Occupational Health Nursing
Third Edition
Edited by
Katie Oakley
John Wiley & Sons, Ltd
iii
www.ebook3000.com
ii
www.ebook3000.com
Occupational Health Nursing
i
www.ebook3000.com
ii
www.ebook3000.com
Occupational Health Nursing
Third Edition
Edited by
Katie Oakley
John Wiley & Sons, Ltd
iii
www.ebook3000.com
CopyrightC 2008 John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex PO19 8SQ, England
Telephone (+44) 1243 779777
Email (for orders and customer service enquiries): [email protected] Visit our Home Page on www.wiley.com
All Rights Reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, scanning or otherwise, except under the terms of the Copyright, Designs and Patents Act 1988 or under the terms of a licence issued by the Copyright Licensing Agency Ltd, 90 Tottenham Court Road, London W1T 4LP, UK, without the permission in writing of the Publisher. Requests to the Publisher should be addressed to the Permissions Department, John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex PO19 8SQ, England, or emailed to [email protected], or faxed to (+44) 1243 770620.
Designations used by companies to distinguish their products are often claimed as trademarks. All brand names and product names used in this book are trade names, service marks, trademarks or registered trademarks of their respective owners. The Publisher is not associated with any product or vendor mentioned in this book.
This publication is designed to provide accurate and authoritative information in regard to the subject matter covered. It is sold on the understanding that the Publisher is not engaged in rendering professional services. If professional advice or other expert assistance is required, the services of a competent professional should be sought.
Other Wiley Editorial Offices
John Wiley & Sons Inc., 111 River Street, Hoboken, NJ 07030, USA Jossey-Bass, 989 Market Street, San Francisco, CA 94103-1741, USA Wiley-VCH Verlag GmbH, Boschstr. 12, D-69469 Weinheim, Germany
John Wiley & Sons Australia Ltd, 42 McDougall Street, Milton, Queensland 4064, Australia
John Wiley & Sons (Asia) Pte Ltd, 2 Clementi Loop #02-01, Jin Xing Distripark, Singapore 129809
John Wily & Sons Canada Ltd, 6045 Freemont Blvd, Mississauga, ONT, L5R 4J3, Canada Wiley also publishes its books in a variety of electronic formats. Some content that appears in print may not be available in electronic books.
Library of Congress Cataloging-in-Publication Data
Occupational health nursing / edited by Katie Oakley. – 3rd ed.
p. ; cm.
Includes bibliographical references and index.
ISBN 978-0-470-03553-5 (cloth : alk. paper) 1. Industrial nursing. I. Oakley, Katie.
[DNLM: 1. Occupational Health Nursing–organization & administration. WY 141 O14 2008]
RC966.O332 2008
610.7346–dc22 2007036430
British Library Cataloguing in Publication Data
A catalogue record for this book is available from the British Library ISBN 9780470035535
Typeset in 10/12pt Palatino by Aptara Inc., New Delhi, India.
Printed and bound in Singapore by Markono Print Media Pte Ltd.
This book is printed on acid-free paper responsibly manufactured from sustainable forestry in which at least two trees are planted for each one used for paper production.
iv
www.ebook3000.com
Contents
Contributors vii
Foreword to the Third Edition by Professor
Dame Carol Black ix
Foreword to the Second Edition by Nola Ishmael x Foreword to the First Edition by Carol Bannister xi
Preface to the Third Edition xii
Introduction The Role of the Occupational Health Nurse 1 Daphne Bagley; Updated by Katie Oakley
PART I MANAGEMENT 25
Chapter 1 Setting Up Services 27
Anne Kennaugh
Chapter 2 Writing Policies and Procedures 43
Andrea Mummery and Katie Oakley
Chapter 3 Managing Services 65
Cynthia Atwell; Updated by Anna M. Cosgrove
Chapter 4 Quality and Audit 87
Linda Maynard
Chapter 5 Independent Practice 105
Kit Artus; Updated by Katie Oakley
Chapter 6 Marketing 119
Janette Murray
www.ebook3000.com
vPART II INTERNATIONAL ISSUES 137
Chapter 7 International Issues 139
Panayota Sourtzi
PART III PRACTICE 157
Chapter 8 Occupational Health and Safety 159
Katie Oakley
Chapter 9 Health Surveillance, Health Assessment and Health Screening 179 Cynthia Atwell
Chapter 10 Mental Health and Stress 197
Angela Franklin
Chapter 11 Musculoskeletal Disorders and Ergonomics 217 Claire Raistrick
Chapter 12 Health Promotion 237
Tracy McFall; Updated by Katie Oakley
Chapter 13 Rehabilitation 253
Dorothy Ferguson
Chapter 14 Case Management 271
Philip Roy Richardson
PART IV EDUCATION AND RESEARCH 291
Chapter 15 Education, Clinical Supervision and Professional Development 293 Patience D. Kenny
Chapter 16 Research 313
Jan Maw and Stuart Whitaker
Index 331
www.ebook3000.com
Contributors
Contributors to the Third Edition
Cynthia ATWELL (RN, OHNC, CertEd) Independent Occupational Health Consultant
Anna M. COSGROVE (RN, BSc (Hons), MSc Occupational Health) Occupational Health Nurse Consultant, University Hospital of North Staffordshire NHS Trust
Dorothy FERGUSON (RN, PhD, BA (Hons), MPH, SCM, RHV, OHNC, HVT, EdD)
MSc Co-ordinator, Department of Nursing and Community Health, Glasgow Caledonian University
Angela FRANKLIN (RN, MSc, DMS, OHNDip, Health Ed Cert) Occupational Health Service Manager, University College London Anne KENNAUGH (RN, MBA, RM, OHNC, MIOSH)
Resource Development Director, Grosvenor Health Ltd Patience D. KENNY (OHNC, MSc, PGCEA)
Formerly Teaching Fellow in Occupational Health, University of Surrey Jan MAW (RN, OHNC, DHP, M(Med)Sc, PGCE)
Lecturer in Occupational Health, University of Sheffield Linda MAYNARD (RN, ONC, DOHN, BSc (Hons), MSc) COPE OH & Ergonomic Services OH Manager to EDF Energy
vii
Andrea MUMMERY (RN, OHNC, Management Diploma) Occupational Health Manager, Nuffield Hospitals
Janette MURRAY (RN, BA, OHND, NEBOSH Cert) Director of Scottish Region, WellWork Ltd
Katie OAKLEY (RN, OHNC, BA (Hons), MA (Social Research)) Independent Occupational Health Adviser
Claire RAISTRICK (MSc, BA, RN, SCPHN(OH), MErgS, Eur Erg, CMIOSH)
Senior Teaching Fellow, University of Warwick Occupational Ergonomist, Matrick Ergonomics Ltd Philip Roy RICHARDSON (RN, BSc(Hons)) Occupational Health Adviser, IBM UK Ltd Panayota SOURTZI (RN, PhD)
Assistant Professor (OHN), Department of Public Health, Faculty of Nursing, University of Athens
Stuart WHITAKER (RN, RMN, OHNC, MIOSH, M(Med)Sc (Occupational Health), PhD)
Senior Lecturer in Occupational Health, St Martin’s College Lancaster
Contributors to Previous Editions
Kit ARTUS, Director, Cheviot Artus plc
Daphne M. BAGLEY, Occupational Health Adviser, Healthcare and Education Consultancy
Tracy McFALL, Specialist Practitioner OH, News International
Charles McK GRAHAM, HM Inspector of Health and Safety (Occupational Health), HSE
Foreword to the Third Edition
This publication provides a most useful tool for occupational health nurses, and highlights the real breadth and depth of issues which they deal with on a daily basis. It is refreshing to see these issues brought together into one publication; and the fact that the first edition was published over 10 years ago shows not only the ongoing popularity of the publication, but also its practicality and enduring relevance.
