pearls/Pitfalls
• Failure to recognize the symptoms of an EP can result in in- creased morbidity and even mortality.
• Identification of risk factors for EP allows early detection and treatment.
• High risk factors include previous EP, previous tubal surgery, tubal damage, and current IUD use.
References
1. Casikar I, Condous G. How to effectively diagnose ectopic pregnancy using ultrasound? Expert Rev Obstet Gynecol. 2013;8(6):493–5.
2. Cantwell R, Clutton-Brock T, Cooper G, Dawson A, Drife J, Garrod D, et al.
Saving mothers’ lives: reviewing maternal deaths to make motherhood safer:
2006–2008. The eighth report of the confidential enquiries into maternal deaths in the United Kingdom. BJOG. 2011;118:1–203.
3. Centers for Disease Control and Prevention (CDC). Ectopic pregnancy—
United States, 1990–1992. JAMA 1995;7:533
4. Creanga AA, Shapiro-Mendoza CK, Bish CL, et al. Trends in ectopic pregnancy mortality in the United States: 1980–2007. Obstet Gynecol.
2011;117:837–43
5. Murray H, Baakdah H, Bardell T, Tulandi T. Diagnosis and treatment of ectopic pregnancy. CMAJ. 2005;173:905.
6. Condous G. The management of early pregnancy complications. Best Pract Res Clin Obstet GynaecoI. 2004;lB:37–57.
7. Condous G, Okaro E, Bourne T. The conservative management of early pregnancy complications: a review of the literature. Ultrasound Obstet GynecoI. 2003;22:420–30.
8. Condous G, Okaro E, Bourne T. The management ofectopic pregnancies and pregnancies of unknown location. Gynecol Surg. 2004;1:81–6.
9 9. Condous G, Okaro E, Khalid A, et al. The accuracy of transvaginal ultra-
sonography for the diagnosis of ectopic pregnancy prior to surgery. Hum Reprod. 2005;20:1404–9.
10. Condous, G. Ectopic pregnancy: risk factors and diagnosis [online]. Aust Fam Physician. 2006 Nov;35(11):854–7.
11. Farquhar CM. Ectopic pregnancy. Lancet 2005;366:583–91.
12. Ankum WM, Mol BW, van der Veen F, Bossuyt PM. Risk factors for ecto- pic pregnancy: a meta-analysis. Fertil Steril. 1996;65:1093–9. (Comment in Fertil Steril 1997;67:791–2).
13. Michalas S, Minaretzis D, Tsionou C, Maos G, Kioses E, Aravantinos D.
Pelvic surgery, reproductive factors and risk of ectopic pregnancy: a case controlled study. Int J Gynaecol Obstet. 1992;38:101–5.
14. Bouyer J, Coste J, Shojaei T, Pouly J, Fernandez H, Gerbaud L, Job-Spira N. Risk factors for ectopic pregnancy: a comprehensive analysis based on a large case-control, population-based study in France. Am J Epidemiol.
2003;157(3):185.
15. Yao M, Tulandi T. Current status of surgical and nonsurgical management of ectopic pregnancy. Fertil Steril. 1997;67:421.
16. Peterson HB, Xia Z, Hughes JM, et al. The risk of ectopic pregnancy af- ter tubal sterilization. U.S. Collaborative Review of Sterilization Working Group. N Engl J Med. 1997;336:762.
17. Kamwendo F, Forslin L, Bodin L, Danielsson D. Epidemiology of ectopic pregnancy during a 28-year period and the role of pelvic inflammatory disease. Sex Transm Infect. 2000;76:28
18. Kriebs JM, Fahey JO. Ectopic pregnancy. J Midwifery Womens Health.
2006;51:431–9.
19. Coste J, Job-Spira N, Fernandez H, et al. Risk factors for ectopic pregnancy: a case-control study in France, with special focus on infec- tious factors. Am J Epidemiol. 1991;133:839–49.
20. Weström L. Influence of acute pelvic inflammatory disease on fertility.
Am J Obstet Gynecol. 1975;121:707–13.
21. Pisarska MD, Carson SA, Buster JE. Ectopic pregnancy. Lancet.
1998;351:1115–20.
22. Saraiya M, Berg CJ, Kendrick JS, et al. Cigarette smoking as a risk factor for ectopic pregnancy. Am J Obstet Gynecol.1998;178:493.
23. Chow WH, Daling JR, Cates W Jr, et al. Epidemiology of ectopic preg- nancy. Epidemiol Rev. 1987;9:70–94.
24. Job-Spira N, Bouyer J, Pouly JL, et al. Fertility after ectopic pregnancy:
first results of a population-based cohort study in France. Hum Reprod.
1996;11:99–104.
25. Cohen J, Mayaux MJ, Guihard-Moscato ML, Schwartz D. In-vitro fer- tilization and embryo transfer: a collaborative study of 1163 pregnancies on the incidence and risk factors of ectopic pregnancies. Hum Reprod.
1986;1:255.
26. Gemzell C, Guillome J, Wang CF. Ectopic pregnancy following treatment with human gonadotropins. Am J Obstet Gynecol. 1982;143:761.
1 Identification of Risk Factors of Ectopic Pregnancy
27. McBain JC, Evans JH, Pepperell RJ, et al. An unexpectedly high rate of ectopic pregnancy following the induction of ovulation with human pitu- itary and chorionic gonadotrophin. Br J Obstet Gynaecol. 1980;87:5.
