Proses Korespondensi Artikel
Judul : Pesticide Exposure and Stunting among Children in Agricultural Areas Artikel No. : C-5
No. Keterangan Tanggal Halaman
1 Submission 4 Agustus 2018 2
2 Reviewer’s Comments(major revision) 19 Desember 2018 3
3 Revised 1 Januari 2019 5
4 Accepted 2 Januari 2019 30
5 Publish Januari 2019 31
[IJOEM] Submission Acknowledgement (Ms #1428)
Dari: Farrokh Habibzadeh, MD, ([email protected]) Kepada: [email protected]
Tanggal: Sabtu, 4 Agustus 2018 09.38 WIB
F. Habibzadeh, MD,
The IJOEM, Editorial Office,
Shiraz NIOC Polyclinics, Eram Blvd, Shiraz 71438, Iran
Tel/Fax: +98-71-3225-2258 E-mail: [email protected] Web: www.theijoem.com
Manuscript ID: 1428 Dear Suhartono Suhartono,
We wish to acknowledge receipt of your manuscript entitled "Exposure of pesticide as the risk factors for stunting on school-aged children in
Indonesian agricultural areas" to The International Journal of Occupational and Environmental Medicine (The IJOEM). This manuscript will have the prompt attention of our Editorial Board. With the online journal management system that we are using, you will be able to track its progress through the
editorial process by logging in to the journal Web site:
Manuscript URL:
http://www.theijoem.com/ijoem/index.php/ijoem/author/submission/1428 Username: suhartono
If you have any questions regarding the manuscript, please contact me. It is understood that this article is submitted exclusively to the The
International Journal of Occupational and Environmental Medicine. Thank you for your submission.
Best Regards, F. Habibzadeh, MD, Editor, The IJOEM
Follow us on Twitter @TheIJOEM
Yahoo Mail - [IJOEM] Submission Acknowledgement (Ms #1428) https://mail.yahoo.com/d/search/keyword=ijoem/messages/5248?guce_re...
1 of 1 21/04/2021, 5:45
1. Submission
[IJOEM] Decision Letter Ms #1428
Dari: Dr. Farrokh Habibzadeh ([email protected]) Kepada: [email protected]
Tanggal: Rabu, 19 Desember 2018 17.27 WIB
Ms Title: "Exposure of pesticide as the risk factors for stunting on school-aged children in Indonesian agricultural areas"
Ms #1428
Dear Dr. Suhartono Suhartono,
Now, I have the comments of reviewers (summarized at the bottom of this e-mail). Please either consider their comments and revise your manuscript accordingly or provide reasonable answers to the comments. Please send us the revised version within next two weeks.
Best Regards, F. Habibzadeh, MD, Editor, The IJOEM
=======================
REVIEWERS' COMMENTS
=======================
Reviewer 1:
Abstract
-Author should be added the recommendation from your finding in the conclusion part
Introduction
-Author should be added the objective of this research in this last paragraph of introduction part
Material and methods
-Author should be added the description of the sample size ratio between case and control
-Author should be added inclusion and exclusion criteria of participant Discussion
-Author should be added the reason for no difference in the proportion of anemia incidence between stunting and normal group
-Author should be added the recommendation from your finding in the last paragraph of discussion part
--- Reviewer 2:
1) In the Abstract Objective, it is mentioned that this study was conducted
"to prove pesticide exposure as the risk factor for stunting among children in agricultural areas." This is in fact a bias. You should mention "this
Yahoo Mail - [IJOEM] Decision Letter Ms #1428 https://mail.yahoo.com/d/search/keyword=ijoem/messages/7387?guce_re...
1 of 2 21/04/2021, 7:53
2. Reviewer’s Comments (major revision)
study was conducted to determine if exposure to pesticides is associated with stunting in children..."
2) In the Methods, this is not "multivariate logistic regression". It is
"binary logistic regression". Multivariate logistic is when you have more than one dependent variable.
3) In the Introduction, it is mentioned that "Stunting prevalence in
school-age children (5-12 years) in Indonesia reached 30.7%". Please provide references.
4) At the end of the Introduction, please clearly state your research question/hypothesis.
5) In the Methods section, based on the provided presumptions, the minimum sample size is 53, NOT 43. Please recheck.
6) In the Methods, it is mentioned that "Determination of cut-off point for the levels of IGF-1 using the Receiver Operating Characteristic (ROC) (Figure 2)." Cut-off value for diagnosis of WHAT condition? How the cut-off value was determined (based on what assumptions? Maximizing the Youden's index? Minimizing the distance from the upper right corner?, or a more complex method). For more information you may refer to: On determining the most appropriate test cut-off value: the case of tests with continuous
results. Biochem Med (Zagreb). 2016 Oct 15;26(3):297-307.
EDITORIAL NOTE: If the manuscript is accepted, we may need the raw data to reproduce the figure.
7) It is mentioned that the logistic regression analysis was used to adjust (control) for some confounding variables. Please name the variables for which the model was adjusted for?
8) Table 2, The SDs for TSH and IGF-1 exceed half of their corresponding means. This implies that the distributions of these variables are unlikely to be normal. Therefore, you need to present the results as median and IQR rather than mean and SD; furthermore, you need to use a non-parametric test, say Mann-Whitney U test instead of Student's t test to compare these values between the two study groups.
9) Table 3, Omit the column for p value. Having the 95% CI of ORs is enough.
10) Table 4, Omit Columns for B, SE, and p value. Those information are already included in other elements in the Table.
Yahoo Mail - [IJOEM] Decision Letter Ms #1428 https://mail.yahoo.com/d/search/keyword=ijoem/messages/7387?guce_re...
2 of 2 21/04/2021, 7:53
Revised Version Kartini's Manuscript (Ms # 1428)
Dari: Suhartono Damas ([email protected]) Kepada: [email protected]
Tanggal: Selasa, 1 Januari 2019 12.00 WIB
Manuscript Apoina Kartini_IJOEM_revised.docx 148.9kB
Response to Reviewers-Kartini's manuscript.docx 20.7kB
Raw data of IGF-1 level.xlsx 12.9kB
Output of ROC analysis.docx 40.5kB
Dear Dr. Farrokh Habibzadeh
We are writing to present the revised version of our manuscript (Ms #1428) the previous entitled
“Exposure of pesticides as the risk factors for stunting on school-aged children in Indonesian agricultural areas” to The International Journal of Occupational and Environmental Medicine.
We changed the title of the manuscript into “Association between pesticide exposure and stunting among children in agricultural areas” to be consistent with the research objectives.
I would like to thank the reviewers and you for the very helpful constructive criticism of our original research article. The reviewers’ comments allowed us to take a fresh look at our original submission. As a result, we have made considerable changes to the layout, language and content of the manuscript.
Our responses to all reviewers’ comments are presented in a file of Response to Reviewers-Kartini’s manuscript and we have uploaded with another files in this email (Manuscript Apoina
Kartini_IJOEM_revised, Raw data of IGF-1 level, Output of ROC analysis).
We would also like to express my appreciation to you for providing us with a chance to revise and resubmit our manuscript.
Kind regards,
Suhartono
Virus-free. www.avast.com
Yahoo Mail - Revised Version Kartini's Manuscript (Ms # 1428) https://mail.yahoo.com/d/search/keyword=ijoem/messages/7624?guce_re...
