She completed her doctorate in the field of seniors and home care services. Older people will account for 87 percent of total population growth between 2005 and 2051 (Statistics New Zealand, 2006). This model uses "case finding" to target only at-risk older adults through systematic population screening using the BRIGHT screen.
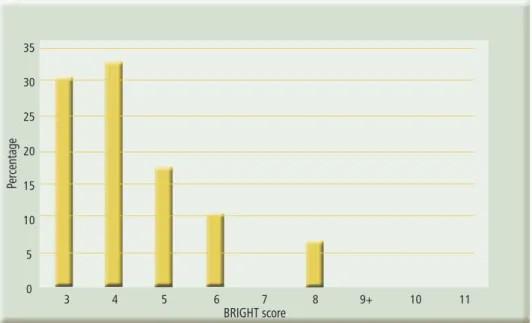
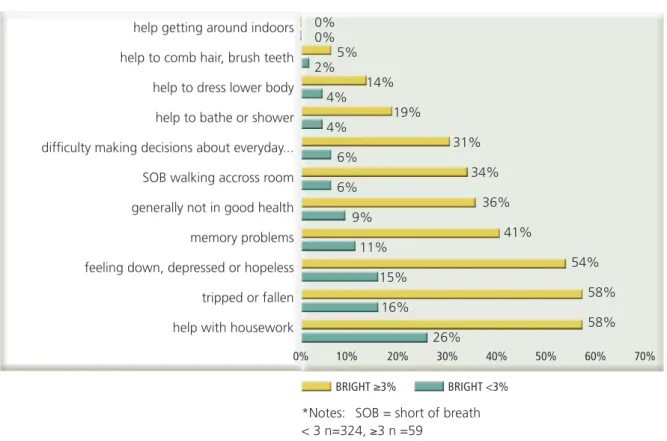
To describe a GNS-guided proactive risk screening process, using the Brief Risk Identification for Geriatric Health Tool (BRIGHT) screen, for older people in the community. To describe the impact of a comprehensive gerontology assessment and care planning intervention for older people identified as high risk in the community. For all older people who completed BRIGHT screens, 15% scored ≥3 and the mean positive BRIGHT screen score was 4.
INTRODUCTION
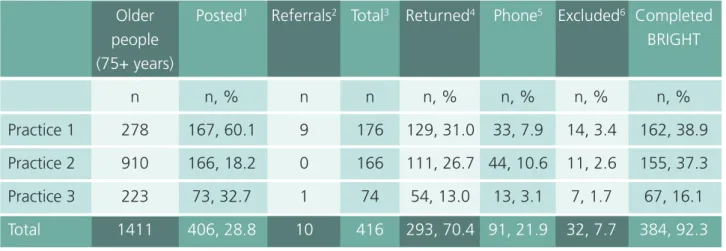
As a result, older people with increased disability are living longer in society than ever before (Broad et al., 2011). Older people were recruited from three primary care practices within Waitemata PHO (formerly Harbor Health PHO), Auckland. All patients aged 75 and over in all three practices were identified and an average of 50 older people per month were sent the screening tool along with a description of the pilot.
In addition, nine older people were assessed with the interRAI MDS-HC comprehensive geriatric assessment used internationally (Landi et al., 2000), including in New Zealand in the community of all DHBs. The BASDEC has been validated as a suitable instrument for screening depression in the elderly. Qualitative evaluation: Qualitative interviews were conducted to assess the effectiveness of the GNS role from the perspectives of older people and health professionals.