28. Molloy D, Deambrosis W, Keeping D, Hynes J, Harrison K, Hennessey J. Multiple-sited (heterotopic) pregnancy after in vitro fertilization and gamete intrafallopian transfer. Fertil Steril. 1990;53:1068–71.
29. Talbot K, Simpson R, Price N, Jackson SR. Heterotopic pregnancy. J Ob- stet Gynaecol. 2011;31(1):7–12
30. Goldberg JM, Falcone T. Effect of diethylstilbestrol on reproductive func- tion. Fertil Steril. 1999;72:1.
31. Backman T, Rauramo I, Huhtala S, Koskenvuo M. Pregnancy during the use of levonorgestrel intrauterine system. Am J Obstet Gynecol.
2004;190:50.
32. Xiong X, Buekens P, Wollast E. IUD use and the risk of ectopic pregnan- cy: a meta-analysis of case-control studies. Contraception. 1995;52:23.
33. Wølner-Hanssen P, Eschenbach DA, Paavonen J, et al. Association between vaginal douching and acute pelvic inflammatory disease. JAMA.
1990;263:1936.
34. Nybo Andersen AM, Wohlfahrt J, Christens P, et al. Maternal age and fetal loss: population based register linkage study. BMJ. 2000;320:1708.
35. Storeide O, Veholmen M, Eide M, et al. The incidence of ectopic preg- nancy in Hordaland County, Norway 1976–1993. Acta Obstet Gynecol Scand. 1997;76:345.
36. Backman T. Levonorgestrel-releasing intrauterine system in contracep- tion. Expert Rev Obstet Gynecol. 2009;4(3):239–44.
37. Fylstra DL. Ectopic pregnancy within a cesarean scar: a review. Obstet Gynecol Survey. 2002;57:537–43.
38. Flystra DL. Ectopic pregnancy not within the (distal) fallopian tube: etiol- ogy, diagnosis, and treatment. Am J Obstet Gynecol. 2012;206(4):289–99.
39. Zhang Y, Chen YS, Wang JJ, Lu ZY, Hua KQ. Analysis of 96 cases with cesarean scar pregnancy. Zhonghua Fu Chan Ke Za Zhi. 2010;45:664–8.
40. Bouyer J, Coste J, Fernandez H, Pouly JL, Job-Spira N. Site of ectopic pregnancy: a 10-year population-based study of 1800 cases. Hum Reprod.
2002;17:3224–30.
I. Levin () · S. Shinar
Lis Maternity Hospital, Tel Aviv Sourasky Medical Center Affiliated to Sackler School of Medicine, Tel Aviv University, 6 Weizmann St., 69234 Tel Aviv, Israel
e-mail: [email protected] S. Shinar
e-mail: [email protected]
Case Study
A 38-year-old patient was admitted for suspected ectopic pregnancy after in vitro fertilization (IVF) treatment for male factor infertility.
Three embryos were transferred 16 days prior to her admission.
Serum beta-hCG measurement 4 days before her admission was 3200 mIU/mL and repeat testing 2 days later demonstrated a beta- hCG level of 2980 mIU/mL. She was hemodynamically stable, with very mild right abdominal pain. Transvaginal ultrasound (TVUS) revealed enlarged ovaries with multiple corpora lutea and a small amount of fluid in the cul-de-sac. The right fallopian tube seemed distended. Beta-hCG level on admission was 3000 mIU/mL. With the possibility of a right ectopic pregnancy, the consulting gyne- cologist prescribed methotrexate.
© Springer International Publishing Switzerland 2015 11 T. Tulandi (ed.), Ectopic Pregnancy,
DOI 10.1007/978-3-319-11140-7_2
Chapter 2
Discriminatory Serum hCG Level for Ectopic Pregnancy
Ishai Levin and Shiri Shinar
My Management
a. Agree with the consulting gynecologist to administer methotrexate
b. Repeat serum hCG measurement and perform ultrasound in 2–3 c. Perform laparoscopydays
Diagnosis and Assessment
In women who conceive via assisted reproductive technique (ART), the risk for ectopic pregnancy may be increased as much as twofold [1]. These women are at risk for an ectopic gestation. Ultrasound find- ings of a gestational sac with a yolk sac, embryo, or cardiac activity outside the uterus provide a definite diagnosis of an ectopic pregnan- cy, and immediate treatment is justified. Our patient had a complex adnexal mass or fluid in the cul-de-sac; it suggests the probability of an ectopic pregnancy, but is not diagnostic [2]. When a pregnancy of unknown location (PUL) is diagnosed, the possibilities include an ab- normal intrauterine pregnancy (collapsed, aborted, or simply underde- veloped) or an ectopic pregnancy (too small for recognition by TVUS or aborted). The possibility of a heterotopic gestation should be enter- tained especially in pregnancies resulting from ART [3]. Only 7–20 % of the women with an initial diagnosis of a PUL will eventually be diagnosed with an extrauterine pregnancy [4].
The serum hCG level can assist in determining the location and normal development of a pregnancy. The levels can help determine whether an intrauterine sac should already be seen by ultrasound.
The cutoff for the diagnosis of an intrauterine pregnancy using transabdominal ultrasonography is 6000–6500 IU/L [5]. With the use for transvaginal transducers, the discriminatory zone for the diagnosis is 1500 IU/L. This threshold level depends on the experi- ence and skill of the examiner and the type of transducer used.