1 of 1 21/04/2021, 6:07
3. Revised
1 We thank the reviewers for their thoughtful comments.
Reviewer 1: Author reply
Reviewer Evaluation (1) Abstract
Author should be added the
recommendation from your finding in the conclusion part
Change made
(2) Introduction
Author should be added the objective of this research in this last paragraph of
introduction part
Change made
(3) Material and methods
a. Author should be added the
description of the sample size ratio between case and control
b. Author should be added inclusion and exclusion criteria of participant
Some sentences have been inserted in material and method section as follows:
a. The sample ratio between case and control was about 1:2, and it have been describe in material and methods b. We have been describe inclusion and
exclusion of participants (4) Discussion
Author should be added the reason for no difference in the proportion of anemia incidence between stunting and normal group
Author should be added the
recommendation from your finding in the last paragraph of discussion part
We have been added discussion about no difference in the proportion of anemia incidence between case and control group Recommendations have been added in the last paragraph of discussion part
2
Reviewer 2: Author reply
Reviewer Evaluation
1) In the Abstract Objective, it is mentioned that this study was conducted "to prove pesticide exposure as the risk factor for stunting among children in agricultural areas." This is in fact a bias. You should mention "this study was conducted to determine if exposure to pesticides is associated with stunting in children..."
Change made
2) In the Methods, this is not "multivariate logistic regression". It is "binary logistic regression". Multivariate logistic is when you have more than one dependent variable.
Change made
3) In the Introduction, it is mentioned that
"Stunting prevalence in school-age children (5-12 years) in Indonesia reached 30.7%". Please provide references
Change made
4) At the end of the Introduction, please clearly state your research
question/hypothesis
Hypothesis has been inserted at the end of introduction paragraph: ‘there is any association between pesticide exposure and stunting among children in agricultural areas’
5) In the Methods section, based on the provided presumptions, the minimum sample size is 53, NOT 43. Please recheck.
We have rechecked the minimum sample size needed by this study based on the provided presumption was 49 samples.
However, in this study, we just got 48 cases as our subjects for the case group because we have excluded one participant due to incomplete interview data (Figure 1). In addition, we have replaced number of 43 by 49 samples in the manuscript.
6) In the Methods, it is mentioned that
"Determination of cut-off point for the levels of IGF-1 using the Receiver Operating Characteristic (ROC) (Figure
Change made
We use a method of maximizing the Youden’s index to determine the cut-off value of IGF-1 level
3 2)." Cut-off value for diagnosis of WHAT
condition? How the cut-off value was determined (based on what
assumptions? Maximizing the Youden's index? Minimizing the distance from the upper right corner?, or a more complex method). For more information you may refer to: On determining the most appropriate test cut-off value: the case of tests with continuous results.
Biochem Med (Zagreb). 2016 Oct 15;26(3):297-307
We have revised Figure 2
EDITORIAL NOTE: If the manuscript is accepted, we may need the raw data to reproduce the figure.
We have sent the raw data in the form of Excel file together with the revised manuscript
7) It is mentioned that the logistic
regression analysis was used to adjust (control) for some confounding
variables. Please name the variables for which the model was adjusted for?
Change made:
“Analysis to assess the risk of pesticide exposure for stunting were done by including confounding variables, i.e. IGF-1 level in binary logistic regressions”
8) Table 2, The SDs for TSH and IGF-1 exceed half of their corresponding means. This implies that the distributions of these variables are unlikely to be normal. Therefore, you need to present the results as median and IQR rather than mean and SD;
furthermore, you need to use a non- parametric test, say Mann-Whitney U test instead of Student's t test to
compare these values between the two study groups.
Change made
9) Table 3, Omit the column for p value.
Having the 95% CI of ORs is enough
Change made
10) Table 4, Omit Columns for B, SE, and p value. Those information are already included in other elements in the Table
Change made
1 Title Page
Type of manuscript:
Original Research Article Manuscript title:
Association between pesticide exposure and stunting among children in agricultural areas Authors’ full names and affiliations:
Apoina Kartini1, Hertanto W Subagio2, Suharyo Hadisaputro3, Martha I Kartasurya1, Suhartono4, Budiyono4
1Department of Public Health Nutrition, Faculty of Public Health, Diponegoro University, Semarang, Indonesia
2Department of Nutrition, Faculty of Medicine, Diponegoro University, Semarang, Indonesia
3Department of Internal Medicine, Faculty of Medicine, Diponegoro University, Semarang, Indonesia
4 Department of Environmental Health, Faculty of Public Health, Diponegoro University, Semarang, Indonesia
Corresponding author:
Suhartono, Department of Environmental Health, Faculty of Public Health, Diponegoro University, Semarang, Indonesia, Jalan Prof. Soedarto, SH Tembalang, Semarang 1269, Indonesia. Tel:+62811275410, email: [email protected]
Running title:
Association between pesticide exposure and stunting
2 Association between pesticide exposure and stunting among children in agricultural areas
Abstract
Background: Stunting prevalence among school-aged children in Indonesia was high (30.7%).
Pesticides have been massively used in Indonesian agricultural areas.
Objective: This study was conducted to determine if exposure to pesticides is associated with stunting among children in agricultural areas
Methods: This case-control study had 160 children aged 8-12 years (48 cases and 112 controls) as the subjects. Exposure of pesticide was measured based on the history of pesticide exposure since the fetus, infant, and child. Stunting was determined as height for age Z-scores (HAZ) <
-2SD. Other variables measured were thyroid stimulating hormone (TSH), insulin-like growth factor-1 (IGF-1), hemoglobin, zinc, albumin, nutrient adequacy level (energy and protein), history of infection, low birth weight (LBW), and mother’s height. Data were analyzed by mean/median difference test, Chi-square tests, Odds Ratio calculation, and binary logistic regression.
Results: There were no difference in characteristics and confounding variables between the cases and controls (p>0.05), except for the median IGF-1 level, which was lower in the cases (66.73 ng/mL) compared to the controls (112.57 ng/mL), p-value < 0.001. ‘High’ level of pesticide exposure (p=0.029) and ‘low’ IGF-1 levels (p<0.001) significantly associated with stunting. These both variables were being risk factors for stunting in children with adjusted OR=3.90 (95% CI=1.15-13.26) and 8.35 (3.65-19.14) respectively.
Conclusion: There was an association between pesticide exposure and stunting among children in agricultural areas. Pesticide exposure could be a risk factor for the occurrence of stunting. This result provides strong support for taking action in the prevention or reduction of pesticide exposure in children.