Occupational Health Nursing – Third Edition has been published in the same year as my Review of the Health of the Working Age Population.
This Review has reinforced my conviction of the pivotal role that occupational health must play in keeping people healthy and in work, or returning them to work as quickly as possible if they leave the work- place.
Occupational health has the opportunity to redefine its relationship in the delivery of health care, and map out how it will meet the chal- lenges of the future and be increasingly relevant to modern workplaces – occupational health nurses will obviously play a vital role in this.
I am honoured to be involved with Occupational Health Nursing – Third Edition, and look forward to seeing many more editions over the coming years.
Professor Dame Carol Black DBE FRCP FMedSci National Director for Health and Work
ix
Foreword to the Second Edition
Over the last five years I have been very privileged to work with occupational health nurses in a number of areas and initiatives through my role of policy development Nursing Officer for occupational health nursing. It has truly been an informative and enjoyable period in which much learning and sharing have taken place. At all times I have been inspired by the dedication, zest and energy, together with the depth of knowledge and range of experience, of the nurses who make up this branch of nursing.
As individual, economic and professional horizons change within society, so do the expectations of people, including those in the work- place. It therefore follows that the knowledge and expertise of occupa- tional health nurses must continue to increase to meet new challenges, deal with developments and act on requirements as they continue to deliver an evidence-based service.
Occupational Health Nursing – Second Edition is a welcome and timely resource which will assist occupational health nurses to develop a strong knowledge base in their field of practice. The modernised world of work demands similar modernised thinking and approaches. Occupa- tional Health Nursing – Second Edition allows readers to look back on the past and retain the lessons from it, to address the present and make it meaningful for themselves, the workforce and employers, and to look forward to the future with renewed assurance and confidence.
I am delighted to be associated with this work and commend it to you.
Nola Ishmael OBE Nursing Officer Department of Health, London
x
Foreword to the First Edition
Books on occupational health nursing are rare, and so it is all the more important that a new book on occupational health nursing should be by nurses and for nurses. Occupational health nursing is in the process of rapid development. New challenges face practitioners. Changes in patterns of work, legislation and education mean that the occupational health nurse needs to be responsive to and able to manage change.
Changes in nursing and nurse education have produced a new kind of occupational health nurse. Occupational health nurses have to show constant reflection on and improvement in practice, and to demonstrate this through professional portfolios to the UKCC, for continuing their ac- tive nurse registration. In addition the new degree programmes produce nurses who challenge practices which are ritualistic and not grounded in research. These practice and educational policy changes were essen- tial to ensure that occupational health nurses grow in confidence and ability and develop innovative approaches to practice, and offer employ- ers and employees the best possible advice and support in reducing the risk of harm from work. UK legislation in health and safety at work now promotes a risk management and risk reduction framework to solving problems in occupational health.
The world of business has also changed and the need for the occu- pational health nurse to show how the speciality of occupational health nursing ‘adds value’ to the purpose of the business is essential. While maintaining traditional values of nursing, the nurse must articulate and demonstrate the benefits of nursing practice to both employers and employees.
This book is for all occupational health nurses who wish to develop quality initiatives and deliver a research-based service.
Carol Bannister Adviser in Occupational Health Royal College of Nursing, London xi
Preface to the Third Edition
My original proposal to the publishers was to write a practical occupa- tional health nursing policy manual – full of templates that people could adapt for local use. Having sent the proposal out for review, the pub- lishers came back wanting something rather different. They asked me to put together and edit a multi-contributor reader on topics of interest to occupational health nurses, and Occupational Health Nursing was the result. It is more than 10 years now since the first edition of Occupational Health Nursing was published. The positive feedback and suggestions received, in particular from students of occupational health nursing and their tutors, have been most welcome and kept up the impetus to de- velop and refine the book. Occupational Health Nursing – Third Edition is three times the size of the first edition.
Occupational Health Nursing is edited and written entirely by occupa- tional health nurses and the focus remains on practical topics relevant to day-to-day practice in the workplace. Contributors have reviewed, revised and updated existing chapters, following appraisal of the latest literature and research and wide consultation with other expert col- leagues. There are also two excellent new chapters on highly topical subjects: ‘Case Management’ by Philip Roy Richardson and ‘Muscu- loskeletal Disorders and Ergonomics’ by Claire Raistrick.
The contributors share what has worked for them and their clients in practice – illustrating this with examples and sample documentation where possible. They are all familiar with the challenges of setting up and managing services, and with tailoring services to suit the needs of the employer and the employees of an organisation without compro- mising the quality of service.
Why become an occupational health nurse? It’s a wonderfully var- ied job presenting opportunities to work with people from the ‘shop floor’ to board level and in a range of settings, from hospitals, prisons xii
and laboratories, to oil rigs, to multi-national banks. There is a shortage of qualified occupational health nurses and there are therefore plenty of opportunities available. The contributors know how frustrating the job can be at times but recognise that being a good occupational health nurse means staying focused on and committed to the overall aim of helping make the workplace a healthier and safer place. This means, for example, persuading employers not just of the importance of imple- menting occupational health-related legislation but also of the benefits of generally paying attention to the health and well-being of their em- ployees. As well as being morally right, looking after one’s employees is increasingly recognised as making good business sense – people are a vital asset to a successful business. Occupational health nurses have to earn the trust and respect of employers, employees and colleagues.
This means being a good team member but also having the confidence, backed by knowledge, to negotiate with and influence others to have a positive impact on workplace health.
The third edition starts with an introductory chapter on the wide- ranging and developing role of the occupational health nurse. This chapter, ‘Introduction: The Role of the Occupational Health Nurse’, also touches on some key general professional issues, such as competence and confidentiality, topics which are referred to repeatedly throughout the book. The main part of the book then follows, arranged by grouping the chapters together by related topic for easier reference. There are four sections: ‘Management’, ‘International Issues’, ‘Practice’ and ‘Education and Research’. In addition to the two completely new chapters already mentioned, Dr Panayota Sourtzi has updated and expanded Charles McK Graham’s ‘European Perspectives’ chapter to create a new chapter entitled ‘International Issues’.