The reported sensitivity and specificity of hCG > 1000 IU/L in the detection of ectopic pregnancy when no intrauterine pregnancy
2 Discriminatory Serum hCG Level for Ectopic Pregnancy 13
is visible is 21.7 and 87.3 %; for an hCG level of > 1500 IU/L these values are 15.2 and 93.4 %, and for an hCG level of > 2000 IU/L they are 10.9 and 95.2 %, respectively [6]. Raising the threshold to 2000 IU/L increases the specificity and minimizes the number of false positive errors, but may also delay the diagnosis of an ecto- pic pregnancy. The contribution of TVUS when beta-hCG is be- low 1500 IU/L in diagnosing intra- and extrauterine pregnancies is small, with sensitivities of 33 and 25 %, respectively [7].
Serum hCG value above the discriminatory zone (1500 IU/L) and no intrauterine sac on TVUS strongly suggests an extrauterine pregnancy, but is still not diagnostic. Several possible scenarios are possible in such cases:
1. A complete abortion with rapidly declining beta-hCG levels.
2. An incomplete abortion with an indiscernible intrauterine sac.
3. A normally developing intrauterine multiple gestation. In women with an intrauterine multiple pregnancy, the serum hCG level could be higher than 1500 mIU and yet ultrasound examination would not reveal an intrauterine pregnancy. Previously, levels of over 9000 IU/L have been described for intrauterine triplet pregnancies unobserved by TVUS [8]. In this case, declining beta-hCG levels may be due to a poorly developed single gesta- tion in a multiple-gestation pregnancy.
4. A heterotopic pregnancy with a normally developing intrauter- ine pregnancy along with an extrauterine pregnancy.
5. Several additional factors can contribute to nonvisualization of an intrauterine singleton pregnancy with levels above the dis- criminatory value. These include obesity and intrauterine pathol- ogies, such as fibroids, adenomyosis, and endometrial polyps [8]. Accordingly, in minimally symptomatic women with a low risk for an ectopic pregnancy, even when the hCG level is above the discriminatory zone and no intrauterine pregnancy is visible on TVUS, a repeat hCG level in 2 days is recommended. This type of watchful waiting can decrease the number of patients treated with methotrexate unnecessarily. More importantly, it could be harmful to an intrauterine pregnancy [9].
In patients with a beta-hCG level below the discriminatory zone, the absence of an intrauterine sac is inconclusive. We recommend serial
measurements of hCG levels at 2-day intervals until the discriminatory zone is reached and the diagnosis is established [10]. Interassay varia- tion of hCG between different laboratories is up to 15 %.
Our patient had hCG values above the discriminatory value for intrauterine pregnancies. The probability of an ectopic pregnancy is high, but the possibility of a concomitant intrauterine pregnancy or a multiple gestation pregnancy cannot be ruled out (Figs. 2.1 and 2.2).
Management
The patient presented is hemodynamically stable and is mildly symptomatic, with minimal abdominal discomfort. TVUS fails to reveal a gestational sac, and the diagnosis of PUL should be made.
There is no need for an emergency laparoscopy and the early ad- ministration of methotrexate could be redundant and even harmful.
Fig. 2.1 Longitudinal view demonstrating regular thickened endometrium
2 Discriminatory Serum hCG Level for Ectopic Pregnancy 15
Repeating beta-hCG and performing TVUS if needed two days af- terwards would be the recommended course of action. Even if an extrauterine pregnancy becomes evident during follow-up, metho- trexate may or may not be the preferred treatment. According to a recent study performed by our group, 40 % of extrauterine pregnan- cies will resolve spontaneously with watchful waiting [11], making the administration of methotrexate redundant. By follow up with beta-hCG and TVUS several possibilities may arise:
1. Values of beta-hCG will rise and a multiple intrauterine preg- nancy will be seen on TVUS. In this scenario the administration of methotrexate may harm the developing fetuses, as this drug is teratogenic.
Fig. 2.2 Transverse view demonstrating intrauterine pseudosac and isth- mic tubal pregnancy to the left of the uterus. (These two ultrasound pictures (Figs. 2.1 and 2.2) were taken from the same patient. Longitudinal view dem- onstrates a normally appearing luteal phase endometrium while the transverse view reveals a pseudosac and a clearly visible ectopic pregnancy in the isthmic portion of the fallopian tube. With beta-hCG levels of 1500 IU/mL this ectopic pregnancy could easily have been missed. (Courtesy Arnon Agmon, MD)
2. Values of beta-hCG will rise and a heterotopic pregnancy is seen on TVUS. In this case the decision to treat conservatively versus surgical removal of the ectopic pregnancy depends on its loca- tion and the patient’s hemodynamic stability [12, 13].
3. Values of beta-hCG will rise and a repeated TVUS will reveal a tubal pregnancy without intrauterine pregnancy. In this case administration of methotrexate versus laparoscopic manage- ment will depend on hemodynamic stability, hCG value, and the existence of extrauterine cardiac activity.
4. Values of beta-hCG will rise above the discriminatory zone, but at an abnormal rate, and yet TVUS will remain inconclusive as to the location of the pregnancy. Here, medical treatment can be offered safely, but a presumed diagnosis of an extrauterine pregnancy will be inaccurate, making methotrexate treatment needless in 40 % of the cases [14].
5. Values of beta-hCG will plateau. Methotrexate administration should be considered.
6. Values of beta-hCG will steadily decrease. In the absence of any significant change in clinical status, expectant management by watchful waiting is the recommended treatment, with success rates of 90 and 60 % in women with hCG concentrations below 2000 IU/L and over 10,000 IU/L, respectively [15].