Keywords: pesticide exposure, stunting, children, agricultural areas
3 Introduction
Stunting, or poor linear growth (low length- or height-for-age) in young children is the result of poor nutritional intake, in terms of both quality and quantity, high morbidity, or a combination of both. These conditions are often found in low and middle-income countries.1 Low consumption of macronutrients and micronutrients, especially during the growth period, will disrupt the process, and result in stunting.2 In addition to food consumption factors, stunting is also influenced by genetic factors,3,4 recurrent (chronic) infections, such as acute respiratory infections (ARI) and diarrhea.5 Normal growth is the result of a complex interaction of genetic factors, nutritional factors, and hormonal factors. These three factors work together at the cellular level resulting in growth. Growth hormone (GH) plays an important role in this process, and other hormones (including thyroid, sex steroid, and glucocorticoid) and psychosocial factors also play a role in growth, partly through interaction with hypothalamopituitary-GH- IGF (insulin-like growth factor) axis.6
History of the growth of children is a sensitive indicator of the health and well-being, and therefore it is an important component of healthy child care. Endocrine disorders include important things to think about in abnormal growth in children.3 The problem of stunting in children should be a concern because it is a reflection of the quality of human resources in the future. Some studies showed an association between stunting with impaired cognitive function7,8 and the learning achievement of children of school age.9 Impaired cognitive function in children with stunting, in the long term, will affect their economic potential. Stunting conditions in childhood generally continue into adulthood and will affect their work capacity and productivity.10
Stunting prevalence in school-age children (5-12 years) in Indonesia reached 30.7%.11 The prevalence of stunting in children of the same age in Central Java was 28.6%, while in Brebes District reached 40.7%, the highest among the other districts in Central Java.11 Brebes
4 District is one of the districts in Central Java province that relies on agricultural sector as the source of local revenue, an especially onion that requires pesticides spraying 2-3 times per week, even everyday in the rainy season.12
Toxic substances exposure from the environment might also interfere the synthesis of Insulin-like Growth Hormone 1 (IGF-1).13 Research in Spain showed that serum IGF-1 levels of boys aged 6-15 years exposed to organochlorine pesticides were significantly lower than the non exposed.14 Low IGF-1 levels in serum were associated to growth disorders. The results of the study in preschool children in Senegal show that there was a relationship between IGF-1 levels and stunting.15
A study in Brebes District showed that the history of organophosphate pesticide exposure was the risk factor for hypothyroidism in women at child-bearing age in agricultural areas.12 Exposure to organophosphate pesticides might cause neurodevelopment disorders.16,17 Pesticides exposure in children may occur directly, because of their involvement in agricultural activities, or indirectly through contact with the environment: water, soil, or food contaminated by pesticide residues. The study results in one of the primary schools in Brebes onion farming areas indicated that 81.3% of the students were involved in agricultural activities, such as finding pests, helping with the harvest, and removing onions from stalks.18 Our previous study concluded that a history of pesticide exposure is a risk factor for thyroid dysfunction in children living in agricultural areas.19 Meanwhile, another our previous study also proved that children whose fathers work as farmers are more likely at risk of suffering goiter than those who are not farmers.20 Pesticide is one of the chemicals classified as endocrine disrupting chemicals (EDCs),21 and its exposure to human can interfere with the function of hormones, such as thyroid hormones, insulin, and IGF-1 which are very important in the child's growth process.15,22 This study was conducted to determine if exposure to pesticides is associated with stunting in children in agricultural areas and to determine it as a risk factor. Therefore, the
5 hypothesis of this study was there is any association between pesticide exposure and stunting among children in agricultural areas.
Materials and Methods
Study Design, Location and Subjects
This study used a case-control design to show pesticide exposure as the risk factor for stunting in children in agricultural areas. The study was conducted in four primary schools in Bulakamba Sub-district as this area had high prevalence of stunting in school children and the onion farming area is quite wide.
The minimum sample size was calculate using the case-control formula from Lemeshow et al;23 so with a significance level of 0.05, research power of 80%, pesticide exposure proportion in the non-stunting children of 22.9% and Odds Ratio (OR) of 3,26,5 the minimum sample size obtained for each case and control group were 49. The inclusion criteria for the subjects were 8-12 years old, no abnormalities of the spine (such as scoliosis), and had not menarche yet for the female subjects. Meanwhile, the exclusion criteria were refuse to take blood samples and incomplete interview data.
The measurement of child height for screening of stunting was conducted on 238 subjects (elementary students) consisted of 119 (50.0%) males and 119 (50.0%) females. Based on WHO growth standard (2006),24 52 subjects (21.8%) were classified as stunting and 186 (78.2%) non-stunting. Of the 52 stunting subjects, 3 subjects refused to take blood samples and 1 subject had incomplete data on interviews, so there were 48 subjects with stunting become as case group. Meanwhile, of 186 non-stunting subjects, 48 subjects refused to take blood samples and 27 subjects had incomplete data on interviews, so there were 112 non-stunting subjects become control group (Figure 1). Based on the minimum sample size calculation, this study required at least 49 participants for each group. Notwithstanding, we just analyzed data from 48 participants for the case group and 112 participants for the control group. The ratio between
6 the case and the control group was approximately 1:2 in accordance with the theory of sample size comparison for cases and controls in the case-control study.25
Figure.1. Selection of study subjects
Data Collection and Methods of Measurement
Subjects and mothers/caregivers were interviewed in this study. Structured questionnaires were used to collect characteristics data (sex, age, parents’ educational and occupational status), pesticide exposure, history of acute respiratory infections and diarrhea in the last month, and history of low birth weight/LBW (less than 2500 grams). History of pesticide exposure is a composite variable of three sub-variables: 1) mother’s involvement in agricultural activity during pregnancy; 2) subjects were brought to farm by the mother, at infant and /or toddler period; and 3) subjects’ involvement in agricultural activities at school age period. In each of the three sub-variables, they were categorized into 1) ‘high’ exposure history,
1017 children in four elementary school
238 children 8-12 years old was
measured height
Stunting (n=52) Normal (n=186)
Cases (n=48) Controls (n=112) Grade 4 and 5 student
(purposive)
3 refused taken blood samples
48 refused taken blood samples
Stunting (n=49) Normal (n=138)
1 incomplete interview data
27 incomplete interview data
7 when they answered "Yes" in all the three time periods (exposed when pregnant women, infants/toddlers, and school age); 2) ‘moderate’ exposure history, when they answered "Yes"
at two time periods; 3) ‘low’ exposure history, when they answered "Yes" at any one time period; 4) unexposed, when they answered none in the three time periods.
The age of the children was derived from the school register. Measurements of height were taken by two postgraduate nutrition students who were trained on the standard procedure of measuring height. The height was measured using a Seca® 213 stadiometer (to the nearest 0.1 centimeters). The measurements were done on the subject with the erect position, without shoes and with the eyes looking horizontally and the feet together on a horizontal level. Stunting was defined as HAZ below minus two standard deviation (-2 SD) , and normal was defined as HAZ equal to minus two (-2 SD) until two (2 SD) of WHO Child Growth Standards.24 The mother's height was measured with a stadiometer in the same way as the measurements for the children.
Non-fasting peripheral venous blood samples were obtained from 160 students in the morning from 09.00 to 11.00. a.m. TSH levels were measured with a mini VIDAS® (bioMérieux S.A.), that is a compact automated immunoassay system based on the Enzyme Linked Fluorescent Assay (ELFA) principles. TSH levels greater than 4.5 mIU/mL was considered as hypothyroidism.22 Serum concentration of IGF-1 was measured with the Quantikine® Human IGF-I ELISA kit (R&D Systems). The cut-off value of IGF-1 levels for the incidence of stunting was determined using the Receiver Operating Characteristic (ROC) curve analysis with maximizing the Youden’s index (maximum vertical distance from 45o diagonal line)26,27 and we found the cut-off value was 97.325 ng/mL, with sensitivity and specificity were 0.652 and 0.833 respectively (Figure 2). Based on these analyses, IGF-1 levels was categorized as ‘low’ if less than 97.325 ng/mL.
8 Figure 2. ROC curve for cut-off IGF-1 level
Hemoglobin was measured using the KX-21 automated hematology analyzer (Sysmex).
Anemia was determined using cut-off point of hemoglobin less than 12 g/dL.28 Zinc serum concentrations were measured using Shimadzu® Atomic Absorption Flame Emission Spectrophotometers (AAS) Model: AA-6401F. Zinc serum fewer than 70 μg/dL was categorized as low.29 Serum albumin levels were measured using the Bromocresol green (BCG) method. Serum albumin concentration of less than 3.5 g/dL were considered as low.30
The amount of daily energy intake of subjects in kilocalories and daily protein intake in grams as measured by interview method using semi quantitative food frequency questionnaire (FFQ) instrument then computed using the Nutri-Survey programme. Energy and protein adequacy levels were categorized: low (<90% RDA/recommended dietary allowance) and
Max.
