Ganga Krishnamurthy, MBBS Assistant Professor of Pediatrics, Director of Columbia University Medical Center, Neonatal Cardiac Care Morgan Stanley Children's Hospital of. Stéphanie Levasseur, MD, FRCPC assistant professor of pediatrics Columbia University Medical Center Morgan Stanley Children's Hospital of.
CONTINUED
Aerating the lung and establishing pulmonary ventilation induces the physiological changes that support the transition to newborn life (Hooper et al, 2015a). However, it is far too simplistic to assume that the primary benefit of "establishing pulmonary ventilation" is to restore oxygen and carbon dioxide exchange lost after umbilical cord clamping.
AIRWAY LIQUID CLEARANCE BEFORE BIRTH AND DURING LABOR
From a teleological perspective, it makes sense that the physiological changes necessary for survival after birth are caused by the one event that cannot occur in the womb: the aeration of the lungs. Lung aeration not only induces the switch to pulmonary gas exchange, but also causes a very large reduction in pulmonary vascular resistance (PVR), which initiates a series of cardiovascular changes that are also essential for survival after birth (see later).
Airway Liquid Clearance After Birth
The idea that an increased heart rate is a sign of lung ventilation is based on the concept that a low heart rate indicates a vagally induced bradycardia in response to perinatal asphyxia (Dawes, 1968). However, whether the increase in heart rate results from increased oxygenation or an increase in PBF, both occur solely as a result of lung ventilation.

SUSTAINED INFLATION DURING RESUSCITATION
This has implications for respiratory function in the neonatal period (Berger et al, 1996), including an increase in interstitial tissue pressure (Miserocchi et al, 1994). However, laryngeal regulation in the fetus and neonate is very different from that in adults (Harding et al, 1986; Praud et al, 1992).
FACILITATING THE CARDIOVASCULAR TRANSITION AT BIRTH
Fetal Circulation: the Starting Point
Transitioning the Circulation From a Fetal Into a Newborn Circulatory Pattern
Before birth, pulmonary blood flow (PBF) flows toward the lungs (positive flow) only briefly during systole, and then during late systole and most of diastole, PBF is mostly retrograde (negative value), leaving the lungs and passing through the DA. This alters the pressure gradient between the pulmonary and systemic circulation, causing blood flow through the DA to reverse (compared to the fetal condition), predominantly flowing from left to right (Figs 1.4 and 1.5) (Crossley et al , 2009).

Delayed Umbilical Cord Clamping (DCC) and Placental Transfusion
During this time, while most DA blood flow is from left to right, immediate flow is bidirectional; from right to left initially during systole and then from left to right during late systole and throughout diastole (Fig. 1.5). As a result, the flow is initially from right to left and then rapidly changes from left to right as the pressure gradients change.
The Physiology of Umbilical Cord Clamping at Birth
Both the right and left ventricles contribute to the increase in PBF (Fig. 1.4) after lung aeration (Crossley et al, 2009), as the decrease in PVR allows the lung to accept 100%. In addition, if the PVR is reduced before cord clamping, the increase in arterial pressure (afterload) caused by cord clamping is reduced because the pulmonary circulation can serve as an alternative low-resistance route for blood flow (Bhatt et al. , 2013).
Physiologic Based Umbilical Cord Clamping
This is also called physiologically based umbilical cord clamping (PBCC) (Kluckow and Hooper, 2015) or infant-centred umbilical cord clamping (Blank et al, 2018), where the timing of umbilical cord clamping is based on the infant's physiology and not on a particular set. period after birth. Similarly, CPR studies that do not use a table simply involve resuscitating the infant on a heating pad on the mother's legs (Blank et al, 2018).
MANAGING THE ASPHYXIATED INFANT
However, it is possible that the infant's body temperature control will be more stable and less prone to rapid reductions if resuscitated with an intact cord because the placenta is still inside the mother and should warm the infant's blood as it flows through the placenta. On the other hand, given the contribution of warmed placental blood to maintaining the infant's body temperature, using the same heat loss/heat gain procedures used in infants with a ligated cord may increase the risk of hyperthermia in infants resuscitated with an intact cord (ie with delayed cord clamping).