Outcome
The patient received an intramuscular injection of a single dose of methotrexate (day 0). On day 4, the serum hCG level was 5000 IU/L. An ultrasound was performed and to the gynecologist’s surprise, it revealed a heterotopic pregnancy with a right tubal cho- rionic sac and yolk sac and an intrauterine gestational sac. Due to the developing extrauterine gestation, a laparoscopic right salpin- gectomy was performed. Understanding the risks associated with methotrexate exposure during pregnancy, the patient opted to ter- minate the intrauterine pregnancy.
2 Discriminatory Serum hCG Level for Ectopic Pregnancy 17
Clinical Pearls/Pitfalls
• The discriminatory values of serum hCG for the diagnosis of an intrauterine pregnancy are not always reliable.
• Serum hCG value above the discriminatory zone and no intra- uterine sac on TVUS is not diagnostic of an extrauterine preg- nancy.
• When hCG level is above the discriminatory value of 1500 IU/L, but no intrauterine pregnancy is visible on TVUS, options such as a complete/incomplete abortion, multiple gestation, or het- erotopic gestation should be considered.
• Obesity and intrauterine pathologies can obscure an early intra- uterine pregnancy.
• A beta-hCG level below the discriminatory zone in the absence of an intrauterine sac is inconclusive. In hemodynamically sta- ble patients, repeated beta-hCG and TVUS exams are recom- mended.
• Interassay variation in beta-hCG values exists. In hemodynami- cally stable patients, serial values should be obtained before treatment is offered.
• Failure to recognize an intrauterine pregnancy may be more harmful than delaying diagnosis of an extrauterine pregnancy.
• Watchful waiting in patients with declining beta-hCG levels prevents redundant administration of methotrexate.
References
1. Marcus SF, Brinsden PR. Analysis of the incidence and risk factors asso- ciated with ectopic pregnancy following in-vitro fertilization and embryo transfer. Hum Reprod. 1995;10:199–203.
2. Gabrielli S, Romero R, Pilu G, Pavani A, Capelli M, Milano V, Bevini M, Bovicelli L. Accuracy of transvaginal ultrasound and serum hCG in the di- agnosis of ectopic pregnancy. Ultrasound Obstet Gynecol. 1992;2:110–5.
3. Clayton HB, Schieve LA, Peterson HB, Jamieson DJ, Reynolds, MA, Wright VC. A comparison of heterotopic and intrauterine-only pregnancy outcomes after assisted reproductive technologies in the United States from 1999 to 2002. Fertil Steril. 2007;87:303–9.
4. Kirk E, Papageorghiou AT, Condous G, Tan L, Bora S, Bourne T. The diagnostic effectiveness of an initial transvaginal scan in detecting ectopic pregnancy. Hum Reprod. 2007;22:2824–8.
5. Kadar N, DeVore G, Romero R. Discriminatory hCG zone: its use in the sonographic evaluation for ectopic pregnancy. Obstet Gynecol.
1981;58:156–61.
6. Condous G, Kirk E, Lu C, Van Huffel S, Gevaert O, De Moor B, De Smet F, Timmerman D, Bourne T. Diagnostic accuracy of varying discriminato- ry zones for the prediction of ectopic pregnancy in women with a pregnan- cy of unknown location. Ultrasound Obstet Gynecol. 2005;26(7):770–5.
7. Barnhart KT, Simhan H, Kamelle SA. Diagnostic accuracy of ultrasound above and below the beta-hCG discriminatory zone. Obstet Gynecol.
1999;94:583–7.
8. Ko JK, Cheung VY. Time to revisit the human chorionic gonadotropin discriminatory level in the management of pregnancy of unknown loca- tion. J Ultrasound Med. 2014;33(3):465–71.
9. Usta IM, Nassar AH, Yunis KA, Abu-Musa AA. Methotrexate embry- opathy after therapy for misdiagnosed ectopic pregnancy. Int J Gynaecol Obstet. 2007;99:253–5.
10. Ankum WM, Van der Veen F, Hamerlynck JV, Lammes FB. Suspected ec- topic pregnancy. What to do when human chorionic gonadotropin levels are below the discriminatory zone. J Reprod Med. 1995;40:525–8.
11. Cohen A, Zakar L, Gil Y, Amer-Alshiek J, Bibi G, Almog B, Levin I.
Methotrexate success rates in progressing ectopic pregnancies: a reap- praisal. Am J Obstet Gynecol. 2014;211(2):e1–5.
12. Baxi A, Kaushal M, Karmalkar H, Sahu P, Kadhi P, Daval B. Success- ful expectant management of tubal heterotopic pregnancy. J Hum Reprod Sci. 2010;3(2):108–10.
13. Eom JM, Choi JS, Ko JH, Lee JH, Park SH, Hong JH, Hur CY. Surgical and obstetric outcomes of laparoscopic management for women with het- erotopic pregnancy. J Obstet Gynaecol Res. 2013;39(12):1580–6.
14. Barnhart KT, Katz I, Hummel A, Gracia CR. Presumed diagnosis of ecto- pic pregnancy. Obstet Gynecol. 2002;100:505–10.
15. Shalev E, Peleg D, Tsabari A, Romano S, Bustan M. Spontaneous resolution of ectopic tubal pregnancy: natural history. Fertil Steril. 1995;63:15–9.
19
Chapter 3
Pregnancy of Unknown Location
Shabnam Bobdiwala and Tom Bourne
© Springer International Publishing Switzerland 2015 T. Tulandi (ed.), Ectopic Pregnancy,
DOI 10.1007/978-3-319-11140-7_3 S. Bobdiwala () · T. Bourne
Queen Charlotte and Chelsea Hospital, Imperial College London, Du Cane Rd., London W12 0HS, UK
e-mail: [email protected] T. Bourne
e-mail: [email protected]
Case Study
A 28-year-old woman was referred to the emergency department by her family practitioner after presenting with a 4-day history of left iliac fossa discomfort. The urinary pregnancy test was positive.
