It is sold with the understanding that the publisher is not engaged in rendering professional services. Concettina Tolomeo, DNP, APRN, FNP-BC, AE-C, Dawn Baker, MSN, CPNP, CCRC and Pnina Weiss, MD.
Preface
Moreover, as a child, when everyone wanted to be a teacher or an actress and play school or dress up, I wanted to be a nurse. I hope you enjoy the practical nature of this book and find it a useful reference as you prepare for teaching and throughout your nursing career.
Acknowledgments
Reviewers
Faustino, Assistant Professor of Pediatrics, Yale University School of Medicine, Department of Pediatric Intensive Care, New Haven, CT. University of Pennsylvania School of Family and Health Community Care Center for Health Equity Research Philadelphia, PA.
Nursing Care in Pediatric
Pediatric pulmonary anatomy and physiology
INTRODUCTION
ANATOMY OF THE RESPIRATORY SYSTEM Embryology
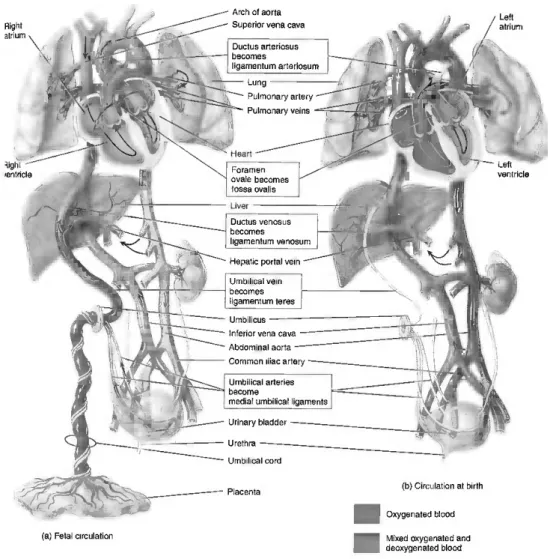
During the pseudoglandular period, there is a differentiation of the primitive airway epithelium (Post & Copland, 2002). Most of the blood passes through the foramen ovale on the left side of the heart.

Pulmonary vascular development and the tracheobronchial tree
The fetal circulation receives highly oxygenated blood from the placenta through the liver to the right side of the heart. The venous blood returning from the head flows through the right side of the heart to the pulmonary artery.
RESPIRATORY AND NONRESPIRATORY FUNCTIONS OF THE LUNG
While the lung bud is forming, the right and left pulmonary arteries are also growing; the branches of the pulmonary arteries follow the branches of the bronchi. By the end of the pseudoglandular period, the conducting airways are complete and have an adult pattern, as are all the conventional and supernumerary arteries leading to the terminal respiratory units.
Nongas exchange functions
The vascular pattern from the sites of gas exchange to the hilum, similar to that of the conducting airways, is complete by mid-gestation. In contrast, just as alveolar formation continues after birth, arteries within the terminal unit continue to form for several years after birth.
Gases and gas exchange Transfer of gases through the airways
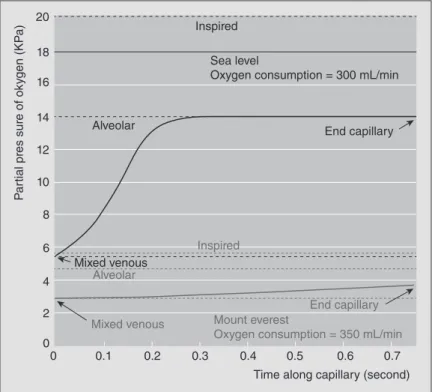
The alveoli in the respiratory zone of the lungs make up a total surface area of around 75 m2 (Pavelka & Roth, 2005). The PO2 of the red blood cells at the initial part of the pulmonary capillary is 40 mmHg.
TRANSPORT OF GAS IN THE RED BLOOD CELL Oxyhemoglobin
The oxygen saturation of Hb is the amount of oxygen bound to Hb divided by the oxygen capacity. As a result, a shift to the right leads to a greater removal of oxygen for a given PO2.

Carboxyhemoglobin
Carbon dioxide binds to Hb at the α-amino group and forms carbaminohemoglobin, the third form of CO2 carried in the blood (Guyton & Hall, 2006). This causes a change in the protein, which facilitates the release of oxygen, which shifts the oxygen dissociation curve to the left, and is known as the Bohr effect.