This new third edition presents up-to-date information and aims to assist occupational health nurses, at all stages of their career, to deliver ef- fective services. I hope it might encourage nurses thinking of branching into occupational health to find out more. It might also be of interest to others, such as NEBOSH students, who undertake occupational health modules as part of their course.
I would like to thank all the contributors to the book and those who have given their time to comment on chapter drafts. I would also like to thank the editors, in particular Tim West, and all involved at Wiley- Blackwell.
xiv
Introduction: The Role of the Occupational Health Nurse
Daphne Bagley; Updated by Katie Oakley
Introduction
Occupational health nurses are the largest group of health care professionals involved in workplace health management in Europe (Whitaker & Baranski 2001). The Royal College of Nursing (verbal com- munication July 2007) estimates that 7000–7500 nurses work in occu- pational health settings in the UK. This number is unchanged from their 1996 estimate, quoted in the first edition of this book. Whitaker and Baranski describe occupational health nursing as a ‘frontline’ role involving a range of aspects, namely: clinician, specialist, manager, co- ordinator, adviser, health educator, counsellor and researcher. How can occupational health nurses contribute to improvements in public health by making a difference to the health, safety and well-being of the work- ing community? What is their role as qualified nurses in the workplace setting? Initially, the role is discussed in general terms, taking the recog- nised functions of the occupational health nurse as a starting point. The historical context of occupational health nursing is then summarised, before moving on to some important professional issues such as compe- tence, accountability, communication and role development in a chang- ing workplace. The chapter concludes with five case studies illustrating the wide-ranging and varied nature of the role but showing that, what- ever the setting, the overall aim of the job is the same – to help achieve improvements in the health of working people.
Occupational Health Nursing Edited by K. Oakley.
C2008 John Wiley & Sons, Ltd
1
Occupational health nursing is a specialist branch of public health nursing with its roots in traditional nursing care. Occupational health nurses are all registered nurses – in other words, they have been through years of rigorous training to qualify as nurses and obtain their official registration. They have subsequently maintained their registration by recording further education and experience and paying registration fees to the Nursing and Midwifery Council (NMC). Practice is regulated by the Nursing and Midwifery Council (the regulatory body whose primary function is to protect the public www.nmc-uk.org). Issues of accountability, confidentiality, professional standards and guidelines affect all nurses, and nurses are always conscious of the fact that they work within a legal framework.
So an occupational health nurse is a qualified, registered, account- able professional with years of experience of confidentially supporting, treating and helping people (often at very difficult times in their lives) in both hospital and community settings. They should thus have ex- cellent communication and problem-solving skills, and most have sig- nificant management experience, e.g. running a hospital ward. A nurse qualified in occupational health has an additional qualification which may be placed on the NMC specialist community public health nurse (SCPHN) register. The Nursing and Midwifery Council has 3698 nurses with a recordable occupational health qualification (as at 31 March 2006).
Does being a registered professional command trust and respect?
Not automatically, however we would argue that employers and em- ployees are likely to value an occupational health nurse’s opinion on health matters and we must work hard to build on and retain this trust by acting with integrity to make a difference to health in the workplace.
How can occupational health nurses improve the health of the work- ing population? How do they work with employers and employees and with other professional groups to reduce sickness absence and assist with rehabilitation and making workplaces healthier and safer?
What is it that the nurse has to bring to the workplace? This book at- tempts to answer these questions by exploring topical issues, illustrated with examples from a variety of settings and placed against a back- ground of general developments in health care, and public health in particular. Every chapter is written by experienced occupational health nurse(s), many with additional qualifications and expertise, practicing in occupational health service provision, management, research, con- sultancy or education. This introductory chapter on the role of the occupational health nurse sets the scene by outlining the job func- tions, historical context and some of the governing principles and key issues of importance to occupational health nursing professionals today.
What Do Occupational Health Nurses Do?
The basic tenets of occupational health nursing practice are to promote health at work and to protect the health of the worker. Aw et al. (2007) define occupational health as:
a multifaceted and multidisciplinary activity concerned with the prevention of ill health in employed populations. This involves a consideration of the two-way relationship between work and health. It is as much related to the effects of the working environ- ment on the health of workers as to the influence of the workers’
state of health on their ability to perform the tasks for which they were employed. Its main aim is to prevent, rather than cure, ill health from wherever it arises in the workplace
In general terms occupational health is about the relationship between work and health and health and work, and paying attention to this is part of good risk management for any successful business. The general func- tions of an occupational health service (OHS) identified by the World Health Organisation (WHO 2002 pp. 11–12) provide a classic framework (Figure 0.1).
Dorward (1993) listed the functions of occupational health nursing as:
r health surveillance of the work environment r accident prevention
r prevention of occupational ill health r treatment of illness and injury at work r first aid organisation
r promotion of health and prevention of ill health r counselling
r rehabilitation
r keeping records and producing reports
r liaison and co operation (internally and externally) r administration of the occupational health unit r research.
All of the above functions are discussed in this book; some, such as rehabilitation, health surveillance, health promotion and research, have specifically dedicated chapters.
Most occupational health nurses perform a wide-ranging and varied role, which may include activities such as health screening and health surveillance, establishing and managing occupational health services, case management, and running a travel clinic and health promotion programmes. Some are involved with teaching and clinical supervision and mentoring. Many participate in or conduct research, surveys and
While the responsibility for workers’ safety and health rests with the employer, the OHS will be required to give expert advice to employers, individual workers and their repre- sentatives, and to carry out essentially preventive functions. These functions should aim at:rrrr Establishing and maintaining a healthy and safe work environment;Maintaining a well-performing and motivated workforce;The prevention of work-related disease and accidents; andThe maintenance and promotion of the work ability of workers.
They hence may comprise the following:
r Identification and assessment of the health risk in the workplace;
r Surveillance of the work environment factors and work practices that affect workers’
health, including sanitary installations, canteens and housing, when such facilities are provided by the employer;
r Participation in the development of programmes for the improvement of working practices, as well as testing and evaluation of health aspects of new equipment;
r Advice on planning and organization of work, design of workplaces, choice and maintenance of machinery, equipment and substances used at work;
r Advice on occupational health, safety and hygiene, and on ergonomics and individual and collective protective equipment;
r Surveillance of workers’ health in relation to work;
r Promoting the adaptation of work to the worker;
r Collaboration in providing information, training and education in the fields of occu- pational health, hygiene and ergonomics;
r Contribution to measures of vocational rehabilitation;
r Organization of first aid and emergency treatment; and
r Participation in the analyses of occupational accidents and occupational diseases.