She stated that her last menstrual period (LMP) was 6 weeks ago.
She had a past history of chlamydia infection. Transvaginal ultra- sonography revealed a hypoechoic area within the uterine cavity measuring 4.3 mm in maximum diameter. This was interpreted as a pseudosac (Fig. 3.1). The patient was tender in the left iliac fossa during the scan, and the left ovary was not clearly visualized. On presentation, the serum hCG was 1600 mIU/mL, and 48 h later had increased to 2200 mIU/mL. The patient’s pain settled over this time period. It was felt that these findings were consistent with an ectopic pregnancy (EP) and methotrexate was given.
My Management
A. I agree with the management above
B. I would proceed to laparoscopy as the hCG is high C. I would repeat the transvaginal ultrasound scan D. I would carry out uterine curettage
E. I would repeat the serum hCG
Diagnosis and Assessment
A patient presenting with risk factors for EP (e.g. previous pelvic infection) should heighten suspicion. The greatest risk factor for an EP is tubal damage, which usually occurs after tubal surgery or fol- lowing a pelvic infection, particularly with Chlamydia trachomatis.
Others include smoking and conception following assisted repro- duction. However, it must be remembered that most EPs occur in women who do not have any risk factors [1]. Dating a pregnancy by LMP is helpful but not necessarily an accurate predictor of what
Fig. 3.1 An early intrauterine gestation sac misclassified as a pseudosac
3 Pregnancy of Unknown Location 21
to expect to see on an ultrasound scan [2]. A significant proportion of women are unsure of their dates or have irregular cycles. Fur- thermore, we know there are clinically relevant variations in the ovulation–implantation interval [3].
Transvaginal ultrasonography is the best imaging modality for investigating problems in early pregnancy, with > 70 % of EPs vi- sualized at presentation and > 90 % before surgery using this ap- proach [4]. The majority (60 %) of EPs will be identified as a small homogeneous mass (blob sign, Fig. 3.2) rather than the classically described ring or ‘bagel’ sign [5]. The concept of a ‘pseudosac’ is to some extent outdated and relates to a misinterpretation of the ul- trasound findings. A round or oval fluid-filled hypoechogenic col- lection in the uterus in a woman with a positive pregnancy test is more likely to be an early intrauterine gestation sac and should not be cited as evidence for the presence of an EP [6]. Great care should also be taken when performing a scan in women when the uterus is axial or in the presence of fibroids. Both can make it difficult to identify an early intrauterine gestation sac.
The case presented had a pregnancy of unknown location (PUL), not a confirmed EP. The correct management would have been to repeat the transvaginal ultrasound scan at an interval to see if the
Fig. 3.2 A homogeneous mass or ‘blob sign’—the commonest ultrasound fea- ture of an ectopic pregnancy
hypoechogenic area in the endometrial cavity could be definitively identified as an intrauterine pregnancy, or an EP mass visualized before considering methotrexate.
The modern management of PUL is based on assigning risk (low risk: failing PUL and viable intrauterine; high risk: EP) rather than locating the pregnancy. Such risk assessment may be carried using the hCG ratio (hCG at 48 h/hCG at 0 h), although we have recently shown the mathematical prediction model ‘M4’ based on the initial hCG and hCG ratio is effective in this context and out- performs single measurements of progesterone and the hCG ratio alone [7]. This model can be downloaded from: http://homes.esat.
kuleuven.be/~biomed/M4PUL/M4triage.htm.
When considering methotrexate administration, it is important to exclude a viable intrauterine pregnancy. Methotrexate can be safely given when an EP has been definitively visualized. How- ever, as most EPs are seen as a homogenous mass [5], false posi- tive test results are possible. Accordingly, waiting 48 hours and reviewing the hCG ratio prior to methotrexate administration can significantly reduce the risk of inadvertent termination. A serum hCG rise of < 35 % is highly unlikely to be associated with a viable intrauterine pregnancy [8]. In this case, the rise in serum hCG of 37.5 % should have alerted the clinical team that the presence of a viable intrauterine pregnancy is potentially possible. A further safe- guard prior to methotrexate administration is to ensure a clinician who has specific expertise in early pregnancy imaging has repeated the ultrasound scan.
Historically, it was felt that a viable pregnancy would result in a doubling of serum hCG levels, a failing pregnancy, a halving of serum hCG levels and an EP, a ‘suboptimal rise’ in serum hCG after 48 hours. This does not, however, necessarily aid the clinician in determining the location of the pregnancy as EPs may demon- strate a ‘doubling’ or ‘halving’ of the serum hCG. In contrast, 8 % of viable intrauterine pregnancies have been found to demonstrate a ‘suboptimal rise’ in hCG levels, as seen in this case [8]. In any event, management is based on risk assessment. If the serum hCG is falling, the pregnancy will fall into the low-risk category irre- spective of whether it is in the uterine cavity.
3 Pregnancy of Unknown Location 23
Management
In a woman with a PUL and a serum hCG of > 2000 mIU/mL, the most likely diagnosis is not an EP but a non-viable intrauterine pregnancy. Similarly, a viable intrauterine cannot be entirely ex- cluded when the serum hCG is > 2000 mIU/mL [1]. Accordingly, methotrexate should not be given solely on the basis of there be- ing a PUL with an initial hCG above this level [2]. In the event of a stable visualized EP, it is sensible to delay decisions about treatment until a second serum hCG result is available 48 hours later. Information given by the hCG ratio will allow the clinician to know if a viable intrauterine pregnancy is a possibility. In the event that the hCG level is falling, expectant management may also be an option, thus avoiding medical intervention altogether. Giving methotrexate as a first line treatment without taking these precau- tions may be hazardous.
