Cannon , MD Assistant Professor, Department of Orthopedic Oncology, Division of Surgery (current position: Orthopedic Surgeon, The Policlinic, Seattle, WA). Yasko, MD Associate Professor, Chief, Division of Orthopedic Oncology, Department of Orthopedic Oncology, Division of Surgery (now deceased; position at the time of his death: Professor, Department of Orthopedic Surgery, Northwestern University Feinberg School of Medicine, Chicago, IL ).
A Multidisciplinary Approach
The experience of the last few decades has shown that the treatment of most bone sarcomas requires the multidisciplinary cooperation of clinicians, musculoskeletal radiologists and bone pathologists. One of the most critical aspects of coordinating patient care is obtaining complete medical records and pathology specimens.
Suggested Readings
Key Practice Points
Introduction
Lesion Location
An important aspect of imaging bone sarcomas is the relationship of the tumor to the adjacent normal soft tissues and other vital structures, such as the neurovascular bundle. Description of the relationship between the tumor and these adjacent normal structures is of critical importance for the local staging of the bone sarcoma and for the planning of surgical intervention.
Diagnostic Imaging
The architecture of cartilaginous bone formation gives the unique appearance of the chondroid matrix (Figure 2.5, bottom row). Intravenous contrast is also used in subsequent preoperative MRI studies to assess tumor response to therapy (discussed later in this chapter).
Assessment of Tumor Extent
The technique provides a global picture of the entire skeleton and is very sensitive but non-specific. Although CT can be useful in diagnosing a malignant bone tumor, its use in assessing the local extent of the tumor is very limited.
Evaluation of Response to Treatment
Accuracy of radiography in grading and tissue-specific diagnosis - a study of 200 consecutive bone tumors of the hand. Both fine needle aspiration and core biopsy are used for sampling bone tumors; the two techniques are often complementary.
Percutaneous Image-Guided Biopsy for Diagnosis of Bone Sarcomas
For the biopsy procedure to be successful in characterizing bone tumors, appropriate planning is of utmost importance. The biopsy must provide sufficient material so that an unequivocal pathological diagnosis can be established.
Percutaneous Versus Open Biopsy
The rapid diagnosis and short recovery time possible with a percutaneous biopsy, as opposed to an open surgical biopsy, allows for the immediate initiation of appropriate therapy. In a study by Yao et al., only 72% of subsequent open biopsies yielded a specific diagnosis, and the remaining 28% were inconclusive.
Assessment of the Patient
In a study of 141 patients with suspected primary musculoskeletal neoplasms, 25 (18%) required open biopsies due to inconclusive results of percutaneous core biopsies (Yao et al. 1999. However, diagnostic dilemmas after percutaneous biopsy cannot always be resolved with open surgical biopsy.
Prebiopsy Planning
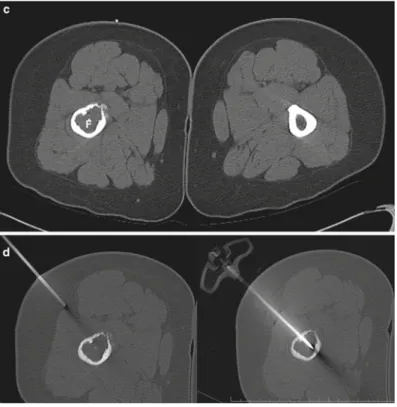
The greatest enhancement is seen at the front of the tumor (T). (c) Transverse ultrasound image (top) of the distal left thigh shows a soft tissue mass (arrowhead) and fractures in the femoral cortex (arrows. Longitudinal ultrasound image (bottom) of the same lesion shows the full length of the biopsy needle (arrow) placed within the tumor.
Imaging Modalities
Endosteal scalloping, destructive lytic changes and faint calcifications are seen. b) With the patient in the prone position, axial T1-weighted (left) and post-contrast fat-suppressed T1-weighted axial MRI scans of the distal femur (right) show heterogeneous enhancement of the femur (F) with tumor extent through the posterior femoral cortex. Interrogation of the needle path with duplex doppler ultrasonography prevents inadvertent vascular injury and hemorrhagic complications.
Biopsy Techniques
Generally, a bone biopsy will begin with FNA of the most appropriate area within the tumor. In cases of suspected osteosarcoma, large (eg, 14-gauge) core biopsy specimens should be obtained with cutting-type needles; at least 4 of these high-quality samples are required for accurate diagnosis and possible subtyping of the tumor.