Figure 0.1 Prevention, Health Protection and Safety: Occupational Health Service Functions
Source: WHO 2002 pp. 11–12
investigations within the company, for example identifying trends in sickness and accident statistics, auditing health programmes and con- ducting environmental surveys and writing reports. They sit on health and safety committees and contribute to and write policies and proce- dures. Occupational health nurses are increasingly involved in assisting managers with sickness absence issues (see Figure 0.2).
The job is varied – a nurse might hold a clinic in the morning and be out assessing and advising in the afternoon. They will be with people at their workstations listening, looking and talking to find out exactly how they are working, and whether this is affecting or has the potential to affect their health.
Occupational health nurses are recognised at the highest levels and are involved in national target setting (e.g. the significant nursing representation on the Support Programme Action Group of Securing Health Together www.ohstrategy.net and www.hse.gov.uk/sh2/pags/
supportreport.pdf).
r Make welfare visits.
r Discuss medical problem in confidence with employee. Regular contact and support.
r Liaise with GP/hospital consultant/welfare officer/occupational health physician as necessary.
r In some cases, help to facilitate treatment if the company provides private medical insurance or is willing to ‘fast track’ staff by paying for investigations or treatment options.
r Advise management on:
r employee progress
r expected duration of absence
r rehabilitation
r retirement.
r Offer advice and guidance on all health-related matters.
Figure 0.2 The Role of the Occupational Health Nurse in Sickness Absence Man- agement
Where Do Occupational Health Nurses Work?
Some occupational health nurses work as members of an occupational health team (more common in large companies, local authorities and the NHS). Many occupational health nurses work as sole practitioners.
Other practitioners provide nurse-led occupational health services to different clients in both the private and public sectors. A small number work in education and research and alongside specialist doctors for the Health and Safety Executive’s (HSE) Employment Medical Advisory Service (EMAS). The occupational health nurse is expected to demon- strate a wide range of competencies, abilities and skills in a variety of work settings.
The History of Occupational Health Nursing
Public health nursing now has a broad remit including health service provision, commissioning, health protection, management, education and research. Public health objectives and themes now go beyond the historical associations with clean water, food, hygiene and shelter, al- though these still remain key determinants of health. Occupational health nursing has always been associated with public health nursing, as the following historical overview illustrates.
Following the industrial revolution of the 18th and 19th centuries, the migration of people from rural areas to cities and towns led to increased health problems associated with poor living and working conditions.
Mortality rates were high among sufferers of tuberculosis, typhoid and cholera. High infant mortality and poor living conditions were noted by
such men as Edwin Chadwick. Chadwick’s report on The Sanitary Condi- tion of the Labouring Population of Great Britain influenced the introduction of the Public Health Act of 1848, which included the establishment of Local Health Boards and the appointment of health officials. The Royal Sanitary Commission (Chadwick 1842) emphasised the importance of preventive medicine, but this was never really followed through effec- tively, in spite of the creation of a National Health Service (NHS) after the Second World War.
History records that the work of early industrial health nurses was based on public health principles. Charley (1978) provides an excellent account of these times, and describes the duties of Philippa Flowerday, believed to be the first industrial nurse in the UK, who was employed by the Norwich mustard factory of J. and J. Colman in 1878 at 26 shillings a week. In America, Wright (1919) and others (McGrath 1946), cited in Rogers (1994), described industrial nursing activities in the 19th century and beyond, emphasising the community focus, public health agency- sponsored services and the school nurse role. The history and devel- opment of occupational health since then has been fully described in other texts, so a summary of the milestones is set down for reference in Figure 0.3.
Acheson (1988) defined public health as: ‘the science and art of pre- venting disease, prolonging life and promoting health through organ- ised efforts of society’ and placed public health high on the health service agenda. The Gregson Report (1984) acknowledged that occupational health practice should be a component of primary health care. Interna- tionally and locally, new models of practice have been developed that place occupational health within public health frameworks and pro- grammes of care.
The Black Report highlighted inequalities in health (Townsend and Davidson 1982), and Calman (1995) stated that four key issues requir- ing special attention were: equity and equality, food poisoning, drug and solvent misuse, and health in the workplace. National health tar- gets on equality aimed to bring up ‘the health experience of those in the least healthy groups closer to that of the currently most healthy groups’
(DoH 1995a). The health gap continues, and occupational health nurses have an important part to play in improving the health of the working population by promoting equal access to health information. Waddell and Burton (2006) found that work is ‘good for you’ but only if it is
‘good’ work. Ballard (2006c) says this evidence review ‘is important because assumptions about the health benefits of work have been ex- trapolated from evidence that joblessness is bad for health rather than direct evidence on the positive impact of work itself.’ Ballard warns that
‘people on benefits, coping with mental illness or facing discrimination on grounds of race and or disability are most likely to be at the wrong end of the “social gradient in health” and . . . where they can find work
370 BC Hippocrates Observed appalling working conditions.
Linked colic symptoms with lead poisoning.
Agricola (1494–1555) Miners and their diseases.
& Paracelsus (1493–1541)
Ramazzini (1633–1714) ‘Father of Occupational Medicine’.
1775 Percival Pott Observed scrotal cancer in patients who had been chimney sweeps.
INDUSTRIAL REVOLUTION
1800s Urbanisation; child labour and the employment of women.
1802 Health and Morals of Apprentices Act.
1831 Charles Turner Thackray The Effects of the Principal Arts, Trades and Professions on Health.
1833 First Factory Act (updated 1844).
1842 Edwin Chadwick The Sanitary Condition of the Labouring Population of Great Britain.
1844 First certifying factory surgeon.
1848 First Public Health Act.
1855/72 Appointment of the first workplace medical officers.
1878 Philippa Flowerday First industrial nurse (J. and J. Colman’s mustard factory).
1895 Legal requirement to notify certain substances harmful to health, e.g. lead, arsenic, anthrax.
1897/1906 Workman’s Compensation Acts.
Sir Thomas Legge (1863–1932) First Medical Inspector of Factories Industrial Maladies (1934).
1901 Doctors inspect places of work.
1916 College of Nursing founded (Royal Charter 1928).
1932 Survey of Industrial Nursing, Royal College of Nursing (RCN).
1934 Training for nurses established by the RCN.
1937–61 Factories Acts.
1946–48 National Health and Insurance legislation.
1948 Appointed Factory Doctors.
1949 Report of a Committee of Enquiry (Gowers) into
Health, Welfare and Safety in Non-Industrial Employment.
1950 Report of a Committee of Enquiry (Dale) on
Industrial Health Services.
1972 Report on Health and Safety at Work (Robens’
Committee).
1974 Health and Safety at Work (etc.) Act.
1988/92 UK/European legislation affecting health and safety practice.
2006 Appointment of first UK National Director for Work and Health.
Figure 0.3 Selected Milestones in the History of Occupational Health
it may often be in low skilled poorly paid unsafe and insecure work environments.’