The consequences of missing the diagnosis of a wanted intra- uterine pregnancy are potentially far greater than delaying the diag- nosis of an EP in a haemodynamically stable patient. The absolute serum hCG level does not predict the likelihood of rupture [9], and most patients who are haemodynamically stable can be safely man- aged either expectantly or medically.
In relation to uterine curettage, current evidence suggests that there is a limited role for uterine curettage as a diagnostic tool in women who are classified as having a PUL [10]. The concern is that there may be inadvertent termination of wanted pregnancies.
It is important to be aware that the rise in hCG that is incompatible with a possible intrauterine pregnancy may be as low as ≤ 15 % over 48 h [10]. This is a different context to using uterine curet- tage in the small cohort of women classified as having a ‘persistent PUL’, where serum hCG levels persistently fail to decline (over
≥ 3 serial serum hCG measurements). Using uterine curettage in this circumstance to confirm the absence of chorionic villi within the uterine cavity before giving methotrexate is reasonable. How- ever, false negatives can occur; for example, chorionic villi are not detected by histopathology in 20 % of curettage specimens from elective termination of pregnancy.
Outcome
The patient received a single dose of intramuscular methotrexate (50 mg/m2 body surface). Subsequent ultrasonography 14 days lat- er demonstrated an intrauterine gestation sac with a yolk sac. Both ovaries were seen and appeared normal with no adnexal masses.
The pregnancy was followed up for the next 4 weeks and ultimately miscarried. The patient took legal action against the gynaecologist and the hospital.
Clinical Pearls/Pitfalls
• Most EPs are in women who have no risk factors.
• Dating a pregnancy by the last menstrual period is not an accu- rate predictor of ultrasound findings.
• A round or oval fluid-filled collection in the uterus is more like- ly to be an early intrauterine gestation sac than a pseudosac.
• A suboptimal rise in the serum hCG level is not diagnostic of an
• A serum hCG level of EP. > 2000 mIU/mL should not be used as an indication of the presence of an EP. It is more likely to represent an intrauterine pregnancy and does not exclude viability.
• Most EPs (> 70 % on initial presentation and > 90 % before final treatment) should be visualized on transvaginal ultrasonography.
Most EPs (60 %) are seen as homogenous masses or ‘blobs’.
• The management of PUL is based on assigning risk and not nec- essarily locating the pregnancy.
• In the event of a stable EP, it is sensible to repeat the hCG after 48 hours before considering treatment.
• If the hCG ratio does not exclude a viable intrauterine pregnan- cy, a repeat ultrasound scan may be carried out to ensure there is certainty about the diagnosis.
• If the hCG is declining, expectant management may be chosen, avoiding the need for methotrexate.
• The serum hCG level does not predict the likelihood of rupture of an EP.
3 Pregnancy of Unknown Location 25
• There is a limited role for uterine curettage as a diagnostic tool in women with a PUL.
• Uterine curettage is reasonable prior to management with meth- otrexate in patients classified with a ‘persistent PUL’.
Acknowledgment Tom Bourne is supported by the NIHR Biomedical Research Center based at Imperial College Healthcare NHS Trust and Imperial College London. The views expressed are those of the author(s) and not neces- sarily those of the NHS, the NIHR or the Department of Health.
References
1. Kirk E, Bottomley C, Bourne T. Diagnosing ectopic pregnancy and current concepts in the management of pregnancy of unknown location. Hum Re- prod Update. 2014;20(2):250–61.
2. Doubilet PM, Benson CB, Bourne T, Blaivas M. Society of Radiologists in Ultrasound Multispecialty Panel on Early First Trimester Diagnosis of Miscarriage and Exclusion of a Viable Intrauterine Pregnancy, Barnhart KT, Benacerraf BR, Brown DL, Filly RA, Fox JC, Goldstein SR, Kend- all JL, Lyons EA, Porter MB, Pretorius DH, Timor-Tritsch IE. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med.
2013;369(15):1443–51. doi:10.1056/NEJMra1302417.
3. Mahendru AA, Daemen A, Everett TR, Wilkinson IB, McEniery CM, Ab- dallah Y, Timmerman D, Bourne T, Lees CC. Impact of ovulation and im- plantation timing on first-trimester crown-rump length and gestational age.
Ultrasound Obstet Gynecol. 2012;40(6):630–5. doi:10.1002/uog.12277.
4. Kirk E, Papageorghiou AT, Condous G, Tan L, Bora S, Bourne T. The di- agnostic effectiveness of an initial transvaginal scan in detecting ectopic pregnancy. Hum Reprod. 2007;22(11):2824–8. (Epub 2007 Sep 13).
5. Brown DL, Doubilet PM. Transvaginal sonography for diagnosing ectopic pregnancy: positivity criteria and performance characteristics. J Ultrasound Med. 1994;13(4):259–66.
6. Barnhart K, van Mello NM, Bourne T, et al. Pregnancy of unknown lo- cation: a consensus statement of nomenclature, definitions, and outcome.
Fertil Steril. 2011;95:857–66.
7. Guha S, Ayim F, Ludlow J, Sayasneh A, Condous G, Kirk E, Stalder C, Timmerman D, Bourne T, Van Calster B. Triaging pregnancies of unknown location: the performance of protocols based on single serum progesterone or repeated serum hCG levels. Hum Reprod. In press 2014.