RESULTS
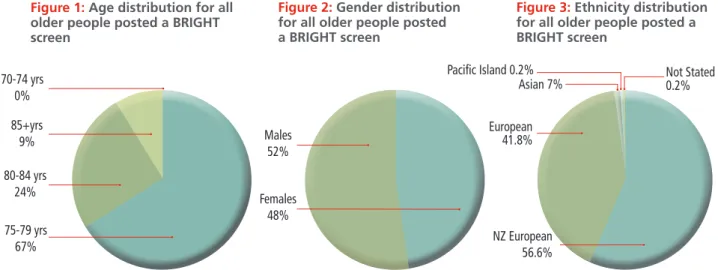
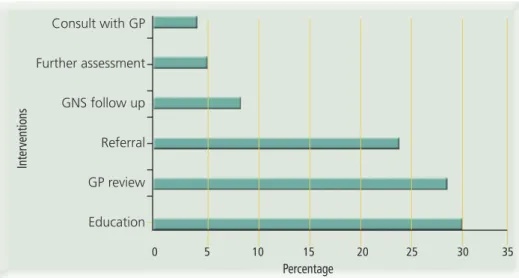
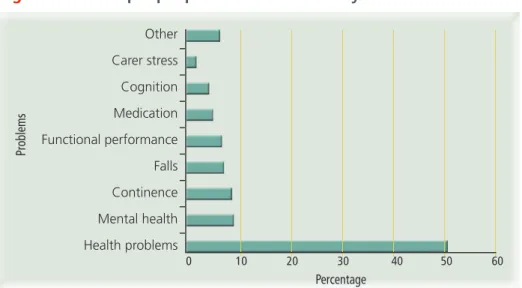
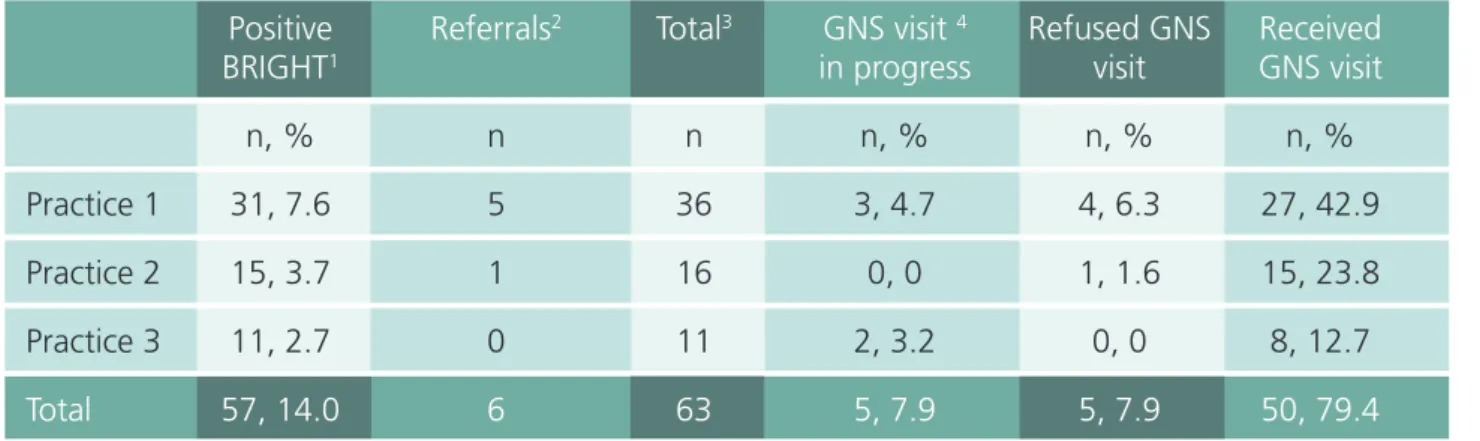
4 GNS had not carried out the visit and comprehensive assessment for these older people. Percentages calculated from the total number of positive BRIGHT screens and referrals. Figures 1, 2 and 3 show baseline characteristics of the total number of older people who were sent BRIGHT screens as well as direct referrals (n=416). In terms of ethnicity, 2 older people were from the Middle East, 1 was a Pacific Islander and 1 did not state his ethnicity.