Postbiopsy Care
Close collaboration and direct communication between the interventional radiologist and cytopathologist enables collection of the appropriate type and quantity of specimens and aids in accurate and efficient diagnosis. In this way, the number of non-diagnostic samples and the need for repeat biopsy are minimized.
Potential Complications
Chapter 4
Orthopedic Oncologic Surgical Specimen Management and Surgical Pathology
Chapter Overview The pathologist is an integral member of the multidisciplinary team central to the successful treatment of bone tumors. The role of the pathologist is to provide morphology-derived information regarding diagnosis and status of disease.
Surgical Pathology Specimens
With the advent of needle biopsy as a reliable diagnostic tool, the need for frozen section diagnosis has greatly decreased. If the frozen section shows metastatic carcinoma, further processing depends on the type of suspected primary tumor.
Preparation of Osseous Tissues by the Surgical Pathologist
In the first of these choices, the skin and soft tissue overlying the tumor-containing bone is incised to the level of the tumor and parent bone. With the removal of the skin and soft tissue from the tumor-containing bone, the full circumference of the bone is available for sectioning.
Gross Description
The essence of this system is the division of the rough description into sections, defined by paragraphs of predetermined content. If a structure is normal, a statement is made about it (for example: “… the articular cartilage is unremarkable”) and no further description is given.
Mapping of Postchemotherapy Specimens
The hallmark of a successful response to therapy is the effacement or disappearance of the neoplastic cells from the involved area. In reporting the results of the response-to-therapy analysis, we do not limit this portion of the pathology report to a simple statement of the tumor necrosis rate.
Pathology Report
As a result, they will look back and forth looking for differences (“the Wimbledon perspective”) rather than listening to a speaker. Recoloring: A final note on “the one that got away”: There are circumstances in which a specimen is dissected and sectioned but must first be formalized before photography can be performed.
Special Studies
Chapter 5
Cases of primary conventional osteosarcoma may occur in older patients, but secondary osteosarcoma is more likely with age. Osteosarcoma of the craniofacial bones and secondary osteosarcoma are two important entities with characteristics that clearly distinguish them from ordinary osteosarcoma.
Diagnostic Workup and Staging
The development of a very clear and mature edge of ossification that defines the border of the tumor represents an excellent response to systemic therapy. The most recent version (seventh edition) of the staging system of the American Joint Committee on Cancer (AJCC) (Edge et al. 2010) includes in the system the size of the tumor and the presence of bypass metastases (Table 5.3.
In addition to tumor size, tumor vascularity is also an indicator of response. A smooth, contiguous area of calcification at the periphery of the tumor is indicative of a good response to chemotherapy.
Rare Variants of High-Grade Osteosarcoma
Osteosarcoma of the Craniofacial Bones
In almost all cases, cure is not possible without surgical excision of the recurrent disease. Craniofacial osteosarcomas tend not to respond to chemotherapy as well as conventional osteosarcomas of the extremities, but there is growing recognition that chemotherapy can improve survival for some patients (Smeele et al. 1997.
Well-Differentiated Intramedullary and Parosteal Osteosarcoma
If there is doubt as to whether a hemicortical resection can be performed with safe margins, it is preferable to fail the entire circumference of the bone rather than risk subsequent recurrence. This change in status suggests that either transformation of the low-grade tumor has occurred or that a small, dedifferentiated component of the original tumor was not appreciated.
Periosteal Osteosarcoma
A hemicortical allograft may not be appropriate if the parosteal osteosarcoma extends partially into the intramedullary space. However, if the percentage of necrosis after preoperative chemotherapy is poor (well below 90%), it may not be beneficial to continue with postoperative chemotherapy.
Dedifferentiated Parosteal Osteosarcoma
Secondary Osteosarcoma
Effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremities. Intensification of preoperative chemotherapy for osteogenic sarcoma: results of the Memorial Sloan-Kettering (T12) protocol.
Clinical Features
With respect to osteosarcoma (Chap. 5), staging systems from both the Musculoskeletal Tumor Society (MSTS) and the American Joint Committee on Cancer (AJCC) can be used. While in other bone sarcomas bone marrow involvement practically never occurs, in Ewing sarcoma it is a well-known phenomenon.
In the Cooperative Ewing Sarcoma Study (CESS-86) from Europe, ifosfamide was used in the treatment of patients at high risk of relapse (Paulussen et al. 2001. -four patients who were surgically treated for Ewing sarcoma between 1990 and 2001 were studied the factors affecting local recurrence a) The rate of local recurrence free survival (LRFS) depended on the response to chemotherapy.