ACID–BASE BALANCE
In metabolic alkalosis, the respiratory system tries to compensate by hypoventilating and retaining CO2, thereby lowering the pH closer to 7.4. However, during respiratory acidosis, the kidney compensates by retaining HCO3−, mostly in the proximal tubule of the kidney, and by excreting H+ ions.
RESPIRATORY MECHANICS
However, these muscles must overcome the inward rebound of the chest wall back to the resting position. The pressure required to empty the lungs must overcome the outward displacement of the chest wall to the resting position.

Static properties: Compliance and elasticity
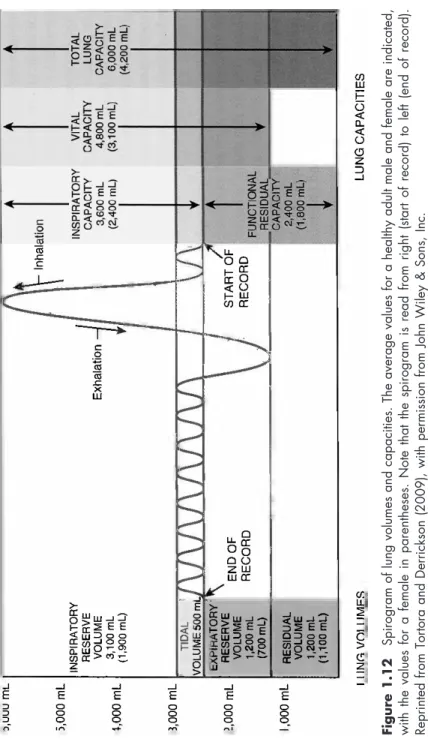
An appreciation of the terminology of different lung volumes is required before the dynamics of ventilation can be understood. TLC is the volume at which inspiration ceases because the inspiratory muscles cannot overcome the inward recoil of the chest wall.
Muscles of breathing Inspiration
Paralysis of the diaphragm produces a paradoxical movement, in which the diaphragm moves upward after inspiration with a drop in intrathoracic pressure. At the end of inspiration, the elastic properties of the stretched alveoli are such that the alveolar pressure is greater than atmospheric pressure, allowing air to flow out of the lungs (see Figure 1.11).
Surface tension properties of the lung
However, the repulsive forces of the two ends of DPCC resist this attraction, reducing the surface tension. Due to the properties of surfactants, smaller alveoli have lower surface tension, which normalizes the alveolar pressure throughout the lung.
Airway resistance
The decreased severity and incidence of RDS leads to a decrease in the need for surfactant therapy, supplemental oxygen, and mechanical ventilation (National Institute of Child Health and Human Development, 1994). Mutations in the adenosine triphosphate (ATP)-binding cassette gene (ABCA3) in neonates result in lethal surfactant deficiency.
Regional differences of the lung
CONTROL OF VENTILATION
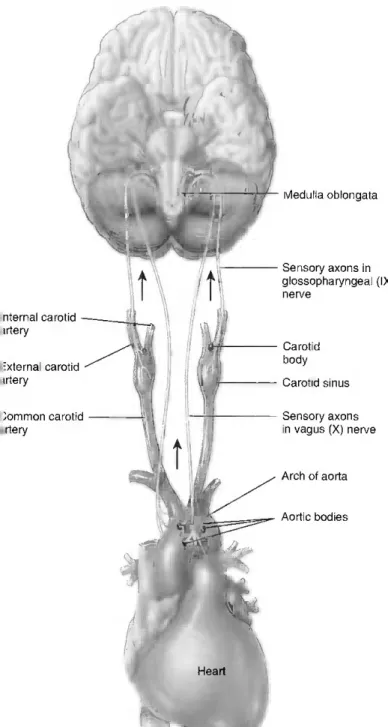
Once in the CSF, the pH will decrease with an increase in H+ ions, stimulating chemo-receptors. The pneumotaxic center is located in the upper pons and sends inhibitory impulses to the dorsal medulla, shortening inspiration and, as a result, leading to an increase in the respiratory rate.