It seems logical then that occupational health nursing comes within the realm of public health nursing, as ‘the care of people with actual or potential health problems and manipulation of the environment to contribute to optimal health have been seen as the generic base of nurs- ing practice for as long as nursing practice has been described’ (Fagin 1981). The definition for specialist community public health nursing used by the Specialist Community Public Health Nursing Committee is that it:
aims to reduce health inequalities by working with individuals, fami- lies, and communities promoting health, preventing ill health and in the protection of health. The emphasis is on partnership working that cuts across disciplinary, professional and organisational boundaries that impact on organised social and political policy to influence the determi- nants of health and promote the health of whole populations (www.nmc- uk.org/aSection.aspx?SectionID=29, accessed 22 June 2007).
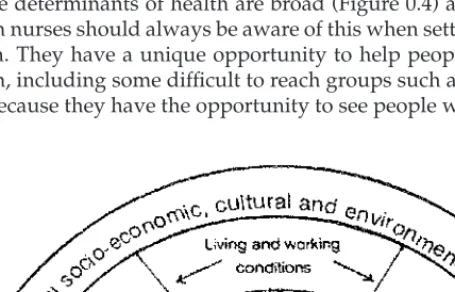
The determinants of health are broad (Figure 0.4) and occupational health nurses should always be aware of this when setting priorities for action. They have a unique opportunity to help people improve their health, including some difficult to reach groups such as migrant work- ers, because they have the opportunity to see people where they work.
Figure 0.4 The Main Determinants of Health From Dahlgren and Whitehead (DoH 1995a). Crown copyright is reproduced with the permission of the Controller of The Stationery Office
Occupational health nurses, as the largest group of qualified health care professionals in the workplace, must ensure that they are fully involved with and contributing to the ground-breaking cross-depart- mental government Health, Work and Well-Being Programme (HM Government 2005). This programme, led by Professor Dame Carol Black (the National Director for Work and Health), has the same aim as we do, namely ‘to improve the health and well-being of people of working age’.
Maintaining Professional Standards
Occupational health nurses must always keep in mind their professional duties and responsibilities. This is particularly important for the occu- pational health nurse who is working outside the traditional hospital nursing management structure. The occupational health nurse may be isolated and working as an independent practitioner and must be re- sponsible for continued awareness of the need to maintain required professional and ethical standards. This should not interfere with the responsibility to the employer or client but diplomacy, negotiating and influencing skills are often required to ensure that, for example, a health surveillance programme is given priority over other, ‘less essential’
programmes.
Upholding the core values of nursing is important:
You are first and foremost a professional nurse with a duty to the public and your profession, and you must safeguard those interests and respon- sibilities (RCN 2003).
Every nurse has an individual responsibility to reflect on their prac- tice, to keep up to date, to ensure they are always working within pro- fessional boundaries, according to governing principles and the NMC Code of Professional Conduct (NMC 2004), and to consult and re- fer to others as appropriate. The NMC Code of Conduct: Standards for Conduct, Performance and Ethics may be used as a framework for ethical decision-making, together with other Council advisory pa- pers, which may not be enforceable in a court of law but whose sub- stance may contribute to minimum standard-setting for the registered nurse.
Networking with colleagues and other experts and sharing best prac- tice is a must. There are many occupational health groups around the country, which meet every few weeks after work and feature in- vited speakers, often focusing on topical issues such as forthcoming health-related legislation. There are active special interest groups such as the Society of Occupational Health Nursing (RCN) and the Associ- ation of Occupational Health Nurse Practitioners, both of which hold
annual conferences. There are also many other relevant conferences and special training workshops. Finally, it is important to keeping up to date by reading professional journals such as Occupational Health (at Work), Occupational Health and Occupational Health Review and checking relevant authoritative web sites for ‘hot topics’ and information (e.g.
government departments, the Health and Safety Executive, the Health Protection Agency).
The Craft of Occupational Health Nursing
A report for the RCN Society of Occupational Health Nursing (SOHN) (Ballard et al. 2005), involving a survey of a sample of SOHN members, found that ‘communication and listening’ was the most highly rated competency for the job. Ballard (2006b) listed the five top functions of occupational health nursing as: confidential handling of health and per- sonal data, assessment of fitness to work, health surveillance, disability management and assessing risks to mental health.
Occupational health nurses should be a highly-trained and experi- enced asset to an organisation, doing preventive work, understanding people’s needs and advising on risks, hazards and environmental prob- lems. They need to be enthusiastic and must be able to communicate their services effectively throughout the organisation, so that the ben- efit can be demonstrated to all. An experienced, confident and knowl- edgeable occupational health nurse who is a good communicator has much to offer to employers and employees in terms of providing cost- effective, high-quality, practical help in the common aim of achieving a safer, healthier workplace.
We see nursing as a craft developed over years of training and expe- rience. Fischhoff (1995) described the process of communicating risks to patients as ‘craftwork’ requiring careful planning and implemen- tation. This could be applied to the development of skills in occupa- tional health nursing as we learn lessons from our experiences with people at work (both clients and colleagues), gradually building up a wealth of knowledge to improve our practice and that of others.
Fischhoff states: ‘complex skills are acquired slowly e.g. aspiring mu- sicians need to attend many concerts and practice before they can benefit from participating in master classes.’ Sharing good practice is important. This can be achieved by getting involved in professional as- sociation and local occupational health group activities and national strategies such as the aforementioned Health, Work and Well-Being Programme (HM Government 2005), and by researching and writing for publication.
Nurses are practical people, trained to listen, observe and assess, to care for people when they are sick and to assist them with rehabilitation, to take responsibility when appropriate and work with patients to help
them improve their health. In occupational health, they also need to be diplomatic and adaptable in a business setting to convince employers and employees of the benefits of good occupational health for them and their organisation. This means negotiating and influencing at all levels of an organisation, including the management board and union representatives.
A week’s work may involve travelling to various sites, for example presenting to the board of a large company, facilitating a workshop for a community, running a clinic and advising on a health problem in a food processing plant. As with much public health work, the benefits are often long-term and difficult to measure and demonstrate. Getting results means assessing the key issues, listening to clients and learning from people using the service, working out what they want and assessing how that fits with the nurse’s own perception of the priorities in health protection and legislative terms, and negotiating an action plan.
Competence
Occupational health nurses have nursing knowledge underpinned by physiological knowledge, and this is a useful support for the technical and scientific specialities of the hygienist and the health and safety ad- viser. Different approaches may be used in implementing the law, and the occupational health nurse can make an important contribution as a team member. Like all professionals, they need to have the confidence to be aware of their limitations and be conscious of their competencies, strengths and limitations and how to put these to the most effective use.
The RCN publishes a benchmarking guidance document on occupa- tional health nursing competencies (Bannister and Maw 2005). In this key document, Bannister and Maw, following extensive research and consultation, detail the competencies that should be expected at differ- ent levels of practice, moving from ‘competent’ through ‘experienced’
to ‘expert’.
