Kemp, Ursula Kirk and Marit Korkman Essentials of Neuropsychological Assessment, Second Edition by Nancy Heb and William Milberg. In the Essentials of Psychological Assessment series we have tried to provide the reader with books that will provide important practical information in the most efficient and accessible style. The topics focus on a simple understanding of the essentials of administration, scoring, interpretation and clinical application.
In this updated and expanded second edition of Essentials of Neuropsychological Assessment, the authors present an overview of the assumptions, logic, knowledge base, and skills that underlie the practice of neuropsychological assessment.
Series Preface
For the experienced clinician, the books in the series offer a concise, yet thorough way to master the use of the continuously evolving array of new and revised instruments, as well as a convenient method of staying current with the tried and true measures. Test profiles must be used to make a difference in the child's or adult's life, or why bother testing. The reader also receives a discussion of the professional development and training of clinical neuropsychologists, as well as extensive information on resources for testing materials, journals, and textbooks in the field.
This book will be a welcome addition to the reading list of any graduate-level course in neuropsychological assessment, as well as to the bookshelves of practitioners seeking practical information on the procedures and logic of one of the fastest-growing specialties in clinical psychology.
INTRODUCTION TO
NEUROPSYCHOLOGICAL ASSESSMENT
As a definitive sign of neuropsychology's establishment as a recognized clinical specialty, the Board of Clinical Neuropsychology (ABCN; Meier, 1998) was established in 1981, and in 1983 began offering diplomatic status in clinical neuropsychology after it came under the auspices of the American Board of Professional psychology (ABPP). This book presents some of the fundamental concepts of the specific discipline of clinical neuropsychological assessment. The Seashore Rhythm Test, a traditional component of the Halstead–Reitan Neuropsychological Test Battery (HRB), was part of a test of musical ability (Saetveit, Lewis, & Seashore, 1940).
All tests used by neuropsychologists have in common (or should have in common) known reliability and validity as predictors of the presence of brain dysfunction.
DON’T FORGET
Part of this determination is trying to determine which part of the brain is involved. Test performance is not necessarily an indication that a function is localized to a specific part of the brain. Literature documenting the sensitivity of the tests' tasks to the presence of brain lesions emerged primarily after their creation.
The publication of the LNNB (Golden, Hammeke, & Purisch, 1978) represented a controversial frontier in the development of neuropsychological test methods.
THE DISCIPLINE OF
Unique to neuropsychology, these courses expand on basic education and training in clinical psychology and provide a knowledge base for the specialty of clinical neuropsychology. Rapid Reference 2.1 provides a summary of the Houston Conference Guidelines for Specialty Teaching and Training in the Field of Clinical Neuropsychology. The American Academy of Clinical Neuropsychology (AACN) developed and published its first set of practice guidelines for clinical neuropsychologists (Board of Directors, AACN, 2007).
Board certification in clinical neuropsychology from the ABN demonstrates an advanced level of competency as a clinical neuropsychologist.
ESSENTIALS OF THE INTERVIEW AND CLINICAL HISTORY
The process of clinical neuropsychological judgment involves integrating details of the patient's past and present life circumstances with empirical test data. It is important to obtain a detailed account of the patient's current symptoms and complaints, their pervasiveness and severity, and their effect on daily life. The clinician is interested in the subjective characteristics of the disease and the length of time the patient has been affected by the disease.
Here too, this results from interviews with the patient (if possible) and from review of medical records (also if possible). The interview can provide information about the organization, focus, and details of the patient's thinking, as well as the subjective aspects of his or her presenting problem. Likewise, personal items in the office should be placed out of sight of the patient during the testing session.
They also allow the examiner to see the patient's limitations in a non-test situation and allow the patient to demonstrate their symptoms. The interview enables observation of the patient's level of hygiene and standard of dress. Is the patient's behavior social and age appropriate, as evidenced by posture, eye contact, mannerisms, and so on.
The interview provides the examiner with an opportunity to observe the coherence of the patient's explanatory or narrative language, evidence of how well the patient's thoughts are organized. If the patient's thinking is disorganized, this reflects a possible thought disorder or perhaps impaired reality testing.
ESSENTIALS OF TEST SELECTION, ADMINISTRATION, AND SCORING
It is the examiner's duty to organize the test conditions so that the patient can take advantage of the opportunity to work to potential. To optimize patient performance, the examiner should try to gain the cooperation and trust of the person being tested. This maintains the formality of the professional situation and communicates your respect for the patient.