The apneustic center is located in the lower back and participates in the transition between inhalation and exhalation. Its name comes from the fact that when it sends stimulating impulses to the spinal cord, it causes a lengthening of the breath, resulting in long, deep breaths.
Pediatric respiratory health history and physical assessment
RESPIRATORY HEALTH HISTORY AND PHYSICAL EXAMINATION
Therefore, at this stage, the nurse must clearly explain what will happen and why. For this age group, the nurse should re-explain what will happen during the examination and allow children to verbalize their symptoms.
Respiratory health history
The nurse must determine whether the child needs supplemental oxygen or mechanical ventilation during the neonatal period. Finally, it is important to consider your child's vaccination history to determine if vaccinations are up to date.
Physical examination
The chest should be palpated for pulsations, tenderness, depressions and abnormal movements (Seidel et al., 2003). In addition, if the child is old enough, he or she should be instructed to breathe with his/her mouth open.

Principles of lung therapeutics
PRINCIPLES OF LUNG THERAPEUTICS
BRONCHODILATORS
Short-acting β 2 -agonists Mechanism of action
The pharmacological activity is due to the (R)-enantiomer, and the (S)-enantiomer was originally thought to be essentially inactive due to the 100- to 1000-fold potency difference between the (R)- and (S)-enantiomers (Lotvall et al., 2001; Waldeck, 1999). Racemic albuterol and levalbuterol produce equivalent bronchodilation and effects on serum glucose and serum potassium at equivalent doses of the (R)-enantiomer (Lotvall et al., 2001).
Long-acting bronchochodilators Mechanism of action
Long-acting β2 agonists should only be used long-term in patients whose asthma cannot be adequately controlled with asthma control medications. Adverse effects associated with acute use of long-acting β2 agonists are the same as for short-acting β2 agonists.
Anticholinergics Mechanism of action
Ipratropium bromide is a non-selective antagonist at the M1, M2 and M3 receptors and is a quaternary ammonium compound that is poorly absorbed across the blood-brain barrier and therefore has few systemic effects compared to atropine. The available products include ipratropium bromide (Atrovent HFA and Combivent [combination of ipratropium and albuterol] as an MDI, and the combination of ipratropium and albuterol (DuoNeb, various generics available) as a solution for nebulization and tiotropium bromide (Spiriva HandiHaler) as a DPI .
INHALED CORTICOSTEROIDS Mechanism of action
Common indications
Common adverse effects
Changes in bone mineral density are unlikely to occur in children treated with low to medium doses (EPR 3, 2007). Suppression of the hypothalamic-pituitary-adrenal axis is unlikely to occur in patients on low to moderate doses of inhaled corticosteroids (EPR 3, 2007).
Generic and brand names
There appear to be no differences between inhaled corticosteroids in the effect on linear growth. Glucose homeostasis is unlikely to be affected by inhaled corticosteroid doses up to 1000 µg/day (EPR 3, 2007).
LEUKOTRIENE MODIFIERS Mechanism of action
Zafirlukast (LTD4 inhibitor at the CysLT1 receptor) is indicated for the prophylaxis and chronic treatment of asthma in adults and children 5 years of age and older. Zileuton (a 5-lipoxygenase inhibitor) is indicated for the prophylaxis and chronic treatment of asthma in adults and children 12 years of age and older.
OTHER ANTI-INFLAMMATORY DRUGS AND IMMUNE MODULATORS
Zileuton may cause liver dysfunction, and monitoring of liver function is currently recommended before initiating treatment: once monthly for the first three months, every two to three months for the remainder of the first year, and periodically thereafter for patients receiving long-term therapy. Zileuton Prescribing Information, 2009). Leukotriene modifiers are available as montelukast (Singulair), zafirlukast (Accolate), and zileuton (Zyflo and Zyflo CR).
Cromolyn
Periodic testing of serum transaminases has not been proven to prevent serious damage, but it is generally believed that early detection of drug-induced liver damage along with prompt withdrawal of the suspected drug increases the likelihood of recovery (Zafirlukast Prescribing Information, 2009). .
Omalizumab Mechanism of action
It is not indicated for other allergic conditions, acute bronchospasm or for patients under 12 years of age. Anaphylaxis is a potentially harmful effect; therefore, patients should be observed for a period of time after dosing.
