Screening the Newborn provides a practical, step-by-step guide for midwives and other practitioners taking on this role. The Newborn Screening provides midwives and other neonatal screening practitioners with a comprehensive guide to the holistic screening of the newborn baby. Routine newborn screening is accepted as good practice (Hall 1996) and its value in addressing parental concerns (Hall 1999) and ensuring parents know what to expect from their baby (Walker 1999).
The clinical examination of the newborn is also becoming a problem due to the increasing number of home births. Examination of the Newborn: A Practical Guide provides comprehensive guidance for the holistic examination of the newborn.
In the beginning
Scenarios will be used to explore specific issues, focusing on the role of the GP who conducts the first examination of the newborn. It is important to consider how this knowledge can affect the care you provide when you do the first examination of the newborn. Some of the issues facing new parents have been considered along with the possible responses from the practitioner.
The practitioner examines the newborn taking into account previous events, dilemmas and expectations. All of them will affect the future life and opportunities of the newborn.
Fetal development: influential factors
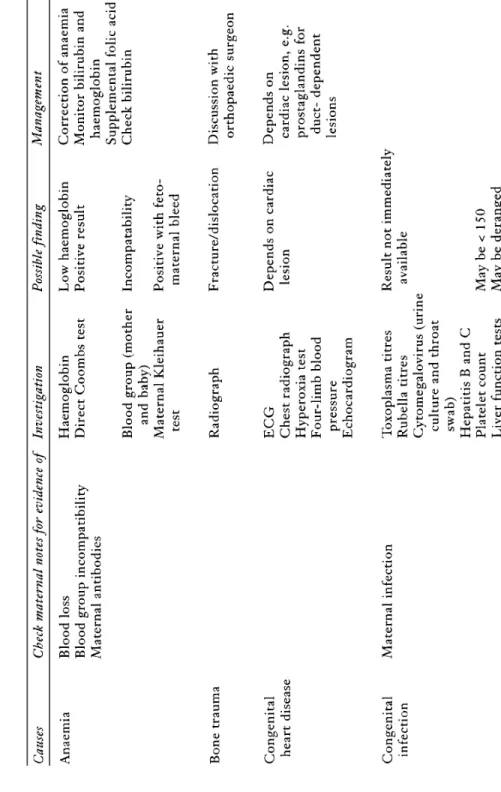
It is important that the clinician examining the baby is able to apply knowledge of the stages of fetal development to the individual antenatal history of the examined baby. Table 2.2 provides an overview of the main effects of smoking on the mother and foetus. For practical purposes, it should be estimated that about one-tenth of the mother's drug intake will pass to the baby through breast milk (Hull and Johnston 1993).
It is believed that about half of the population will be infected without realizing it. If maternal infection is confirmed during pregnancy, antibiotic treatment can reduce the risk of fetal infection.
Assessment of fetal wellbeing
This information is essential for the examination of the newborn and should therefore be read carefully by the doctor before seeing the baby. Clearly, prior knowledge of the prenatal history may enable the physician to improve the parents' experience of examining their baby. This can manifest itself in a barrage of questions for the professional conducting the initial examination of the newborn.
If the baby was in a certain position before birth, it may have consequences for the newborn examination. It has been shown that there are a number of antenatal parameters that the practitioner examining the newborn should be aware of in order to be sensitive to the needs of the mother and her baby.
Risks to the fetus during childbirth
Such knowledge also helps the doctor put into context some of the problems he might encounter in the newborn. The importance of the clinician's exploration in relation to the neonatal examination is twofold; Premature rupture of membranes (PROMs) are defined as rupture of the fetal membranes before the onset of labor and occurs in approximately 10% of all pregnancies; 90% of this is over time (Alexander and Cox 1996).
However, this does not mean that the doctor examining the newborn can be complacent about premature rupture of the membranes, especially if he works within a unit that actively manages such cases. The doctor examining the baby should consider all of the above when reading the woman's labor and delivery records to assess how this history may affect the newborn. The effects on the baby of the drugs commonly used in childbirth are described in the following paragraphs.
The practitioner examining the baby can encourage the mother in the above situation that the baby's response is likely due to the pethidine she received during delivery, and is therefore worth persevering with. The shape of the baby's head is a positive result of undergoing an unusual birth, which the practitioner may wish to comment on during the examination for the benefit of the parents. Therefore, the first newborn examination may be the first time the child is examined clinically, unless there is an indication.
The obstetrician who presided over the delivery should be informed of the tear and a careful record should be made. While going over the details of the mother's birth in detail, it is important to consider the condition of the baby at birth so that you can anticipate any questions the parents may have. Careful research into birth records provides many valuable details that will assist in the examination of the newborn.