When radiation therapy is administered after surgery, the surgical bed and incision must be included in the radiation field. In general, if patients are candidates for systemic chemotherapy, it should be given first, before treatment of the local recurrence.
Follow-Up
Multimodal therapy for the treatment of non-pelvic, localized Ewing bone sarcoma: IESS-II intergroup study. Multimodal therapy for the treatment of primary, nonmetastatic Ewing bone sarcoma: a long-term follow-up of the First Intergroup study.
Diagnostic Workup
The greatest decrease in agreement from the diagnosis of cartilage to the diagnosis of the exact grade of chondrosarcoma was in tumors of the pelvis. Therefore, at MD Anderson and other sarcoma referral centers, in some cases a biopsy is not considered a critical component of the pretreatment evaluation if the diagnosis of a cartilage tumor (chondrosarcoma) can be made with confidence using radiology. studies.
Radiologic Studies
Low-grade chondrosarcoma of long bones usually has uniform calcification of the tumor matrix. Cortical thickening, widening of the involved region of the long bone, and soft tissue extension are unusual in low-grade cases.
Treatment of dedifferentiated chondrosarcoma remains a challenge due to the high propensity of these tumors to metastasize. The authors reported no statistically significant difference in 5-year survival rates for patients treated with and without adjuvant therapy (chemotherapy and/or radiation).
The spine surgeon performing en bloc resection of spinal chordomas must have knowledge of spinal and paraspinal anatomy. Once the rectum is protected and the superior aspect of the tumor has been identified, the osteotomies and soft tissue dissection required for en bloc resection can be performed entirely from a posterior approach.
Adamantinoma
Clinical investigators at Massachusetts General Hospital reported a local control rate of 53% and an overall survival rate of 50% at 5 years for patients treated with mixed proton/photon radiotherapy (Hug et al. 1995). Stereotactic fractionated radiation therapy has also been investigated as a possible solution. treatment modality for chordates of the skull base (Debus et al. 2000.
Hemangioendothelioma
They most commonly occur in the calvaria, axial skeleton, and long bones of the lower limbs, with the tibia and femur most commonly affected (Ignacio et al. 1999. These tumors may also have intravascular papillary projections with epithelial or histiocyte-like cells (Tillman et al. 1997 .
Hemangiopericytoma
Characteristic features include: (1) sheets of spindle-like cells surrounding numerous capillaries, (2) monotonous round to oval nuclei lacking atypia, (3) indistinct cytoplasmic borders, and (4) in silver staining, a visible reticulin sheath surrounding each tumor cell outside the capillary walls (Tang et al. 1988. When extensive resection is not possible, it has been suggested that a compromise can be made between optimal treatment for cure and optimal treatment for function (Sahin - Akyar et al. 1997.
Low-Grade Fibrosarcoma
Adjuvant radiation therapy has been shown to play a role in the treatment of both primary and recurrent hemangiopericytoma. In the long bones, these lesions tend to be based in the metaphysis and often extend into the epiphysis.
Most patients described in the literature were treated surgically, either with wide excision or amputation (Capanna et al.
Skeletal Reconstruction After Bone Sarcoma Resection
Chapter overview The majority of patients with bone sarcomas can be successfully treated with limb-sparing surgery. Similarly, peripheral nerves can be excised and the limb spared, in selected cases with nerve grafting or tendon transfer; an isolated peripheral nerve resection will usually result in a more functional limb than an amputation.
At our institution, the most common method of fixation involves a long-stemmed prosthesis that spans the length of the allograft and is cemented into both the host bone and the allograft. 9.5 (a) A double-barreled vascularized fibular bone flap. b) Use of this type of flap for reconstruction of the pelvic ring after internal hemipelvectomy.
Another anatomical problem with proximal fibula resection is preservation of the anterior tibial vessels. After tumor resection, the pelvis of the allogeneic graft is carefully shaped to fit the defect.
Wound Defects That Require Soft Tissue Repair
Certain anatomic sites, such as the tibial region, are known to be prone to wound dehiscence and therefore benefit from planned soft tissue reconstruction. A larger than expected allograft may result in a larger implant and may increase the stress on the soft tissue repair.
Finally, overlapping flap harvest and implant preparation shortens the length of surgery. This muscle can be used to cover soft tissue defects over the middle third of the tibia.