SUMMARY
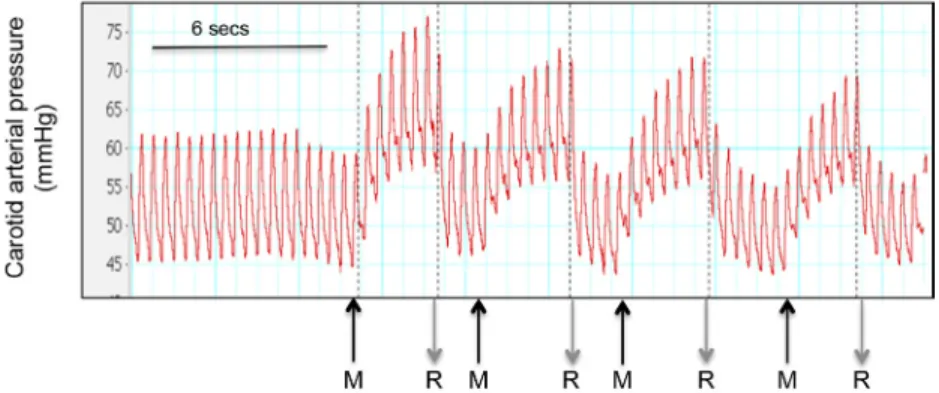
This is because rebound hypertension is the result of a large increase in the sympathetic drive to, among other things, the cardiovascular system, which forms the basis of the fight or flight response. For decades it has been taught that the key to neonatal resuscitation is ventilation of the lungs.
An initial sustained inflation improves the respiratory and cardiovascular transition at birth in preterm lambs. Optimizing lung ventilation at birth using continuous inflation and positive pressure ventilation in preterm rabbits.
STABILIZATION FOLLOWING POSSIBLE PERINATAL ASPHYXIA
CASE1
Questions
However, resuscitation is only one piece of evidence when deciding on hypothermic therapy. If there is no blood loss, there is no indication to provide packed cells or whole blood to augment the volume given the time required to obtain blood.
DIAGNOSIS—A CONTRAST OF 2 CASES CASE 2
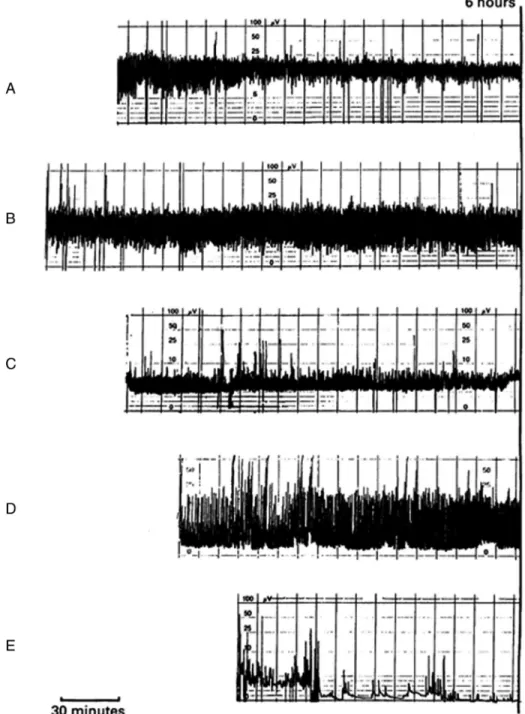
Which of the following aEEG recordings would merit initiation of hypothermia therapy (Fig. 2.4). Determining the need for hypothermia therapy should be done as soon as possible and before the age of 6 hours.
SUPPORTIVE MANAGEMENT FOLLOWING PERINATAL ASPHYXIA
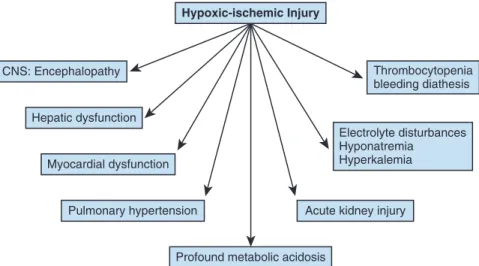
The change in base excess is often called a "tissue washout" of lactate after hypoxia-ischemia. All of the choices can result in a metabolic acidosis, but in the setting of CNS dysfunction suggestive of hypoxia-ischemia, myocardial dysfunction should be considered first.