Youden’s index
9 sufficient (≥90% RDA). Iron adequacy levels were categorized: low (<77%
RDA/recommended dietary allowance) and sufficient (≥77% RDA).31 Statistical Analysis
Data were analyzed using SPSS for Windows software (version 18). For bivariate and multivariate analysis, descrete scale variables were transformed into categorical scales. The means and standard deviations of age, height, HAZ, TSH, IGF-1, hemoglobin, Zinc level in the case and control groups were compared using the mean difference test (Mann-Whitney and Independent t-test). Proportions were calculated for categorical variables, and they were compared using the Chi-square tests. Potential risk factors associated with stunting were identified by the odds ratios (ORs) and their 95% confidence intervals (CI). A multivariate analysis to assess the risk of pesticide exposure for stunting were done by including confounding variables, i.e. IGF-1 level in binary logistic regressions. Statistical significance was determined at 95% level of significance or p-value <0.05.
Ethics
Ethical approval and clearance were obtained from the Diponegoro University Medical Faculty Ethical Committee. The teachers, subjects, and parents were well-informed of the purpose and benefits of this study, and parents signed the informed consent forms.
Results
In the cases and controls, the largest proportion of subjects was 10 years old, respectively 41.7%, 34.8%. The mean birth weight of the subjects in the case group was 3008
± 539.6 grams while the control group was 3174 ± 532.9 grams. There were 4 mothers in the case group and 10 mothers in the control group who had no records and the mothers forgot the birth weight of the subjects. The mean mother’s height of cases and controls is almost the same as 150.2 ± 5.96 cm and 150.2 ± 5.65 cm respectively. There were some mothers who were not measured their height at the time of the study because the mother worked outside the study area.
10 The majority of father’s and mother’s had a low level of schooling. The highest proportion of mother’s occupations were farmers, in both cases and controls, 47.9% and 34.8% respectively.
The highest proportion of father’s occupations in the case group were farmers (43.8%), while in the control group were merchants (46.4%) (Table 1).
Table 1. Characteristics of the subjects
Variables Cases (n=48)
Mean ± SD
Controls (n=112) Mean ± SD
Age (years) 9.9±0.98 10.0±0.96
Height (cm) 123.8±4.81 134.9±6.22
HAZ (SD) -2.5±0.48 -0.8±0.75
Birth weight a (g) 3008±539.59 3174±532.91
Mother’s height b (cm) 150.2±5.96 150.2±5.65
n (%) n (%)
Sex
Male 25 (52.1) 55 (49.1)
Female 23 (47.9) 57 (50.9)
Mother’s Education level
Illiterate 1 (2.1) 4 (3.6)
Middle school or below 45 (93.7) 104 (92,8)
High school 2 (4.2) 4 (3,6)
Father’s Education level
Illiterate 0 (0.0) 1 (0.9)
Middle school or below 46 (95.8) 101 (90.2)
High school 2 (4.2) 10 (8.9)
Mother’s Occupations
Unemployed 7 (14.6) 30 (26.8)
Farmers 23 (47.9) 39 (34.8)
Merchants 13 (27.1) 34 (30.4)
Others 5 (10.4) 9 (8.0)
Father’s Occupations
Farmers 21 (43,8) 46 (41,1)
Merchants 20 (41,7) 52 (46,4)
Government employees 0 (0,0) 1 (0,9)
Others 7 (14,6) 13 (11,6)
a Cases=44, Controls=102; b Cases=37, Controls=75
There was no difference in the median of TSH between case group (3.31 mIU/mL) and control group (3.24 mIU/mL). The median IGF-1 in the case group were lower (66.73 ng/mL) than the control group (112.57 ng/mL). The proportion of low zinc levels in cases (9.7%) was
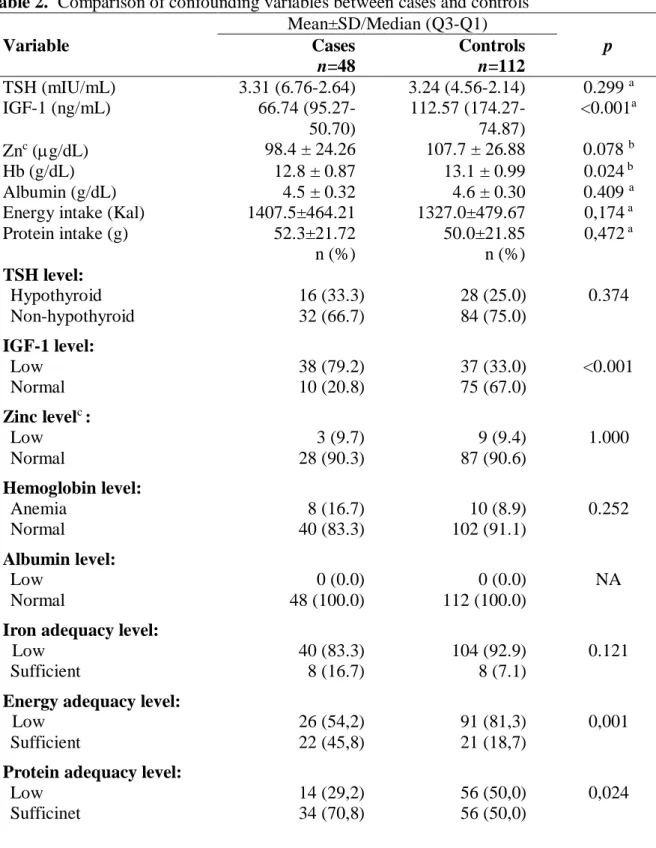
11 not different than the controls (9.4%). The proportion of anemia in the cases was higher (16.7%) than in the controls (8.9%), but not statistically significant (p=0.252). All subjects, both cases and controls had normal albumin levels. The majority of subjects in both groups did not have a history of chronic infection, 93.8% and 86.6% respectively, and low birth weight (LBW) (90.9% and 94.1% respectively) (Table 2).
Table 2. Comparison of confounding variables between cases and controls Mean±SD/Median (Q3-Q1)
Variable Cases
n=48
Controls n=112
p TSH (mIU/mL) 3.31 (6.76-2.64) 3.24 (4.56-2.14) 0.299 a
IGF-1 (ng/mL) 66.74 (95.27-
50.70)
112.57 (174.27- 74.87)
<0.001a
Znc (g/dL) 98.4 ± 24.26 107.7 ± 26.88 0.078 b
Hb (g/dL) 12.8 ± 0.87 13.1 ± 0.99 0.024 b
Albumin (g/dL) 4.5 ± 0.32 4.6 ± 0.30 0.409 a
Energy intake (Kal) 1407.5±464.21 1327.0±479.67 0,174 a
Protein intake (g) 52.3±21.72 50.0±21.85 0,472 a
n (%) n (%)
TSH level:
Hypothyroid 16 (33.3) 28 (25.0) 0.374
Non-hypothyroid 32 (66.7) 84 (75.0)
IGF-1 level:
Low 38 (79.2) 37 (33.0) <0.001
Normal 10 (20.8) 75 (67.0)
Zinc levelc :
Low 3 (9.7) 9 (9.4) 1.000
Normal 28 (90.3) 87 (90.6)
Hemoglobin level:
Anemia 8 (16.7) 10 (8.9) 0.252
Normal 40 (83.3) 102 (91.1)
Albumin level:
Low 0 (0.0) 0 (0.0) NA
Normal 48 (100.0) 112 (100.0)
Iron adequacy level:
Low 40 (83.3) 104 (92.9) 0.121
Sufficient 8 (16.7) 8 (7.1)
Energy adequacy level:
Low 26 (54,2) 91 (81,3) 0,001
Sufficient 22 (45,8) 21 (18,7)
Protein adequacy level:
Low 14 (29,2) 56 (50,0) 0,024
Sufficinet 34 (70,8) 56 (50,0)
12 History of infections:
Yes 3 (6.3) 15 (13.4) 0.300
No 45 (93.8) 97 (86.6)
History of LBWd :
Yes 4 (9.1) 6 (5,9) 0.728
No 40 (90.9) 96 (94.1)
a Mann-Whitney U-test; b Independent t-test; c Cases=31, Controls=96; d Cases=44, Controls=102; NA=Not Analyzed
The OR values of the children involvement in agricultural activities showed that this was the risk factor for stunting (OR=2.02 and 95% CI=1.97-4.23). Bivariate logistic regression results showed that children with high pesticide exposure had a risk of more than three times for stunting compared to the unexposed children (OR=3.25 and 95% CI=1.09-9.66), while for moderate exposure, the OR was 1.58 (95% CI=0.58-4.33) and low exposure was 1.17 (95%
CI=0.43-3.19) (Table 3).