Scheduling a testing session depends on the referral question, the nature of the tests being used, and the focus and persistence of the patient. I read the book), use of adverbs (eg, the paper thing with the words vs. the book). In many cases, unusual deviations from implicit social norms and the examiner's own expectations are also deviations from the expectations of the patient's own culture.
For example, if a test is designed to be administered without a break, giving the patient a short break may reduce the accuracy of the confidence with which the test standards can be applied. Depending on the severity of the patient's language delay, assessment (as in hearing-impaired individuals) may need to be continued with nonverbal tests and other tests that do not depend on language ability (as previously described for testing patients with hearing problems). Perform nonverbal tests that require spatial manipulation and problem solving, but not vision (e.g., the Tactual Performance Test).
Patients achieving a score of 0.5 or above are classified as "with cerebral impairment". The Halstead Impairment Index is used to identify functioning consistent with brain damage, but it does not indicate the type or level of dysfunction. This test assesses the patient's ability to perceive tactile, auditory and visual stimuli on both sides of the body. This test is one of the working memory subtests of the WAIS-IV and WISC-IV.
Rapid Reference 4.19 provides a list of the test names, the appropriate age groups and the publishers.
ESSENTIALS OF INTERPRETATION
Criterion validity refers to the ability of a test to predict or correlate with other measures that define the test's function. In neuropsychology, tests are most often used as predictors of the presence of brain dysfunction. Content validity: The extent to which items on a test are actual exemplars of the construct being measured.
Undoubtedly, the most important technological development in measuring the condition of the tissues of the central nervous system is computed tomography. The Reitan Neuropsychological Battery, although extremely sensitive to the presence of brain dysfunction, is not a valid predictor of lesion location. It is easy to see that as the level of error increases, the level of reliability of the test decreases.
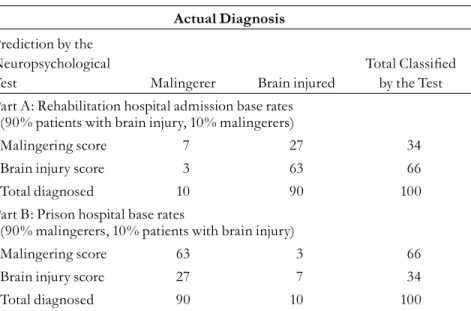
Due to the inconsistency of the measurements the ruler provides, its validity as a measure of. The accuracy of predictions about the presence or absence of a condition varies depending on the prevalence of the condition in the population tested. The accuracy of predictions about the presence or absence of a condition varies depending on the prevalence or base rate of the condition in the population tested.
Positive predictive value is influenced by the base rate of the condition in the population tested and is an important measure of the accuracy of a test in the situation in which it will actually be used. Negative predictive value is influenced by the base rate of the condition in the population tested.
SPECIAL ISSUES IN
Test developers can be sensitive to these issues, and numerous tests are designed specifically for use with developing children (e.g., the NEPSY-II). A given test result may reflect interactions between two or more of the following factors: changes in normal biological development, incomplete knowledge acquisition, and the focal effects of a lesion. When the physician is asked to assess the effects of a recent neurological illness and the ability to stand for extended periods of time, it may be necessary to evaluate the entire school record to map the overall course of the child's cognitive development to bring.
Although some tests originated in other languages such as French (e.g., Rey Auditory Verbal Learning Test; Rey, 1958) and Italian (Token Test; De Renzi & Vignolo, 1962), these instruments have been translated into English and are renormalized using a US population to achieve widespread use in the United States or Canada. This should not be surprising because tests are products of the cultural and language origins of their developers. These differences could potentially affect both the sensitivity and specicity of neuropsychological tests that have been normed only in the general population.
As might be expected, the neuropsychological assessment of the geriatric patient presents its own questions and challenges; these are summarized in the quick reference guide 6.3. If individuals with these disorders are included in larger numbers in the normal sample used for validation, the result of the criterion for classifying patients as having brain dysfunction may be too conservative and the sensitivity of the test will be compromised. A number of geriatric neuropsychological tests have been designed and validated to detect the presence of Alzheimer's disease, the most common degenerative dementia disease.
Furthermore, because the incidence of Alzheimer's disease itself increases with age, test norms that include data from randomly sampled age-matched normally functional individuals can be expected to include larger numbers of individuals with the early signs of dementia, leading to reduced sensitivity of these tests. as a function of the increased age of the individual. Such observations emphasize why the health status of the individuals comprising the normal samples should be known and specified in the validity studies of neuropsychological tests used with older adults.