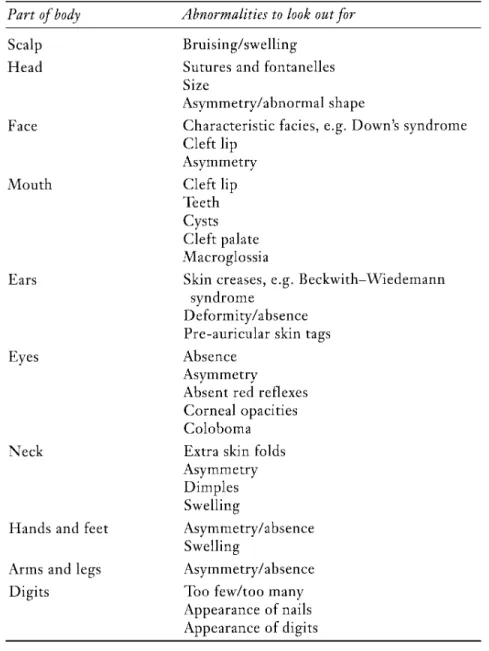
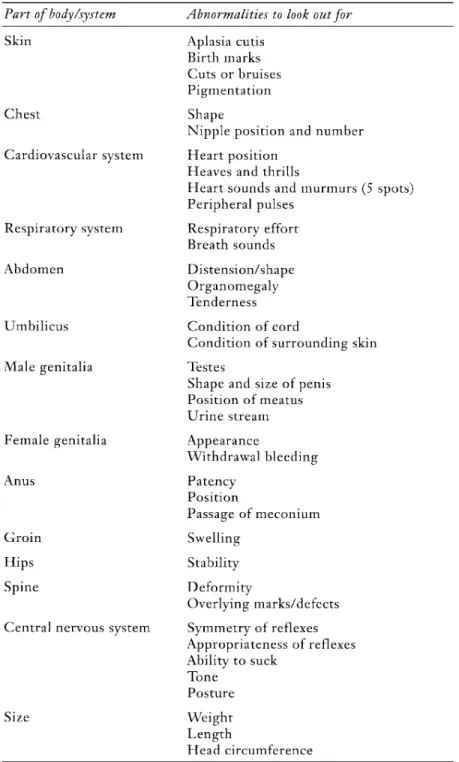
Neonatal examination
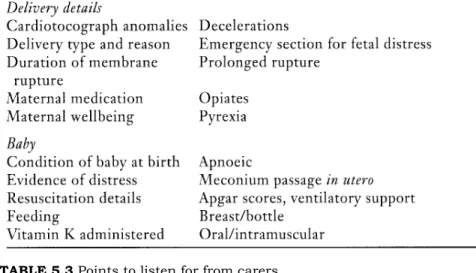
Before disturbing the newborn, much can be learned by listening to those who care for the mother and baby (Table 5.3). It is also important to collect the equipment that will be needed during the inspection and ensure that it is clean and in working order. If you have to leave the bed to look for equipment, a previously content baby may become fussy, hungry or in need of comfort, and the examination should be postponed.
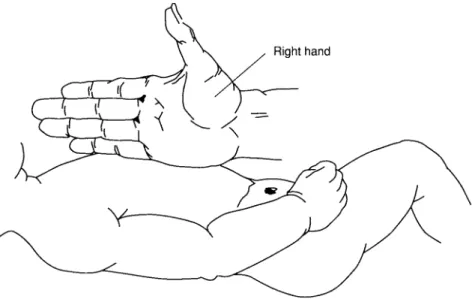
The first and third components are self-explanatory, but the second and fourth require an explanation of how they are performed, depending on which part of the child is being examined. Palpation is performed differently depending on the situation; therefore, specific instructions will be given at appropriate points in the chapter. It is performed by placing the middle of the left hand flat on the child's body and gently tapping the middle phalanx with the middle of the right hand.
This technique can be useful for examination of the chest (the percussion sound is hyperresonant in the presence of pneumothorax) and abdomen.