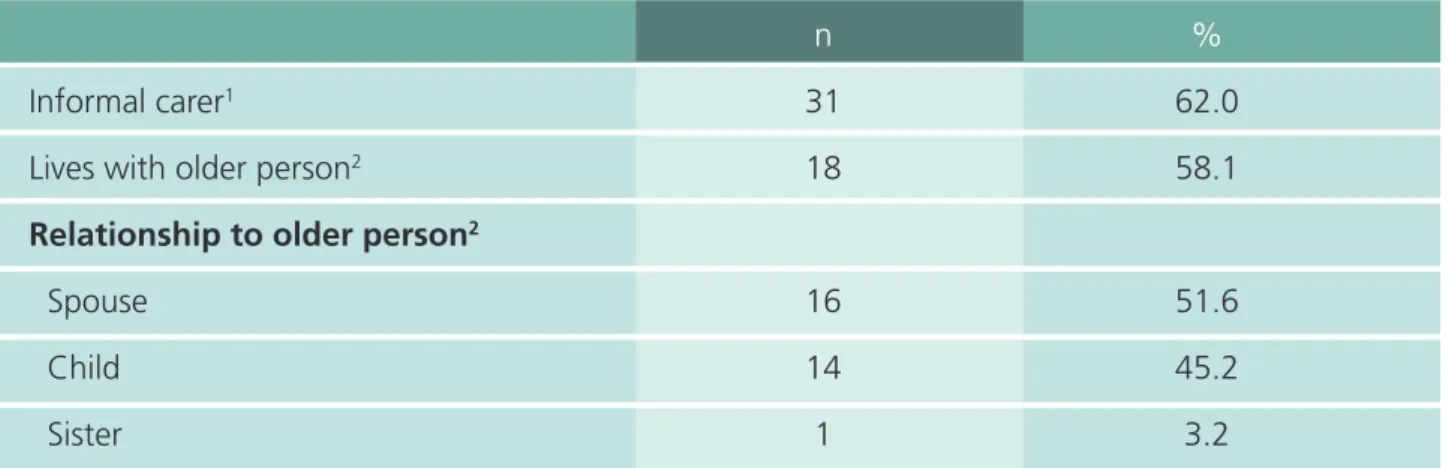
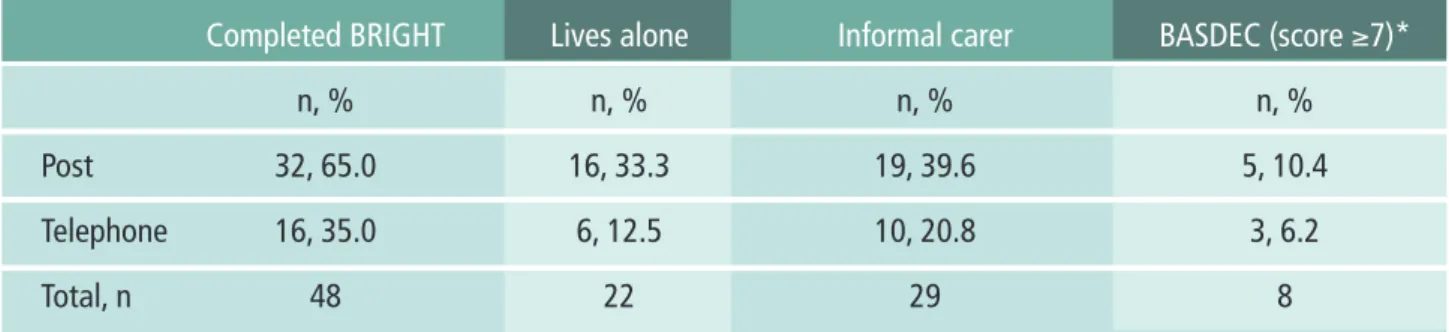
Figures 4, 5 and 6 present the basic demographics for older people who received a GNS visit because of a positive BRIGHT screen or GP referral (n=50), revealing that the majority were European NZ (68%), female (56%) and age 75-79 years. 1Percentage calculated based on the total number of older people who received a GNS visit due to a positive BRIGHT screen or GP referral (n=50). Percentages calculated based on total BRIGHT screens completed by all older adults (n=383) Excluded due to meeting exclusion criteria, deceased or moved to residential aged care: n= 19.