8. Seeber BE. What serial hCG can tell you, and cannot tell you, about an early pregnancy. Fertil Steril. 2012;98(5):1074–7. doi:10.1016/j.fertn- stert.2012.09.014. (Epub 2012 Sep 29). Review.
9. Galstyan K, Kurzel R. Serum beta-hCG titers do not predict ruptured ec- topic pregnancy. Int J Fertil Women Med. 2006;51:14–6.
10. Condous G, Kirk E, Lu C, Van Calster B, Van Huffel S, Timmerman D, Bourne T. There is no role for uterine curettage in the contemporary di- agnostic workup of women with a pregnancy of unknown location. Hum Reprod. 2006;21(10):2706–10. (Epub 2006 Jun 21).
27
Chapter 4
Ectopic Pregnancy After In Vitro Fertilization
Lisa Caronia, Rebecca Flyckt and Tommaso Falcone
© Springer International Publishing Switzerland 2015 T. Tulandi (ed.), Ectopic Pregnancy,
DOI 10.1007/978-3-319-11140-7_4 L. Caronia () · R. Flyckt · T. Falcone Cleveland Clinic, Cleveland, OH, USA e-mail: [email protected]
R. Flyckt
e-mail: [email protected] T. Falcone
e-mail: [email protected]
Case Study
A 38-year-old primigravida with a 2-year history of primary in- fertility presented for her first pregnancy ultrasound after in vitro fertilization (IVF) with day 5 embryo transfer (ET). The patient had a history of tubal factor infertility secondary to endometriosis, with left tubal obstruction identified on the initial hysterosalpin- gogram. She underwent laparoscopic left salpingolysis with hys- teroscopic left tubal cannulation and chromopertubation 4 months earlier. Her IVF cycle was uncomplicated and two embryos were transferred on day 5 of development. Two weeks later, she had a positive pregnancy test with serum human chorionic gonadotropin (hCG) of 1238 mU/mL. A second hCG level measured 1 week later was 9870 mU/mL. The patient was scheduled for an ultrasound at 7 weeks gestational age, correlating with approximately 4 weeks af- ter IVF-ET. A transvaginal ultrasound (TVUS) revealed a singleton
intrauterine pregnancy, as well as an extrauterine gestational sac with a fetal pole in the left adnexa. The patient’s infertility doctor was notified of the abnormal pregnancy and a decision was made to proceed with laparoscopic removal of the tubal pregnancy.
My Management
A. Agree with performing laparoscopy B. Perform ultrasound-guided local injection
C. Expectant management with hCG and TVUS in 2–3 days
Diagnosis and Assessment
Our patient has multiple factors which increase the risk of ecto- pic pregnancy, including history of infertility, tubal surgery, and advancing age. In one study, the authors reported that the risk of ectopic pregnancy among infertile women was double than that in fertile women [1]. Tubal factor infertility, as in this patient’s his- tory, is a predominant risk factor. It could be due to pelvic inflam- matory disease, abnormal tubal anatomy, or damage from a previ- ous ectopic pregnancy or surgery. These factors affect the ability of an embryo to successfully migrate to the uterus, increasing the risk of extrauterine implantation. Pregnancies as a result of ovulation- inducing therapies are also associated with increased risk of ectopic pregnancy [2]. It is possible that it is due to changes in tubal trans- port function; however, multiple confounding variables make a true association difficult to establish. IVF has also been associated with an increased risk of ectopic pregnancy.
The incidence of ectopic pregnancy after IVF was previously reported to be 2–11 %. Recent studies show that the rate is much lower (0.7 %) [1, 3]. Perhaps, it is related to improvements in many aspects of IVF techniques, including ET under ultrasound guidance, practice catheterization, utilization of minimal transfer
4 Ectopic Pregnancy After In Vitro Fertilization 29
media, and avoidance of deep catheter insertion. Recent research has also demonstrated that the incidence of ectopic pregnancy is no different in fresh versus frozen IVF-ET cycles, as well as with donor eggs versus standard IVF [4, 5]. Tubal surgery can have a dichotomous impact on ectopic pregnancy occurrence; although tubal surgery is a known risk factor for ectopic, in some cases, tubal surgery may actually help to reduce ectopic risk (e.g., in patients who have a hydrosalpinx removed or a damaged tube repaired or freed from adhesions). Lastly, the risk of ectopic pregnancy pro- gressively increases as women age, with a significantly higher in- cidence of extrauterine pregnancy in women more than 35 years of age as compared to their younger counterparts [6].
In fertility population, close monitoring with serial hCG levels and TVUS is standard and can help to detect ectopic pregnancy at an early stage. However, early monitoring increases the likeli- hood of an initial pregnancy of unknown location diagnosis, which can make proper management decisions challenging. With assisted reproductive technologies (ART) and the increased prevalence of multiple gestations, serial hCG levels may be less helpful, as early rises in hCG measurements may not follow accepted norms.
Heterotopic pregnancy, which classically occurs in 1/30,000 pregnancies [7], is now on the rise due to the increased use of ART.
Current estimates of heterotopic pregnancy are 1 per 4000 preg- nancies and can be as high as 1 per 100 to 1 per 1000 pregnancies in women undergoing ovulation induction or IVF [8–10]. Similar to ectopic pregnancy, TVUS has a high sensitivity for heterotopic diagnosis after IVF-ET when performed by an experienced ultraso- nographer. Even after seeing an intrauterine pregnancy, one should always examine the adnexas carefully, especially in IVF pregnancy.