COUGH SUPPRESSANTS Dextromethorphan
Codeine
Diphenydramine, promethazine, and other first-generation antihistamines
EXPECTORANTS Guaifenesin
DECONGESTANTS
Oral decongestants Mechanism of action
Stimulation of postcapillary α1-adrenergic receptors causes vasoconstriction of postcapillary venules in the nasal mucosa (Johnson & Hricik, 1993). Congestion is caused by increased blood volume, which increases the volume of the nasal mucosa.
Topical decongestants Mechanism of action
INHALED ANTIBIOTICS
Mechanism of action
Nebulized colistimethate sodium can often cause bronchospasm, cough, and throat irritation; inhaled β2-agonist can be administered prophylactically or for the treatment of these effects (Heijerman et al., 2009). Inhaled tobramycin is available as TOBI; colistimethate sodium is available as Coly-Mycin M and generic products; and aztreonamlysine is available as Cayston.
DELIVERY DEVICES (SEE TABLE 3.1) MDIs (See Figure 3.1)
DPIs (See Figure 3.2)
If you use a face mask, it should fit tightly and allow at least five breaths per trigger. From left to right: MDI, breath-triggered MDI, nebulizer cup with face mask, nebulizer cup with mouthpiece, holding chamber with valve and mouthpiece, valve holding chamber with face mask.

Nebulizers (See Figure 3.1)
Compared to pressurized MDIs, DPIs do not require the patient to coordinate activation of the device with inhalation (Kelly, 1999a). Some DPIs (ie, Diskus) are more robust in terms of the inspiratory flow rate required to deliver the drug, so that delivery is still effective even at flow rates.
Holding chambers (See Figure 3.1)
13 cm length is required for a spacer as smaller devices will actually reduce drug delivery (Dolovich et al., 2000). This is particularly important for children with tidal volumes that do not exceed the volume of the holding chamber (Dolovich et al., 2000).
INHALER TEACHING DEVICE (SEE FIGURE 3.3)
Note the inspiratory flow rate opposite the red indicator on the cylinder of the DIAL. Compare the inspiratory flow rate to the target flow rate of the selected device (Education/Clinics, n.d.).
PEAK FLOW METERS/FORCED EXPIRATORY VOLUME IN THE FIRST SECOND METERS (SEE FIGURE 3.3)
Use of regularly scheduled albuterol treatment in asthma: genotype-stratified, randomized, placebo-controlled crossover study. Ipratropium bromide: a review of its pharmacological properties and therapeutic efficacy in asthma and chronic bronchitis.
Neonatal lung disease
Apnea of prematurity and bronchopulmonary dysplasia
NEONATAL LUNG DISEASE
Apnea of prematurity Epidemiology
The medical care of a baby with apnea of prematurity must be systematic and comprehensive. Nursing care of an infant with BPD is multifactorial due to the many conditions and complications associated with BPD.
Lower airway disease
LOWER AIRWAY DISEASE
All too often the decision is made to treat all children with lower respiratory tract symptoms with an antibiotic. It is crucial for practitioners to remember that viral infections remain the most common cause of lower respiratory tract disease.
Common viral agents that cause acute lower respiratory infections in children
One of the most difficult challenges for the clinician is determining whether a given illness is viral or bacterial. The pathophysiology of the virus is similar to that of RSV and is found to be the causative virus in 5-15% of infant bronchiolitis.
Common bacterial agents that cause ALRIs in children
The clinical presentation is also similar to that of RSV, showing symptoms such as rhinorrhea, congestion, cough, tachypnea and dyspnea (Maranich & Rajnik, 2009).
Common lower airway diseases in children
Careful and frequent clinical evaluation of the child is essential for the successful treatment of bronchiolitis. Infiltration of leukocytes into the respiratory tract contributes to the appearance of purulent discharge.
CONCLUSION
Virus-specific IgE enhances airway responsiveness to respiratory syncytial virus reinfection in newborn mice. Palivizumab, a humanized respiratory syncytial virus monoclonal antibody, reduces hospitalization from respiratory syncytial virus infection in high-risk infants.