Table 3. Association between history of pesticide exposure and stunting
Variable Cases
n=48
Controls n=112
OR (95% CI) Mothers involvement in
agricultural activity during pregnancy:
Yes 26 (54.2) 50 (44.6) 1.47 (0.74-2.89)
No 22 (45.8) 62 (55.4)
Subjects at the time of infant/
toddler brought the mother to farm/stall:
Yes 19 (39.6) 29 (25.9) 1.88 (0.92-3.84)
No 29 (60.4) 83 (74.1)
Involvement of subjects in agricultural activities at school age:
Yes 35 (72.9) 64 (57.1) 2.02 (1.97-4.23)
No 13 (27.1) 48 (42.9)
History of pesticide exposure (composite variable) b:
‘High’ 13 (27.1) 14 (12.5) 3.25 (1.09-9.66)
‘Moderate’ 14 (29.2) 31 (27.7) 1.58 (0.58-4.33)
‘Low’ 13 (27.1) 39 (34.8) 1.17 (0.43-3.19)
‘Unexposed’ (ref) 8 (16.6) 28 (25.0) -
*(ref) reference category
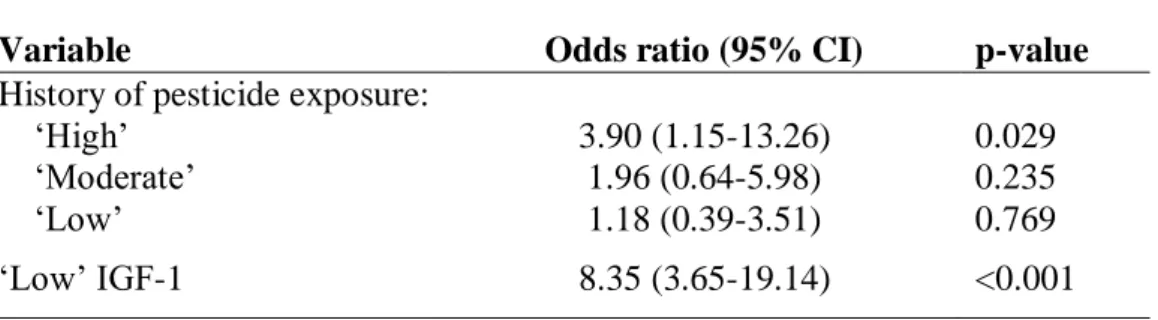
13 The results of binary logistic regression using backward method, showed that there were association between the ‘high’ pesticide exposure (p=0.029) and ‘low’ IGF-1 level (p<0.001) and stunting in children and both were proven to be risk factors for stunting with adj-OR=3.90 and 8.35 respectively (Table 4).
Table 4. Binary logistic regression analysis of stunting risk factors
Variable Odds ratio (95% CI) p-value
History of pesticide exposure:
‘High’ 3.90 (1.15-13.26) 0.029
‘Moderate’ 1.96 (0.64-5.98) 0.235
‘Low’ 1.18 (0.39-3.51) 0.769
‘Low’ IGF-1 8.35 (3.65-19.14) <0.001
Discussion
Stunting is a condition of linear growth disorder32 and has been more often associated with poor nutritional intake.33 Less intake of macronutrients, especially energy and protein, were the cause of growth disorders in children.34 Amino acids present in the body as well as those derived from food, are essential ingredients in the formation of proteins as well as collagen. Food sources of energy (amino acids, carbohydrates, fats) support the growth process directly or indirectly through the provision of fuel for neutrophils, macrophages, lymphocytes, and other cells that function in cell or tissue regeneration.35 The role of nutrition in linear growth occurs through various mechanisms. Experiments with animals showed that the restriction of energy and protein in the diet lowered the plasma concentration of Insulin-like Growth Factor- 1 (IGF-1), a hormone that is needed in the process of linear growth36 and will return to normal after energy and protein refeeding. The effect of intake restriction on IGF-1 levels, was more visible on protein restriction than on energy restriction. IGF-1 levels also decreased in patients
14 with kwashiorkor (acute protein deficiency) and in children with protein-energy malnutrition (PEM).35
In addition to macronutrients, several micronutrients are also essential for growth, namely Zinc (Zn),37 iron (Fe) and vitamin A.34 Zn deficiency in rats decreased IGF-1 and growth hormone (GH) plasma concentrations.38 Zn was associated to bone metabolism,39 played a role in the synthesis of deoxyribonucleic acid (DNA) and ribonucleic acid (RNA), and also interacts with important hormones involved in bone growth such as somatomedin-c, osteocalcin, testosterone, thyroid hormones, and insulin.40 Other micronutrient deficiencies, such as iron (Fe) and magnesium (Mg), can cause anorexia, and result in impaired growth indirectly, due to reduced dietary intake including energy and protein. Zinc, iron, and selenium are also associated with immune function and disease risk, which can interfere with growth.41 Based on interviews with the FFQ method, the mean of energy and protein intake in case group was higher than control groups. This result was probably related to the recall bias in the interview process. To anticipate this, serum albumin levels were examined to describe protein intake more objectively,42 and the results showed no difference in mean albumin levels between cases and controls (Table 2).
Some theories can be used to explain why the energy and protein adequacy levels in the case group are higher than the control group, among others, the occurrence of nutrient absorption disorders caused by pathogenic bacterial infections and mycotoxins43 or due to exposure to toxic substances in the environment,44 referred to as environmental enteric dysfunction (EED). EED is a sub-clinical disorder characterized by morphological and physiological abnormalities in the small intestine, in the form of increased permeability, impaired nutritional absorption and growth faltering.45,46 Pesticides are one of the toxic substances in the environment that can trigger the onset of EED. Exposure to pesticides through breast milk, food, and drinking water is thought to be a major cause of EED in children.47 High
15 intake of nutrients, energy and protein, will not provide enough benefits for growth and development, if EED occurs. Several studies have linked the high prevalence of stunting with EED.47,48 Research in Zimbabwe proves that the presence of gastrointestinal inflammatory biomarkers is associated with stunting in infants.49 The exact diagnosis for EED is not easy, as it requires an invasive gastrointestinal tissue biopsy.45
Exposure to toxic substances in the environment, including pesticides, leads to oxidative stress50 which led to an increase in the use of energy for the activation of the immune system, thereby reducing the use of energy for the maintenance, reproduction, growth and thermoregulation.51 The term for this wasteful use of energy is known as the 'Barrel Model'.52 Research on juvenile Japanese quails proved that exposure to the subchronic exposure to chlorpyrifos, one of the most widely used pesticides in agricultural areas, disrupting energy expenditure and the ability to detoxify.53
The proportion of anemia incidence between case and control groups were relatively equal (Table 2). This condition was due to no differences between both groups in levels of nutrient intakes like iron and protein (serum albumin) as essential elements for hemoglobin synthesis (Table 2).