Older people referred by GP and scored <3 on the BRIGHT screen n=3 Missing data n=2 (referred by GP and did not complete a BRIGHT screen). 48 people received a GNS visit (another two, referred by their GPs) received a home visit but not a LYS screen. Percentages calculated from the total number of elderly who received a GNS visit and completed the BRIGHT screen (n=48).
The following tables and figures show the findings regarding older people who received GNS scores (n=50). A total of 70% of the elderly received one GNS control visit (three elderly received an additional control visit), and 78% of them were discharged from the GNS. A small number of older people (n = 3.6%) died or entered care after the initial GNS assessment.
Percentages calculated from the total number of elderly who received a GNS visit (n=50) SD= standard deviation.
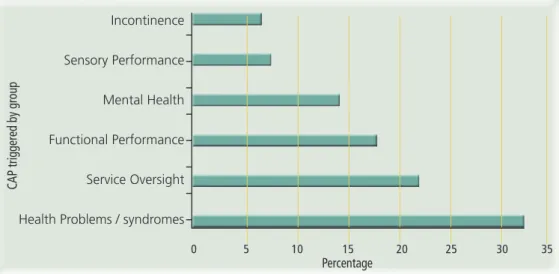
MDS-HC – CAPS
The elderly made several positive comments regarding the competent practice and personal qualities of GNS. Qualitative interviews were conducted to assess the effectiveness of the GNS role from the perspective of the elderly and health professionals. One of the benefits mentioned by both the GPs and the practical nurse was how the GNS role saved them time.
The GNS was found to be an important link between healthcare professionals, the elderly and their families. Most healthcare professionals commented on the benefit gained from GNS assessment of people in their own home. GNS made a number of comments regarding the benefits of home counseling.
This allowed time for rapport to build, which resulted in the older person disclosing more to GNS. The GNS was valid for the primary care setting as shown in a number of ways. The GNS identified older people who were not coping well and was able to implement appropriate interventions.
Therefore, GNS will also need to undertake parts of the original WDHB GNS physical assessment. These comments related to the practical help, environmental changes and emotional effect as a result of the GNS contribution. A number of health professionals referred to the practical assistance that the GNS offered to the elderly.
GNS offered several examples of the positive physical and psychological impact she gave the elderly. GNS described many specific examples of the practical advice she gave to older people. Older people reported no problems in relation to the GNS role and few health professionals made comments.
DISCUSSION
- The BRIGHT tool was an efficient mechanism of ruling out those that did not required a full comprehensive geriatric assessment. The proactive population approach taken was
- The PHO GNS was seen as help and facilitated comprehensive care for high needs older people
- The importance of Integration of GNS into Primary Health Care Practices and DHB GNS team within the Integrated Health Model
- Implementation of the InterRAI MDS-HC in Primary Care was difficult
- Falls in Older Adults need a specific intervention in Primary Care: When older people fall the cause is often multi-factorial and can indicate that there are several acute and chronic
- Mild and Moderate Depression and Dysthymia need available interventions in Primary Care: Those that scored three or greater on the BRIGHT screen were found to have a higher
The PHO GNS intervention can potentially identify isolated elderly and refer them to appropriate resources (Frederick et al., 2007). Following the pilot, most GPs expressed enthusiasm for the PHO GNS role and a strong desire to work with a GNS in the future. They said that the PHO GNS improved the care of their high-needs patients.