HYPOTHERMIA THERAPY CASE 4
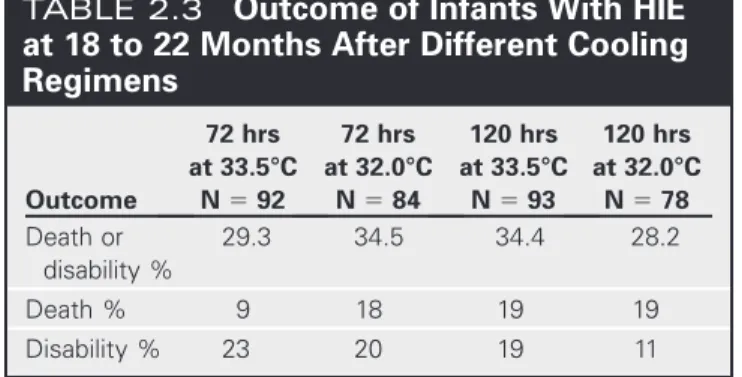
In general, MRI is the imaging method of choice to determine the extent and distribution of the injury. Therapeutic hypothermia is the only neuroprotective therapy that has been shown to reduce an important outcome, death or disability, after 18 to 22 months in rigorous randomized trials.
CONTROVERSIES IN HYPOTHERMIA THERAPY
Frequency and severity of magnetic resonance imaging abnormalities in infants with mild neonatal encephalopathy. Abstract: Perinatal asphyxia is a challenging condition because it represents a modifiable etiology for neonatal encephalopathy with the use of hypothermia.
FETAL FLUID BALANCE
BODY WATER AND SODIUM BALANCE IN TRE NEONATE
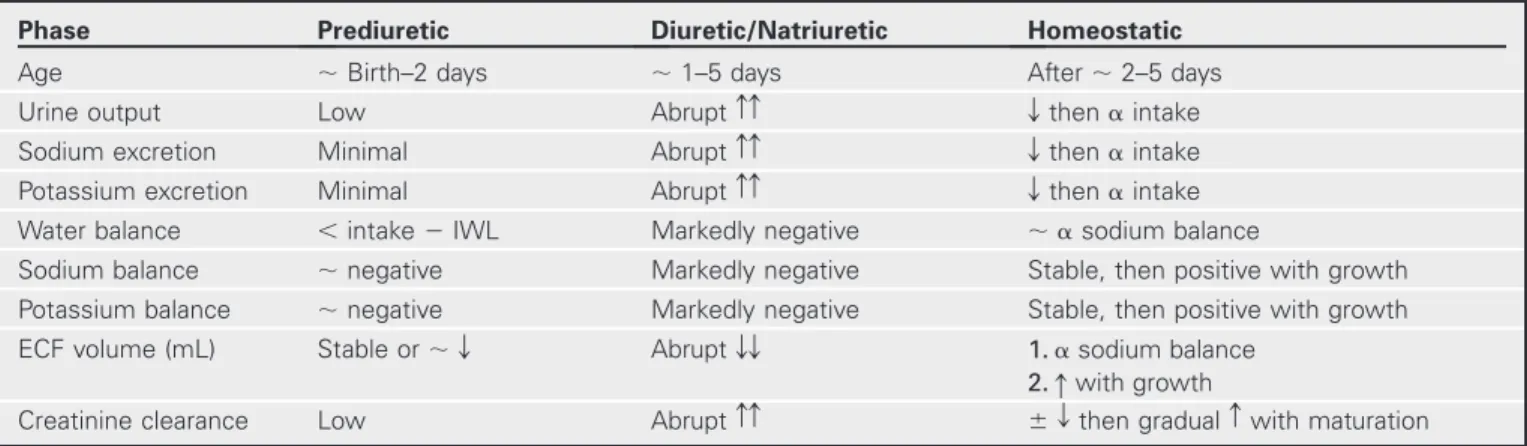
DIURESIS AND NATRIURESIS
When the diuretic/natriuretic phase begins, there is an abrupt increase in the amount of water and Na in the urine, independent of water and Na intake, heralding a contraction of the ECF space. As the ECF space stabilizes at an appropriate volume, urinary water and electrolyte excretion decreases and begins to vary appropriately with intake.
POTASSIUM
At the same time, the low glomerular filtration rate (GFR) in the immediate perinatal period limits the infant's ability to excrete water and electrolyte loads. A decrease in serum K concentration ([K1]) can be expected, as increased supply of water and Na to the distal nephron stimulates K secretion and kaliuresis.
GLUCOSE
- HYPONATREMIA
- HYPERNATREMIA
- HYPERKALEMIA
- INSENSIBLE WATER LOSS
- ASSESSMENT OF RENAL FUNCTION
- BPD, DIURETICS,
What changes do you anticipate regarding fluid and electrolyte status and the baby's weight over the next few days? Therefore, early in the diuretic phase, free water losses exceed sodium losses and serum [Na] increases (Bidiwala et al, 1988).