Based on the causes, stunting can be divided into two categories, namely growth hormone deficiency and idiopathic.3,54 Children borned and raised in agricultural areas have the potential to be exposed to pesticides since they were in the womb, making them at risk for various health problems including growth disorder. Growth disorders caused by the exposure of pesticides can work through several mechanisms, such as the disruption of the hormone system that plays a role in the growth process. Several types of pesticides, including organophosphates and carbamates that are widely used in agricultural activities, are classified as EDCs, chemicals in the environment that can interfere with synthesis, secretion, transport, metabolism, binding action, and elimination of hormones in the body that keep homeostasis,
16 reproduction, and the process of growth and development.21 Thyroid hormone and IGF-1 are the hormones that are necessary for the process of children growth. Several studies had shown that exposure to pesticides was the risk factor for hypothyroidism.12,55–57 Thyroid hormone deficiency (hypothyroidism) will cause metabolic disorders in the cells so that the process of growth and development are also disrupted.58 The thyroid dysfunction caused by pesticides exposure was work through some mechanisms, which disrupts the TSH receptor on the thyroid gland,59 the similarity of the pesticide chemical structure with thyroid hormone,59 lowering the D1 (deiodinase type 1) enzyme,60 and stimulate the D3 enzyme.59 Exposure to pesticides, especially organochlorines groups, can also disrupt the IGF-1 function.13,14 Research in Spain has shown that the mean IGF-1 levels in the women who had DDT metabolites detected were lower than those who were not detected.13 Binary logistic regression analysis showed that the children with low levels of IGF-1 had 8.35 times higher risk for stunting compared to the normal IGF-1 levels. IGF-1 hormones play a role in growth through its role as a mitogen and cell proliferation stimulator and play an important role in tissue repair/regeneration.61 IGF-1 also mediates protein anabolic processes and increases growth hormone (GH) activity for linear growth 36,62. Some other chemicals such as lead [plumbum (Pb)],54,63 phthalate64 have been shown to disrupt the function of the IGF-1 hormone. Lead is a toxic substance that is widely available in the environment, among others in paint, toys, cookware, battery, electronic equipment, and others. Lead exposure in children can occur through several paths, i.e. oral (contaminated food/drink) and inhalation,65 phthalate is a chemical contained in plastic raw materials in toys and building materials, such as wall paint, which also potentially exposed to the children in their daily activities.66 Other chemicals, dioxins and polychlorinated biphenyls (PCBs) have also been shown to interfere child growth.66
In this study, we could not eliminate unmeasured confounders, especially another EDCs exposure, (i.e. phthalate, dioxins and PCBs exposures), but we did examine the potential for
17 confounding among known predictors of stunting in our data analyses namely levels of TSH, IGF-1, Zn, hemoglobin, and nutrient intake. The results of measurements for these potentially confounding variables except IGF-1 level were homogenous between both groups.
Notwithstanding, the level of nutrient intake in the case group was better than that of in the control group. These results indicated the possibility of any contribution of environmental toxicants on children's growth disorders. The other limitation in our study was in terms of data collection for pesticide exposures that only used an interview method. It could be information bias. The questions of activities on the farm written in a questionnaire were our research participants’ routine activities. Therefore, the information bias that might occur could be minimized. For further studies, measurement of pesticide metabolites in the urine needs to be undertaken to ensure the pesticide exposures.
Our results demonstrated an association between pesticide exposure and stunting among children in agricultural areas. Pesticide exposure could be a risk factor for the occurrence of stunting. Further research needs to measure several variables that have potential as confounders, such as lead, phthalate, dioxins and PCBs exposures. These results provide strong support for taking action in the prevention or reduction of pesticide exposure among pregnant women and children,e.g. by reducing or limiting their involvements in agricultural activities.
Conflict of interest
The authors declare that they have no conflict of interest.
Acknowledgement
The authors are grateful to the Directorate of Research and Community Services, Directorate General of Research and Development, Ministry of Research, Technology, and Higher Education of the Republic of Indonesia for providing funding of doctoral research. We also would like to thank the principals and teachers in fours Elementary Schools in Brebes District, Indonesia for their support to this study; and we are grateful for the support of all subjects.
18 References
1. Gibson R. Principles of Nutritional Assessment. 2nd ed. New York: Oxford University Press, Inc; 2005. http://www.oup.com.
2. Mikhail W, Sobhy H, El-sayed H, Khairy S, Salem H, Samy M. Effect of Nutritional Status on Growth Pattern of Stunted Preschool Children in Egypt National Nutrition Institute ( NNI ), Cairo , Egypt. Acad J Nutr. 2013;2(1):1-9.
doi:10.5829/idosi.ajn.2013.2.1.7466
3. Nicol L, Allen D, Czernichow P, Zeitler P. Normal growth and growth disorders. In:
Kappy M, Allen D, Geffner M, eds. Pediatric Practice Endocrinology. New York: The McGraw-Hill Companies, Inc; 2010:23-79.
4. Candra A, Puruhita N, Susanto J. Risk factors of stunting among 1-2 years old children in Semarang City. Media Med Indones. 2011;45(3):206-212.
5. Paudel R, Pradhan B, Rr W, Dp P, Sr O. Risk Factors for Stunting Among Children : A Community Based Case Control Study in Nepal. Kathmandu Univ Med J.
2012;39(3):18-24.
6. Vogiatzi M, Copeland K. The Short Child. Pediatr Rev. 1998;19(3):92-99.
doi:10.1542/pir.19-3-92
7. Kar B, Rao S, Chandramouli B. Cognitive development in children with chronic protein energy malnutrition. Behav Brain Funct. 2008;4(1):31. doi:10.1186/1744-9081- 4-31
8. Sokolovic N, Selvam S, Srinivasan K, Thankachan P, Kurpad A V, Thomas T. Catch- up growth does not associate with cognitive development in Indian school-age
children. Eur J Clin Nutr. 2014;68(1):14-18. doi:10.1038/ejcn.2013.208
9. Brito G, Onis M de. Growth status and academic performance in Brazilian school age children: growth retardation impairs mathematical, but not reading and spelling abilities TT - Crescimento e desempenho acadêmico em escolares brasileiros: retardo no crescimento interfere co. Arq Neuropsiquiatr. 2006;64(4):921-925.
10. Prendergast A, Humphrey J. The stunting syndrome in developing countries. Paediatr Int Child Health. 2014;34(4):250-265. doi:10.1179/2046905514Y.0000000158
11. Indonesian Health Ministry. National Survey on Primary Health. Report. 2013.
12. Suhartono, Djokomoeljanto R, Hadisaputro S, Subagio H, Kartini A, Suratman.
Pesticides exposure and risk factor of hypothyroidism in women childbearing in the agricultural area, Indonesia (in Bahasa). Media Med Indones. 2012;46(2):91-99.
13. Boada L, Lara P, Alvarez-León E, et al. Serum levels of insulin-like growth factor-I in relation to organochlorine pesticides exposure. Growth Horm IGF Res.
2007;17(6):506-511. doi:10.1016/j.ghir.2007.05.004
14. Zumbado M, Luzardo O, Lara P, et al. Insulin-like growth factor-I (IGF-I) serum concentrations in healthy children and adolescents: Relationship to level of
contamination by DDT-derivative pesticides. Growth Horm IGF Res. 2010;20(1):63- 67. doi:10.1016/j.ghir.2009.07.003
15. Idohou-Dossou N, Wade S, Guiro A, et al. Nutritional status of preschool Senegalese children: long-term effects of early severe malnutrition. Br J Nutr. 2003;90(06):1123.
doi:10.1079/BJN2003990
16. Rauh V, Garfinkel R, Perera F, et al. Impact of Prenatal Chlorpyrifos Exposure on Neurodevelopment in the First 3 Years of Life Among Inner-City Children. Pediatrics.