What is a competent occupational health nurse? Competence is a key issue whatever the task at hand, whether giving advice on health- related legislation, counselling employees who are experiencing stress or undertaking tasks associated with health surveillance and health screening.
The term ‘competent person’ is used in the Factories Act 1961 and other legislation, but has been inadequately defined. There is no statu- tory definition of ‘competent’; the United Kingdom Central Council for Nursing, Midwifery and Health Visiting (UKCC) report ‘Fitness for Practise’ (1999) describes competence as ‘the skills and ability to practice safely and effectively without the need for direct supervision. The con- cept of competence is fundamental to the autonomy and accountability of the individual practitioner . . .’ (UKCC 1999).
‘Competence’ is included in the characteristics of a professional listed by Rogers (1994). The professional ‘possesses expertise, formal educa- tion or special technical competence; has a unique degree of autonomy that entitles her or him to exercise judgment; consciously conforms to a code or standard; feels a sense of service to humanity; acknowledges a higher responsibility for more than making a living; instils public trust.’
A competent occupational health nurse must keep up to date, not just with legislation, but with the changing workplace and emerging threats, such as pandemic influenza and bio-terrorism, and is involved in associated contingency planning and policy development. They are also involved in policy and practice development from the health perspective related to demographic changes and issues of equity, such as increasing retirement age, increase in temporary, agency and migrant workers, and teleworking.
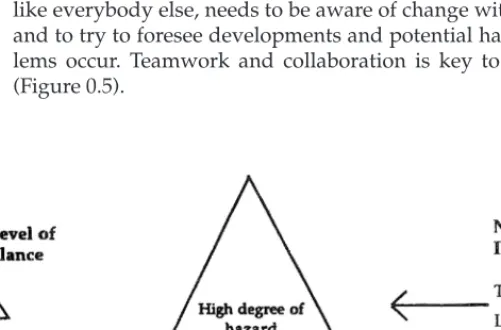
With changes in the type and pattern of employment, the hazards and risks of working have changed. There are still hazards from chemicals and substances, but there has been a great reduction in manufacturing and heavy industrial work. Risk management is an important part of protecting businesses and employees. The occupational health nurse, like everybody else, needs to be aware of change within the workplace and to try to foresee developments and potential hazards before prob- lems occur. Teamwork and collaboration is key to workplace health (Figure 0.5).
Figure 0.5 The Occupational Health Nurse within a Multi-Disciplinary Framework
General health promotion on issues such as healthy eating, alcohol and smoking on an individual or group basis has traditionally been a part of the occupational health nurse’s work, and obviously such issues can potentially affect work performance (see Chapter 10). There is little point, however, in addressing these issues alone without first tackling the hazards of the workplace.
Persuading the Employer
Occupational health nurses can help employers and employees to un- derstand their duties and responsibilities in relation to workplace reg- ulations, codes of practice and publications which place occupational health practice high on the health and safety agenda. Employers usually want answers to the following questions: ‘Have I got to do it?’ and ‘How much is it going to cost?’
The occupational health nurse, in conjunction with others in the health and safety team, can help employers by explaining why mea- sures are required in their organisation and the benefits of complying with the law. It is useful to point out estimated costings, including the potential effect of non-compliance on the company image. Quoting case studies related to the particular setting can help, e.g. to illustrate the importance of safe working systems in an X-ray department, the case of a radiographer who developed occupational asthma could be quoted. A radiographer was awarded more than £ 75,000 damages against the em- ployer, who was found negligent (Ogden v Airedale Health Authority 1996). In his summing up, the judge said, ‘it is in my judgment incum- bent upon an employer who requires employees to use chemicals in the course of their work to make inquiry as to the safety hazards which they present’ (see Chapter 9 for more details on health and safety matters).
More Legal and Ethical Issues, Including Confidentiality
Chris Cox (2006) of the RCN legal department, in a presentation on indemnity insurance, legal accountability and the occupational health practitioner, listed core competencies for all health practitioners:
r A thorough grasp of fundamental legal principles around account- ability and standards of care, the assessment of capacity and law of consent, confidentiality.
r A clear understanding of equal opportunities, disability, human rights and (if appropriate) mental health legislation, other relevant employment law.
r Knowledge of relevant professional codes of practice.
Nurses may encounter conflicts arising from, for example, maintain- ing confidential records and reports. Since the second edition of this book an occupational health nurse has been awarded compensation for unfair dismissal in a case which involved refusing to divulge confiden- tial information about an employee without consent (Tracey Cooke v West Yorkshire Probation Board).
In relation to records and reports, decisions have to be made regard- ing who must know, who should know, who could know and who should not know (Downie & Calman 1994). The patient’s interest is paramount, and the burden of proof lies with the person providing the information. Occupational health nurses have a duty to ensure that re- ports and records are held in trust, and that the information retained is both clear and concise, as access to the information may be required by a court of law. Disclosure of information may also take place if the patient provides consent (preferably written), and if the information is required ‘in the public interest’. The occupational health nurse then has accountability under civil law and criminal law to all parties involved.
(See Chapter 2, Appendix 2.1 for a sample policy on confidentiality.) If in doubt, seek advice from colleagues, other experts or your professional association. A key reference book on legal matters is the authoritative and user friendly Occupational Health Law by Diana Kloss (4th edn 2005).
Professional negligence and duty of care, standard of care, the implica- tions for practice of the Disability Discrimination Act 1995, the Human Rights Act 1998, health and safety legislation and much more are cov- ered in this book.
Conflicts may also be experienced in relation to patient advocacy.
This is about upholding an individual person’s rights; acting in the best interests of the person; and acting as an intermediary on behalf of a person who is unable to articulate clearly his or her health needs to service providers. Empowering the individual to engage in personal target-setting is important here. The health professional is no longer perceived to be the sole expert, the ‘teacher’ or even the ‘victim blamer’.
Power should be transferred to the client, creating a ‘partnership in care’, with critical appraisal of the relationship in terms of self-motivation and achievement. This is just as important in occupational health as it is in other aspects of health care, and involves special skills, diplomacy, experience and time to listen.
Case Studies
The following case studies aim to give a flavour of the role of the occu- pational health nurse in a range of employment settings. The majority of occupational health nurses work in the independent sector (RCN verbal communication July 2007). The first case study relates to an independent OH service provider. This is followed by case studies on an NHS OH
and safety service, a group OH service, an occupational health project and finally a self-employed OH nurse. Some general background on the type of service/organisation is given along with examples of work carried out in the specific case chosen.
Case Study 1: Independent Occupational Health Service Provider
The head of nursing services at AXA PPP healthcare OHS Ltd says that ‘For nurses working within the private sector there are unlimited opportunities to develop and increase their portfolio of skills and com- petencies. The benefit of being able to experience such a wide variety of industry sectors, and have exposure to different client, employee, leg- islative and health and safety requirements is a great advantage to their professional development and progression.’