Management
The general management principles for ectopic pregnancy also ap- ply to ectopic pregnancy after IVF. However, in the presence of an intrauterine pregnancy, practitioners should choose the treat- ment for the extrauterine gestation that will pose the least risk to
the developing intrauterine fetus. Expectant management is not a feasible strategy, given the inability to reliably monitor with serial hCG levels and TVUS. Methotrexate is not a suitable therapy, as it would be toxic to the viable intrauterine pregnancy. Ultrasound- guided local injection of either hyperosmolar glucose or potassium chloride is an alternative to surgery. There are also several reports in the literature of successful TVUS-guided aspiration of gestation- al sac content before injection of those agents [1]. This procedure can be performed in the outpatient setting and is of low risk to the concurrent intrauterine pregnancy. It is important to note that lo- cal injection of methotrexate is not a suitable agent for heterotopic pregnancy, as it maintains systemic effects [11]. The treatment of choice is laparoscopy with salpingectomy or salpingostomy. It is efficacious and can also be used for patients with hemodynamic instability or signs of tubal rupture. Laparoscopy permits evacua- tion of the extrauterine pregnancy without disturbing the intrauter- ine pregnancy. Salpingostomy can be performed for an unruptured ampullary ectopic, whereas salpingectomy may be more suitable if extensive damage of the involved tube is identified intraoperatively and there is a relatively normal-appearing contralateral fallopian tube. Proper preoperative counseling with patients regarding pos- sible intraoperative scenarios is imperative.
Outcome
The patient underwent a successful laparoscopic salpingostomy without complications. Subsequently, she delivered a full-term male infant by cesarean section. The tubes appeared to be normal at surgery. A hysterosalpingogram 1 year after her delivery was normal, with bilateral spill of contrast material into the abdominal cavity. She then conceived spontaneously 18 months after the birth of her son, delivered at term by repeat cesarean section.
4 Ectopic Pregnancy After In Vitro Fertilization 31
Clinical Pearls/Pitfalls
• Infertility, especially tubal factor infertility, is associated with increased risk of ectopic pregnancy.
• Ectopic pregnancy rates are now estimated to be at 0.7 % of all pregnancies achieved through IVF, likely related to improved ET techniques.
• TVUS has a high sensitivity for the diagnosis of ectopic after IVF-ET. Due to the increased risk of multiple pregnancies with ART, serial hCG alone may be difficult to interpret.
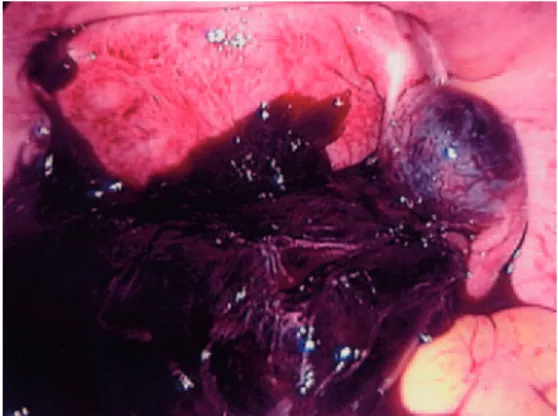
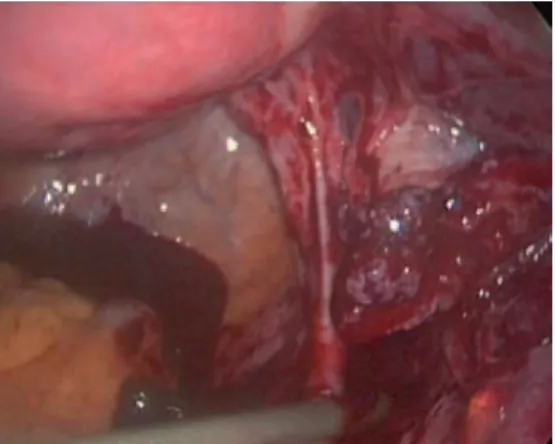
• Management strategies of heterotopic pregnancy include lapa- roscopy as well as ultrasound- guided local injection of hyper- osmolar glucose or potassium chloride. Decisions for manage- ment should be made on individualized basis dependent upon the clinical context (Fig. 4.1).
Fig. 4.1 Tubal ectopic pregnancy
References
1. Marcus SF, Brinsden PR. Analysis of the incidence and risk factors asso- ciated with ectopic pregnancy following in-vitro fertilization and embryo transfer. Hum Reprod. 1995;10(1):199–203.
2. Fernandez H, Coste J, Job-Spira N. Controlled ovarian hyperstimulation as a risk factor for ectopic pregnancy. Obstet Gynecol. 1991;78(4):656–9.
3. Centers for Disease Control and Prevention. Assisted reproductive tech- nology success rates. In: National Summary and Fertility Clinic Reports 2009. Atlanta, GA; 2007.
4. Decleer W, Osmanagoglu K, Meganck G, Devroey P. Slightly lower in- cidence of ectopic pregnancies in frozen embryo transfer cycles versus fresh in vitro fertilization-embryo transfer cycles: a retrospective cohort study. Fertil Steril. 2014;101(1):162–5.
5. Rosman ER, Keegan DA, Krey L, Liu M, Licciardi F, Grifo JA. Ectopic pregnancy rates after in vitro fertilization: a look at the donor egg popula- tion. Fertil Steril. 2009;92(5):1791–3.
6. Nybo Andersen A, Wohlfahrt J, Christens P, Olsen J,