Qualitative feedback from the health care team and older adults who received the PHO GNS intervention indicated that the use of the BRIGHT screen and follow-up PHO GNS home visits were an effective way to provide targeted early intervention. The PHO GNS model in this pilot included features that have been shown to be successful in advance care coordination programs or studies. In this pilot project, GPs reported that PHO GNS provided more resources and time to care for older people with high needs.
This pilot is designed to provide peer support and mentoring from the WDHB GNS team to PHO GNS. This pilot demonstrated a possible way to use specialist training and skills in primary care, with ongoing PHO GNS training and support. PHO GNS was seen as helpful and facilitated comprehensive care for seniors with high needs.
GPs and practice nurses appreciated the expertise and extra time that the PHO GNS could devote to the care of older people with complex needs. The PHO GNS role, working with a group of general practitioners, has successfully built gerontology nurse specialist capacity within primary care, so that assessment and intervention can be undertaken in high-risk older people in the community. The assessment itself appeared to be a general assessment and lacked the depth of specialist gerontology assessment required by the PHO GNS.
Third, the interRAI MDS-HC may not be suitable for use by PHO GNS because it is a generalist assessment and not a specialist assessment.
RECOMMENDATIONS
- Continue the Gerontology in Primary Care Model into Phase II
- Expand the scope of the Model to include hospital discharge planning and dementia care
- Develop a Pathway for the treatment of Depression in Primary Care
- Extending the GNS follow up and building Gerontology Capacity in the Primary Care workforce
- Develop the interRAI MDS-HC
Depression is a possible clinical indicator of dementia, including a risk factor for the accelerated deterioration of Alzheimer's disease. Early treatment of depression in older adults in primary care could impact dementia treatment and delay functioning in older adults, with potential economic savings. Brooten and Naylor (2002) found that there is a dose effect with the intensity of a nursing intervention.
Enhanced follow-up should be developed, with efficient transfer of care to the general practitioner and primary health care nurse. The transfer process can be an ideal mechanism for PHO GNS to upgrade and train general nursing staff in geriatric care, thereby building the capacity needed for the future workforce. For the tool to be useful in primary care, it needs to interface with GP PMS systems and hospital database IT systems.
In addition, the outcome reports should be in a clinically useful report that is understandable to those unfamiliar with the interRAI system. Further development should also be undertaken to integrate the generalist assessment content of the interRAI MDS-HC and the specialist GNS assessment content. Waitemata PHO has the software expertise to develop the tool at a fraction of the cost of commercial developers.
- The BRIGHT screen
- MDS-HC CAPs
- The Barthel Index
- CSQ-8
- GP feedback form
- Interview guides
Sensitivity and specificity of the minimal mental status examination for identifying dementia in the elderly: the over-90 study. The Home Care Minimum Data Package: A Valid Instrument to Assess Frail Elderly Living in the Community. Cognitive screening instruments in neuropsychiatry: a report of the Committee on Research of the American Neuropsychiatric Association.
A randomized trial of a comprehensive geriatric assessment and home-based intervention in the care of hospitalized patients. Retrieved from http://www.nzdoctor.co.nz/un-doctored/2010/september-2010/24/ageing-population,-ageing-health-workforce-double-whammy-.aspx. Discharge of older patients from accident and emergency department: functional changes and risk of readmission.
A randomized trial of a screening, case-finding, and referral system for older veterans in primary care. Discharge of the elderly from accident and emergency department: evaluation of follow-up of an outpatient clinic. Birmingham, UK: NHS Modernization Agency and University of Birmingham Center for Health Services Management Statistics New Zealand.
Retrieved from http://www.stats.govt.nz/browse_for_stats/people_and_communities/older_people/demographic-aspects-nz-ageing-population.aspx. A trial of annual comprehensive geriatric home assessments for community-dwelling older adults. Home visits to prevent nursing home admission and functional decline in the elderly: systematic review and meta-regression analysis.
Depression and anxiety in elderly outpatients with chronic obstructive pulmonary disease: prevalence and validation of the BASDEC screening questionnaire.