Upper airway disorders
ANATOMICAL AND PHYSIOLOGICAL CONSIDERATIONS OF THE PEDIATRIC AIRWAY
The cricoid cartilage is located below the thyroid cartilage and is the first ring of the trachea. The muscles of the larynx are responsible for the elevation and depression of the larynx (extrinsic muscles) as well as the movement of the vocal cords (intrinsic muscles) (Healy, 1989).
ASSESSMENT OF THE CHILD WITH AIRWAY DIFFICULTIES
The posterior wall of the trachea (open part of C) consists of smooth muscle and connective tissue that allows the diameter of the trachea to change. Pouseuille's law states that the flow within the system is related to the radius of the pipe to the fourth power.
History
The degree (loudness) of stridor or stertor is not a reliable indicator of the severity of obstruction (Papsin, Abel, & Leighton, 1999). The quality of voice and crying varies from normal to muffled with oronasopharyngeal obstruction (oropharyngeal obstruction—hot potato voice;.

Endoscopy
If possible, try to reassess when the child is awake or asleep, agitated, during physical exertion, with changes in position, and with feedings.
Diagnostic imaging
Laryngeal obstruction naturally affects the voice, ranging from weak to hoarse to aphonia, depending on the location and extent of the obstruction in the larynx. Videostoboscopy of the vocal cords is useful in providing information about the anatomy and movement of the vocal cords.
ANOMALIES OF THE LARYNX AND TRACHEA Laryngomalacia
It can identify external airway compression, foreign bodies, strictures and tracheoesophageal fistulas and can identify gastroesophageal reflux (but there is a high percentage of false negative results). Anatomy is otherwise normal, including normal structure and function of the vocal cords and a free, unobstructed airway on exhalation.

Vocal cord disorders
The use of antireflux medications in infants without overt symptoms of reflux is advocated by some physicians. Babies with laryngomalacia who show symptoms of severe breathing problems and/or growth retardation will require surgical treatment.
Immobility, paralysis, and dysfunction VCP
If the unilateral cord is immobile in the paramedian position, then cord opposition is absent and the baby may have a weak cry or voice. VCD occurs when there is abnormal movement of the vocal folds in the absence of other diseases.
Vocal cord masses and lesions
Primary tracheomalacia is an intrinsic condition caused by an abnormality in the wall of the airways (Healy, 2000). The child will outgrow the symptoms with the maturation of the tracheal rings and the growth of the airways.
UPPER AIRWAY INFECTIONS
Families also need to have a sense of control in caring for their child during long-term hospitalizations. Nurses are instrumental in teaching families and caregivers the skills required to care for their child when they move home.
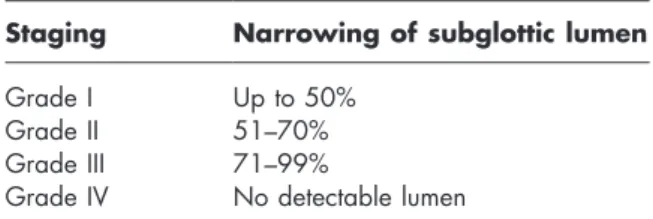
Laryngotracheobronchitis (Croup)
The virus is transmitted via the inhalation route and infects the epithelial cells of the mucous membrane of the larynx and trachea, subsequently resulting in swelling and inflammation. This is due to swelling and inflammation of the airways in the subglottic region.
Epiglottitis
The epidemiology is changing and there has been a shift in the average age of the child to ages 6 and 7 (Gorelick & Baker, 1994). Additionally, allowing familiar objects, such as pictures or a favorite blanket, will help comfort the child.
SINUSITIS AND RHINITIS
Observing the child from across the room before approaching him or her is helpful in determining the actual degree of distress. The child is typically comforted most by his or her parents or primary caregivers and will benefit from their continued presence if possible.
Anatomy of the nasal cavity and sinuses
Sinusitis Epidemiology
Therefore, the source of the cough must be viewed holistically (Boat & Green, 2007). A medial subperiosteal abscess of the orbit is the most common serious complication of sinusitis in children (Pereira, Mitchell, Younis, & Lazar, 1997).
Rhinitis
But in children with chronic sinusitis, there is a greater need for further education and reinforcement of the treatment plan. Allergic rhinitis represents an inflammatory condition of the nasal mucosa resulting from an excessive immunoglobulin E (IgG)-mediated immune response to inhaled allergens (Luong & Roland, 2008).