AXA PPP healthcare OHS Ltd is the second-largest medical insurer in the UK and is part of the UK business of AXA Group, one of the top four insurers in the world. AXA bought MIS, an occupational health service provider, in the late 1990s, and following this acquisition is now trading as AXA PPP healthcare OHS Ltd. Its staff includes over 85 occupational health workers, including nurses, physicians, health and safety staff and occupational health technicians. They all work closely with specialised teams of administrative and operational support workers.
A senior management team made up of the leads from finance, oper- ations, medical, nursing and business development operationally and clinically manages the company. The SMT meets monthly to develop and implement business strategy.
The nursing team is managed by the head of nursing services, sup- ported by the regional clinical managers in the north and south. Regional clinical team leaders, again in the north and south of the UK, support and assist them.
The clinical leadership team has ownership of clinical governance, with responsibility for review, development, implementation and main- tenance of clinical standards and policies and procedures. The heads of nursing services and medical services – with appropriate input and sup- port from in-house and external clinicians with the specialist skills and knowledge for the specific projects ongoing at any one time – lead the clinical leadership team.
The nurses can be home-based, work from client sites or AXA of- fices, or have a mix of locations. There is no particular service delivery model that AXA implements as its aim is to provide clients with a flex- ible approach to occupational health service provision, ensuring their needs are continually met. The skill sets and abilities of the nursing team include, but are not limited to, health surveillance, travel health, vocational rehabilitation, nurse case management, stress management,
workplace risk assessment and audit, health education and promotion, sickness absence management, fitness for work assessment and training both in-house personnel and external clients.
Case Study 2: An NHS Occupational Health Service
Many NHS trusts now provide occupational health programmes for commercial enterprises and businesses in their locality, targeting small and medium-sized companies. The occupational health department in this case study is a self-funding business unit within an NHS primary care trust based in south-east England. The head of occupational health services (a nurse) says, ‘working within an NHS setting, occupational health is driven by a business philosophy. This is further endorsed by the advice and standards set by the NHS Plus initiative which is an arm of the Department of Health.’ The government’s NHS Plus network aims to strengthen partnerships between the public and private sectors of the community (www.nhsplus.nhs.uk).
As part of the health service business culture, income is generated by providing a service to non-NHS employees employed by outside agencies, ranging from charities to funeral directors. It is of utmost im- portance, however, that the service to trust employees is a priority.
The philosophy of the department is captured in its mission state- ment: ‘We are a market leader in the provision of a professional quality and dynamic service tailored to the needs of the working environment.’
The aim of the department is ‘the promotion of positive health and fitness’.
The service employs qualified and experienced occupational health nurses and doctors, who each have areas of responsibility in relation to all contracts within and outside the NHS. Other staff includes clerical/
administrative grades, a health and fitness adviser, a ‘moving and han- dling trainer’ and a psychologist who acts as a staff counsellor. Core occupational health activities are offered as part of a customer-focused service, plus a wide range of health programmes, which include work- place health surveillance, assessments and employment health screen- ing. A gymnasium facility with supporting programmes is available for staff, as well as a comprehensive travel service. Members of staff are made aware of specific health topics on national awareness days.
Both qualitative and quantitative auditing is carried out by the occu- pational health service, based on statistical returns, activity analyses and evaluations, following training courses and health-related programmes (including stress-management sessions).
Innovations include developing specific projects, for example mental health services for staff; working with bullying and harassment advisers;
and back care and rehabilitation programmes, which include a fast- track referral system, clinical exercise programmes and a management case conference as part of return-to-work policies. Extensive work with
three call centres is another development. Another separate unit based in a satellite hospital has a travel clinic, fitness suite, equipment for disabled users, stress-relaxing chairs and a steam room. There is a strong emphasis on rehabilitation.
Case Study 3: A Group Occupational Health Service
The Gregson Report (1984) recognised the important contribution of group services, tracing their development and status and stating that
‘much depends on the zeal and proselytizing abilities of the staff’. The report recommended the extension of group services ‘especially in areas of primarily industrial development’.
Group health services employ a skill mix of professionals, who usu- ally operate from a central base but also provide on-site activities. Close liaison is maintained between the services and the regulatory bodies, including EMAS. Most services belong to an association of group oc- cupational health services and have a common identity in that they all provide services that are ‘employer-led’, non-profit-making (having charitable status) and accountable to member companies.
This case study is an example of a group service managed by an occupational health nurse and based on an industrial estate. Other oc- cupational health nurses are employed, together with two qualified occupational health physicians and two other medical officers who work on a sessional basis. The medical officers carry out executive med- ical examinations for member and non-member companies. Ancillary staff includes a first aid supplies officer and a physiotherapist. Admin- istrative support is provided by the company secretary/administrator, accounts clerk, two secretaries and two receptionists/clerks. First aid training is provided by a self-employed contract instructor.
Around 100 small and medium-sized enterprises (SMEs) belong to the service. Subscription charges are invoiced on a per capita basis, and additional charges are made for specific services (at a subsidised rate), such as health surveillance (health and safety legislation), health promotion activities, lifestyle screening, first aid and health and safety training, manual handling training and vision screening. In addition, some 80 companies use the service on an ad hoc basis.
Case Study 4: An Occupational Health Project
Occupational health projects (OHPs) have been in existence since 1978 and work with GPs and other health care staff to provide an independent occupational health advisory service to workers in a defined geograph- ical area. Jackson (2004) provides an interesting and detailed summary of the work of two projects in his report of an evaluation research study conducted for the HSE.
A national association has been established and project members meet regularly. The aims of the association include providing:
mutual aid and benefit to member organisations (staff and commit- tee members); pursuing a joint programme of exchange and activities;
attempting to develop new methods of identifying emerging patterns of occupational disease; providing a national voice; developing awareness of occupational health . . . in primary and secondary health care and fur- thering the development and integration of occupational health services into primary health care in England, Scotland and Wales; emphasising the special value and strength of collective action to resolve health and safety problems; developing skills and capacities of workers and patients to solve problems for themselves.
Other activities include creating models for the future develop- ment of occupational health services; establishing closer links with Europe; developing resources for public use; and identifying training programmes. Each OHP produces an annual report, and the projects are all at different stages of development. Funding for the projects comes from different sources, for example the Department of Health, health authorities and local authorities. Staff members are drawn from different backgrounds and include academics, scientists and nurses.
A nurse working in a long-established project says:
OHPs are ideally placed to plug a gap in occupational health service pro- vision, with a particular remit to provide health and safety advice and information to small and medium-sized enterprises, particularly where no on-site occupational health provision is available, and where health inequalities need to be addressed. They appear to provide impartial help, whereas with on-site services conflicts of interest may arise, for exam- ple among managers, staff representatives and the work of occupational health practitioners.
This particular project conducts research projects, e.g. on stress in taxi drivers and on health in self-employed ‘home-workers’. Several leaflets, available in different languages, are produced by the project – for example, on mothers at work.