2006;118(6):e1845-e1859. doi:10.1542/peds.2006-0338
17. Bouchard M, Bellinger D, Wright R, Weisskopf M. Attention-deficit/hyperactivity disorder and urinary metabolites of organophosphate pesticides. Pediatrics.
2010;125(6):e1270-e1277. doi:10.1542/peds.2009-3058
19 18. Budiyono, Suhartono, Kartini A, et al. Pesticide Metabolites, Anti-Thyroid Peroxidase
and Thyroid Stimulating Hormone Status in School Children: A Preliminary Study in Agriculture Areas in Indonesia. Int J Sci Basic Appl Res. 2015;22(1):1-12.
19. Suhartono, Kartini A, Subagio H, et al. Pesticide Exposure and Thyroid Function in Elementary School Children Living in an Agricultural Area, Brebes District, Indonesia.
Int J Occup Environ Med. 2018;9(3):137-144. doi:10.15171/ijoem.2018.1207 20. Kartini A, Suhartono, Pangestuti D, Adi M, Suratman, Rasipin. Goiter and
hypothyroidism among elementary school children in lowland agricultural area, Brebes District Indonesia. Indian J Public Heal Res Dev. 2018;9(9):120-125.
21. Diamanti-Kandarakis E, Bourguignon J, Giudice L, et al. Endocrine-Disrupting Chemicals: An Endocrine Society Scientific Statement. Endocr Rev. 2009;30(4):293- 342. doi:10.1210/er.2009-0002
22. Stone MB and Wallace RB. Medicare Coverage of Routine Screening for Thyroid Dysfunction. Washington DC: The National Academic Press; 2003.
http://www.nap.edu/catalog/10682.html.
23. Lemeshow S, Hosmer Jr D, Klar J, Lwanga S. Adequacy of Sample Size in Health Studies. New York: John Wiley & Sons Ltd.; 1993.
24. World Health Organization. WHO Child Growth Standards. Geneva: WHO Press;
2006.
25. Schlesselman J, Stolley P. Case-Control Studies. Design, Conduct, Analysis. New York: Oxford University Press; 1982.
26. Youden W. Index for rating diagnostic tests. Cancer. 1950;3(1):32-35.
27. Habibzadeh F, Habibzadeh P, Yadollahie M. On determining the most appropriate test cut-off value: the case of tests with continuous results. Biochem Medica.
2016;26(3):297-307.
28. World Health Organization. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. 2011:1-6.
http://www.who.int/vmnis/indicators/haemoglobin/en/.
29. Dehghani S, Katibeh P, Haghighat M, Moravej H, Asadi S. Prevalence of Zinc Deficiency in 3-18 Years Old Children in Shiraz-Iran. Iran Red Crescent Med J.
2011;13(1):4-8.
30. Abdullah S, Ahmed F, Lutfi M. Serum Albumin Level in Sudanese Children with Edematous and Non-Edematous Malnutrition * 1. Asian J Biomed Pharm Sci.
2014;04(38):47-49. doi:10.15272/ajbps.v4i38.636
31. Yasmin G, Kustiyah L, Dwiriani C. Risk factors of stunting among school-aged children from eight provinces in Indonesia. Pakistan J Nutr. 2014;13(10):557-566.
32. World Health Organization. Catalogue of health indicators. 1996:37-38.
33. de Onis M, Branca F. Childhood stunting : a global perspective. Matern Child Nutr.
2016;12:12-26. doi:10.1111/mcn.12231
34. Umeta M, West C, Verhoef H, Haidar J, Hautvast J. Factors Associated with Stunting in Infants Aged 5 – 11 Months in the Dodota-Sire District , Rural Ethiopia. J Nutr.
2003;133:1064-1069.
35. Esfivariz C, Ziegler T. Nutrition and the Insulin-Like Growth Factor System.
Endocrine. 1997;7(1):65-71.
36. Skottner A. Biosynthesis of Growth Hormone and Insulin-Like Growth Factor-I and the Regulation of their Secretion. Open Endocrinol J. 2012;6(Suppl 1: M2):3-12.
37. Gibson R, Manger M, Krittaphol W, et al. Does zinc deficiency play a role in stunting among primary school children in NE Thailand ? Br J Nutr. 2017;(May):167-175.
doi:10.1017/S0007114507250445
38. Ninh N, Thissen J, Maiter D, Adam E, Mulumba N, Ketelslegers J. Reduced liver
20 insulin-like growth factor-I gene expression in young zinc-deprived rats is associated with a decrease in liver growth hormone (GH) receptors and serum GH-binding protein. J Endocrinol. 1995;144(3):449-456. doi:10.1677/joe.0.1440449
39. Yamaguchi M. Role of zinc in bone metabolism and preventive effect on bone disorder. Biomed Res Trace Elem. 2007;18(4):346-366.
40. Salgueiro M, Zubillaga M, Lysionek A, Caro R, Weill R, Boccio J. The Role of Zinc in the Growth and Development of Children. Nutrition. 2002;18:510-519.
41. Rivera M, De Souza A, Araujo-Jorge T, De Castro S, Vanderpas J. Trace elements, innate immune response and parsites.pdf. Clin Chem Lab Med. 2003;41(8):1020-1025.
42. Watanabe M, Higashiyama A, Kokubo Y, Ono Y, Okayama A, Okamura T. Protein Intakes and Serum Albumin Levels in a Japanese General Population : NIPPON DATA90. J Epidemiol. 2010;20(Suppl 3):5-7. doi:10.2188/jea.JE20090221
43. Crane R, Jones K, Berkley J. Environmental enteric dysfunction : An overview. Food Nutr Bull. 2015;36(1):S76-S87.
44. Miller G, Jones D. The Nature of Nurture : Refining the Definition of the Exposome.
Toxicol Sci. 2014;137(1):1-2. doi:10.1093/toxsci/kft251
45. Lin A, Arnold B, Afreen S, et al. Household Environmental Conditions Are Associated with Enteropathy and Impaired Growth in Rural Bangladesh. Am J Trop Med Hyg.
2013;89(1):130-137. doi:10.4269/ajtmh.12-0629
46. Prendergast A, Kelly P. Review : Enteropathies in the Developing World : Neglected Effects on Global Health. Am J Trop Med Hyg. 2012;86(5):756-763.
doi:10.4269/ajtmh.2012.11-0743
47. Mapesa J, Maxwell A, Ryan E. An Exposome Perspective on Environmental Enteric Dysfunction. Environ Health Perspect. 2016;124(8):1121-1126.
48. Owino V, Ahmed T, Freemark M, Kelly P. Environmental Enteric Dysfunction and Growth Failure / Stunting in Global Child Health. Pediatrics. 2016;138(6):1-10.
doi:10.1542/peds.2016-0641
49. Prendergast AJ, Rukobo S, Chasekwa B, et al. Stunting is characterized by chronic inflammation in Zimbabwean infants. PLoS One. 2014;9(2):e86928.
doi:10.1371/journal.pone.0086928
50. Lukaszewicz-hussain A. Role of oxidative stress in organophosphate insecticide toxicity – Short review. Pestic Biochem Physiol. 2010;98:145-150.
doi:10.1016/j.pestbp.2010.07.006
51. Degen A. Effect of macroparasites on the energy budget of small mammals. In:
Morand S, Krasnov Y, Poulin R, eds. In: Morand S, Krasnov Y, Poulin R, eds.
Micromammals and Macroparasites: From Evolutionary Ecology to Management.