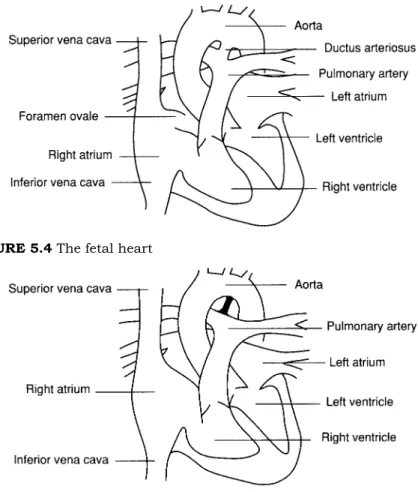
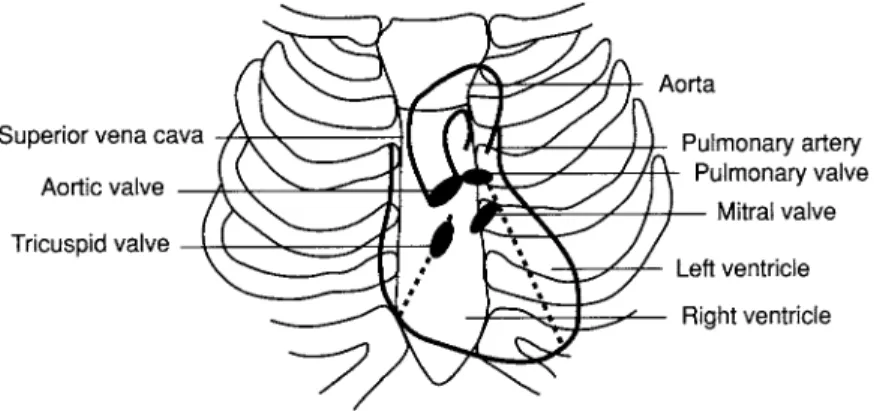
The doctor must be familiar with the normal anatomy of the eye before the examination (Figure 5.2). Look at their size, their position (including the distance between them), the features around them (epicanthic folds, eyelids and eyebrows) and the slope of the palpebral fissures (Figure 5.3). Low pulmonary blood flow is caused by a blockage of blood leaving the right side of the heart (right outflow tract obstruction).
The first heart sound (best heard at the apex) represents the closing of the mitral and tricuspid valves. Palpation of the abdomen is best performed by approaching from the right side of the baby. The procedure must be repeated centrally as the left lobe of the liver can be enlarged independently.
The skin on the underside of the penis may be attached to the scrotum (hordee). The baby's shin touches the side of the crib and the baby will perform a walking/climbing maneuver. The palmar grip reflex is elicited by placing the practicing little finger on the child's palm.
The plantar grasping reflex is elicited by touching the sole of the child's foot with the little toe. The baby is then carefully stretched and the movable rod is raised to touch the plane of the baby's foot. The baby should lie flat, with the head in contact with the top of the growth meter and the pelvis in a neutral position, i.e.
Abnormal findings and congenital abnormalities
This is usually associated with a shallow orbit, so for cosmetic reasons, and for examination of the normal eye, the baby should be referred to an ophthalmologist. The baby should then be discussed with an endocrinologist and a pediatric surgeon in light of the examination findings and results of the examinations. If ballooning of the foreskin occurs during urination, the baby's condition should be discussed with a surgeon.
These findings suggest congenital luxation of the hip, and the child should therefore be referred to an orthopedic surgeon. There may be a loud pulmonic second sound due to the pulmonary hypertension that develops as a result of the congestion. It may occur in the membranous part of the septum or in the muscular part.
The baby needs a referral to a cardiologist to confirm the diagnosis and ensure early repair of the defect. The child needs urgent referral to a pediatric surgeon for further investigations and repair of the lesion. Examine the child carefully, paying particular attention to the appearance and size of the genitals and other abnormalities.
Accountability and effective care
We have explored issues regarding who undertakes the first examination of the newborn, and it is now appropriate that accountability within this role is further clarified. The first examination of the newborn baby is not currently part of the role of all midwives or neonatal nurses. Symon (1998) outlines a case in which a child had congenital cataracts, which were not diagnosed during the first examination of the newborn.
What is the legal position of a practitioner who fails to detect a congenital condition in an infant during the first newborn examination. Paediatricians who carry out the newborn examination are usually qualified doctors who have been working for a pediatric consultant for about 6 months. Newborn screening is performed on all babies within the first 24 hours of life.
It is also essential that the designation of the practitioner is made clear to parents. Failure to communicate effectively is one of the most common complaints in health care (DOH 1994). Examination of the newborn is a screening test and should be offered as such in light of its ability to detect abnormality.
An audit is a "systematic and critical analysis of the quality of clinical care" (DOH 1993b) and, through the implementation of clinical governance in the UK National Health Service, it is an integral part of the provision of health care (DOH 1997). There are many aspects of the newborn review process that can be audited to ensure continuous improvement in the quality of care. We need to make sure that as healthcare professionals we contribute positively to their child's birth experience.
Useful addresses