As part of expansion of their services, OHPs see themselves continu- ing to provide workplace health and safety advice, establishing new working partnerships with providers of community health services, as well as continuing to strengthen existing relationships with health purchasers.
Case Study 5: A Self-Employed Occupational Health Nurse
Some self-employed occupational health nurses specialise in key areas such as stress management and the management of back pain. Others may work through nursing agencies, providing relief cover on a tem- porary basis. Some nurses have developed a consultancy role, which might include, for example, combining teaching with practice and pro- viding professional advice and support to organisations in other coun- tries. Numerous opportunities exist for the self-motivated, multi-skilled and experienced occupational health nurse to provide a wide range of services (see Chapter 5 for a detailed discussion).
An experienced and qualified occupational health nurse was prompted to become self-employed following redundancy. She has since used her knowledge, skills and abilities in a creative way and has de- veloped a portfolio of skills that has wide appeal and involves both on-site and off-site activities. Such activities include lifestyle screening, workplace risk assessment and environmental survey, vision screening and first aid examining. This occupational health nurse is also actively engaged in health education on behalf of a women’s cancer charity organisation and is developing male health education programmes.
Another important consideration for this nurse is the financial aspect of being self-employed. She has many expenses associated with, for ex- ample, ensuring adequate professional indemnity insurance, subscrib- ing to professional journals and organisations, purchasing equipment and supplies (including those required to maintain a home office base) and marketing. As one should when setting up any business, she sought advice on writing business proposals and engaged an accountant.
Changes in personal circumstances and a desire for freedom and more control over workloads may motivate nurses to become self-employed practitioners. The role of the occupational health nurse cited in this case study highlights the importance of practitioners keeping up to date clinically, in order to maintain competence and professional standards.
Conclusion
Occupational health nursing aims to improve people’s health at work.
Sometimes the effect of an occupational health intervention is obvious and measurable and this is satisfying for all concerned, for example fol- lowing the introduction of a successful case management programme, or reducing the rate of back injuries amongst care workers following manual handling training and ergonomic interventions. More often, however, the effect is not immediately obvious or demonstrable as, in common with much public health work, it often involves preventing
health problems in the medium and long term. An occupational health nurse therefore needs to be strongly committed to the discipline and be- lieve that their work can make a difference. It is important to effectively balance sometimes competing demands and interests; remembering re- sponsibilities and duties to the employer and the employee without compromising professional guidelines and code of conduct.
Occupational health nursing practice is a synthesis of the study of the core values of community health nursing within the context of public health, combined with an in-depth knowledge of occupational health and safety and an understanding of the organisational and psychosocial factors affecting the workplace. Working with colleagues as a team mem- ber and in partnership with patients/clients is integral to any branch of nursing. Nurses must be competent at assessing and problem solving, but also at knowing when to refer on and to whom, e.g. occupational health physicians, safety professionals, ergonomists and hygienists.
Occupational health nursing is a challenging, interesting and satisfy- ing job. This chapter has tried to outline the role in order to set the con- text for the more detailed chapters which follow. In every aspect of the role, knowledge, qualifications, experience and contacts are not enough on their own; confidence, competence, adaptability and excellent com- munication skills, using language and methods appropriate to each setting, are essential for a successful and effective occupational health nurse.
References and Further Reading
The Acheson Report (1988) Public Health in England: The Report of the Com- mittee of Enquiry into the Future Development of the Public Health Function, London: HMSO.
Agius R. and Seaton A. (2006) Practical Occupational Medicine, 2nd edn, Hodder Arnold.
The Allitt Inquiry (1994) Independent Inquiry Relating to Deaths and Injuries on the Children’s Ward at Grantham and Kesteven General Hospital During the Period February to April 1991, London: HMSO.
Association of Occupational Health Practitioners (UK) web site, www.aohnp .co.uk (accessed 16 July 2007).
Aw T.C., Gardiner K. and Harrington J.M. (2007) Pocket Consultant Occupational Health, 5th edn.
Ballard J. (2006a) Delivering OH Services Part 1: Performance Indicators and Benchmarking in OH Nursing, Occupational Health (at Work) 2(5).
Ballard J. (2006b) Delivering OH Services Part 2: Nursing Competence and Per- formance Indicators, Occupational Health (at Work) 2(6).
Ballard J. (2006c) Healthy Working (editorial), Occupational Health (at Work), October/November.
Ballard J., Silcox S., Suff P. (2005) Performance Indicators and Benchmarking in Occupational Health Nursing, London: The At Work Partnership.
Bannister C. and Maw J. (2005) Competencies: an Integrated Career and Com- petency Framework for Occupational Health Nursing, London: RCN.
Black D. (1980) Inequalities in Health Report, London: DHSS.
Calman K.C. and Department of Health (1995) On the State of the Public Health.
The Annual Report of the Chief Officer of the Department of Health for the Year 1994, London: HMSO.
Chadwick E. (1842) The Sanitary Condition of the Labouring Population of Great Britain (republished 1965, M.W. Flinn (ed)), Edinburgh: Edinburgh Univer- sity Press.
Charley I.H. (1978) The Birth of Industrial Nursing, London: Bailliere Tindall.
Commercial Occupational Health Providers Association web site, www.cohpa .co.uk.
Confederation of British Industry (CBI) (2001) Focus on Absence Survey, London: CBI Publications.
Data Protection Act 1998.
Cox C. (2006) Presentation for the RCN Society of Occupational Health Nurses Annual Conference (unpublished).
Department for Work and Pensions (2004) The Framework for Vocational Reha- bilitation www.dwp.gov.uk/publications/vrframework/.DoH (1993) Tar- geting Practice: the Contribution of Nurses, Midwives and Health Visitors, London: HMSO.
Department for Work and Pensions (2007) Information on Health and Em- ployment. Corporate Medical Group www.dwp.gov.uk/medical (accessed 15 July 2007).
DoH (1995a) Variations in Health: What Can the Departments of Health and NHS Do?, London: HMSO.
DoH (1995b) Making it Happen: Public Health – the Contribution, Role and De- velopment of Nurses, Midwives and Health Visitors. Report of the Standing Nursing and Midwifery Advisory Committee, London: HMSO.
DoH (2003) Taking a Public Health Approach in the Workplace: a Guide for Occupational Health Nurses, London: DoH.
Dorward A.L. (1993) Managers’ Perceptions of the Role and Continuing Edu- cation Needs of Occupational Health Nurses. Research Paper 34, Sudbury:
HSE.
Downie R. and Calman K. (1994) Healthy Respect, 2nd ed., Oxford: OUP.
English National Board for Nursing, Midwifery and Health Visiting (1996) Oc- cupational Health Nursing. Leaflet, February.
Faculty of Occupational Medicine (2006) Guidelines on Ethics for Occupational Physicians, 6th edn, London: FOM, Royal College of Physicians.
Faculty of Occupational Medicine, Society of Occupation