Tokyo: Springer-Verlag; 2006:371-400.
52. Weiner J. Physiological limits to Energy Budgets Sustainable in Birds and Mammals : Ecological Implications. Trends Ecol Evol. 1992;7(11):384-388.
53. Narváez C, Manuel J, Píriz G, Sanchez-hernandez J, Sabat P. Chemosphere Subchronic exposure to chlorpyrifos affects energy expenditure and detoxification capacity in juvenile Japanese quails. Chemosphere. 2016;144:775-784.
doi:10.1016/j.chemosphere.2015.09.060
54. Xu Y, Liu M, Wang P, et al. Correlation between serum IGF-1 and blood lead level in short stature children and adolescent with growth hormone deficiency. Int J Clin Exp Med. 2014;7(4):856-864.
55. Goldner W, Sandler D, Yu F, Hoppin J, Kamel F, Levan T. Pesticide use and thyroid disease among women in the agricultural health study. Am J Epidemiol.
2010;171(4):455-464. doi:10.1093/aje/kwp404
56. Farokhi F, Taravati A. International journal of Medical Investigation Pesticide
21 exposure and thyroid function in adult male sprayers. Int J Med Invest num.
2014;3(4):127-132.
57. Piccoli C, Cremonese C, Koifman R, Koifman S, Freire C. Pesticide exposure and thyroid function in an agricultural population in Brazil. Environ Res. 2016;151:389- 398. doi:10.1016/j.envres.2016.08.011
58. Setian N. Hypothyroidism in children: diagnosis and treatment. J Pediatr (Rio J).
2007;0(0):209-216. doi:10.2223/JPED.1716
59. Boas M, Feldt-Rasmussen U, Skakkebæk N, Main K. Environmental chemicals and thyroid function. Eur J Endocrinol. 2006;154(5):599-611. doi:10.1530/eje.1.02128 60. Wade M, Parent S, Finnson K, et al. Thyroid toxicity due to subchronic exposure to a
complex mixture of 16 organochlorines, lead, and cadmium. Toxicol Sci.
2002;67(2):207-218. doi:10.1093/toxsci/67.2.207
61. Guntur A, Rosen C. IGF-1 regulation of key signaling pathways in bone. Bonekey Rep.
2013;2(September):1-6. doi:10.1038/bonekey.2013.171
62. Laron Z. Insulin-like growth factor 1 (IGF-1): a growth hormone. J Clin Pathol Mol Pathol. 2001;54(5):311-316. doi:10.1136/mp.54.5.311
63. Fleisch A, Burns J, Williams P, et al. Blood lead levels and serum insulin-like growth factor 1 concentrations in peripubertal boys. Environ Health Perspect.
2013;121(7):854-858. doi:10.1289/ehp.1206105
64. Boas M, Frederiksen H, Feldt-Rasmussen, UlSkakkebæk N, et al. Childhood exposure to phthalates: Associations with thyroid function, insulin-like growth factor I, and growth. Environ Health Perspect. 2010;118(10):1458-1464. doi:10.1289/ehp.0901331 65. Liu J, Goyer R, Waalkes P. Toxic effects of metals. In: Shanahan J, Naglieri C, eds.
Casarett and Doull’s Toxicology: The Basic Science of Poisons. 7th ed. New York:
The McGraw-Hill Companies, Inc; 2008:931-979.
66. Ejaredar M, Nyanza E, Eycke K, Dewey D. Phthalate exposure and childrens neurodevelopment: A systematic review. Environ Res. 2015;142:51-60.
doi:10.1016/j.envres.2015.06.014
Take-Home Message
Stunting prevalence among school-aged children in Indonesia was high
The prevalence of stunting in school-aged children in Brebes District is the highest among the other districts in Central Java, Indonesia
The use of pesticides in Indonesian agricultural areas is very high
Pesticides are one of the toxic substances in the environment
Toxic substances exposure from the environment might also interfere the synthesis of Insulin-like Growth Hormone 1 (IGF-1).
Pesticide exposure was associated with stunting among children in agricultural areas.
[IJOEM] Decision Letter Ms #1428
Dari: Dr. Farrokh Habibzadeh ([email protected]) Kepada: [email protected]
Tanggal: Rabu, 2 Januari 2019 12.16 WIB
Ms Title: "Exposure of pesticide as the risk factors for stunting on school-aged children in Indonesian agricultural areas"
Ms #1428
Dear Dr. Suhartono Suhartono,
We reviewed the revised version of your manuscript. I am pleased to inform you that the manuscript has been accepted for publication in The IJOEM.
We'll edit your manuscript according to our house style and send you the galley proof of the article. In due course, you may be asked some editorial questions. Thank you very much for your contribution to the Journal.
Best Regards, F. Habibzadeh, MD, Editor, The IJOEM
Yahoo Mail - [IJOEM] Decision Letter Ms #1428 https://mail.yahoo.com/d/search/keyword=ijoem/messages/7387?guce_re...
1 of 1 21/04/2021, 7:54
4. Accepted
Follow us on Twitter
@TheIJOEM
CURRENT ISSUE
USER Username Password
Remember me Login
JOURNAL CONTENT Search
Search Scope All Search Browse
By Issue By Author By Title FONT SIZE HOME ABOUT LOGIN SEARCH CURRENT ARCHIVES ONLINE FIRST
Home > Vol 10, No 1 January (2019) > Kartini
Pesticide Exposure and Stunting among Children in Agricultural Areas
Apoina Kartini, Hertanto W Subagio, Suharyo Hadisaputro, Martha I Kartasurya, Suhartono Suhartono, Budiyono Budiyono
Abstract
Background: The prevalence of growth disorders among school-aged children in Indonesia is high (30.7%). Pesticides have been massively used in Indonesian agricultural areas.
Objective: To determine if exposure to pesticides is associated with stunting among children in agricultural areas.
Methods: This case-control study included 160 children (48 cases and 112 controls) aged 8–12 years. Exposure to pesticides was measured based on the history of the exposure since perinatal period, infancy, and childhood of the participants. Stunting was determined as a height for age z-score (HAZ) < ‑2 SD. Other variables measured were levels of thyroid stimulating hormone (TSH), insulin-like growth factor-1 (IGF-1), hemoglobin, zinc, albumin, nutrient adequacy level (energy and protein), and history of infection, low-birth weight (LBW), and mother's height.
Results: There were no significant difference between the cases and controls in terms of in the baseline characteristics, except for the median IGF-1 level; it was significantly (p<0.001) lower in the cases (66.73 ng/mL) than the controls (112.57 ng/mL). High level of pesticide exposure (p=0.029) and low IGF-1 levels (p<0.001) were significantly associated with stunting. After adjusting for confounding variables, these variables were found to be independent risk factors for stunting in children (aOR 3.90, 95% CI 1.15 to 13.26; and aOR 8.35, 95% CI 3.65 to 19.14, respectively).
Conclusion: Pesticide exposure could be a risk factor for the occurrence of growth disorders in children living in agricultural areas. Necessary actions should be taken to protect children living in agricultural areas from exposure to pesticides.
Keywords
Pesticides; Growth disorders; Child; Agriculture
Full Text:
FULL TEXT (HTML)PDF [885 KB]EPUB doi: 10.15171/ijoem.2019.1428
pISSN: 2008-6520 eISSN: 2008-6814
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License
Citations
CrossRef - Citation Indexes: 3 Scopus - Citation Indexes: 9
Usage
EBSCO - Abstract Views: 117 EBSCO - Full Text Views: 78 EBSCO - Link-outs: 24
Captures
EBSCO - Exports-Saves: 12 Mendeley - Readers: 94
Social Media Twitter - Tweets: 2
- see details