AND ELECTROLYTE DISTURBANCES
Impaired renal function is traditionally defined as elevated serum creatinine and nitrogenous waste (blood urea nitrogen). In this case the baby had a slight increase in serum creatinine during the first day of life.
![Fig. 3.4 Change in plasma [Creat] in preterm infants without risk factors for acute renal failure over the first 10 days of life as a function of gestational age](https://thumb-ap.123doks.com/thumbv2/azdoknet/10577231.0/56.918.212.720.102.994/change-plasma-preterm-infants-factors-failure-function-gestational.webp)
SUGGESTED READINGS
Hyperglycemia is a risk factor for early death and morbidity in extremely low birth weight infants. Glucose and insulin versus cation exchange resin for the treatment of hyperkalemia in very low birth weight infants.
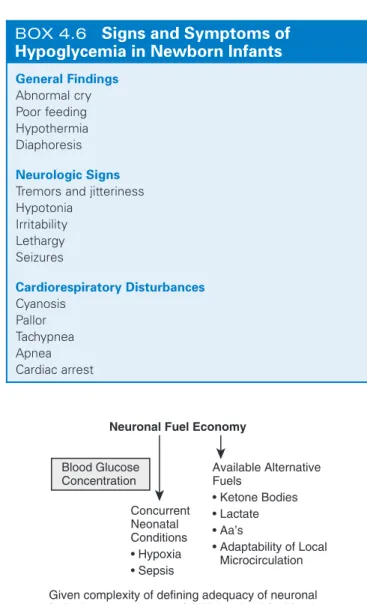
INTRODUCTION
After birth, the normal newborn's plasma glucose concentration falls below the levels that were common in fetal life. When should screening for hypoglycemia occur, and was this infant's screen obtained at the physiological nadir for plasma glucose values.
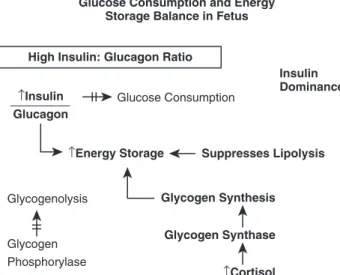
POSTNATAL GLUCOSE HOMEOSTASIS AND TRANSITIONAL NEONATAL HYPOGLYCEMIA
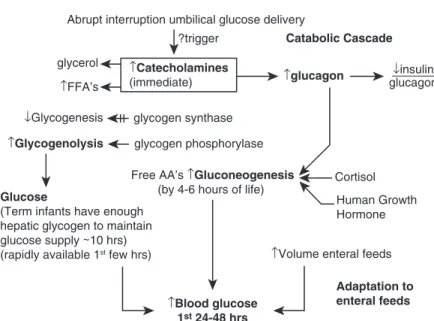
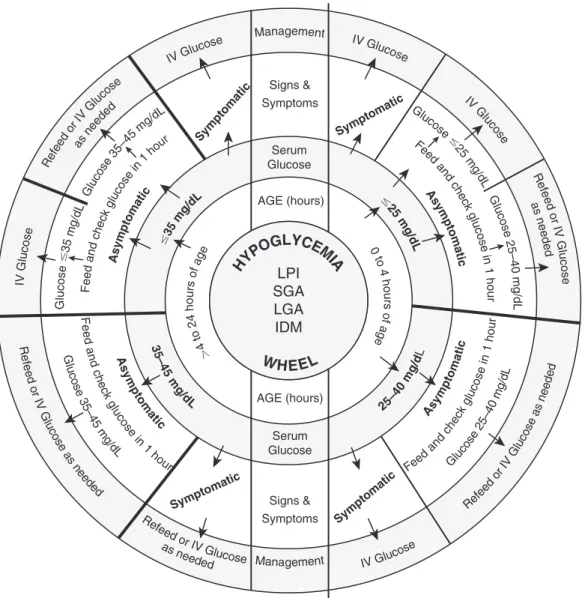
Screening and management of postnatal glucose homeostasis in late preterm and full-term SGA infants, IDM/LGA infants [(LPT) infants 34–366/7 weeks and SGA (0–24 h screen): IDM and LGA 34 weeks ( display 0-12 hours )]. The release of glucose from glycogen provides a readily available source of glucose for the newborn in the first hours after birth.
AAP RECOMMENDATIONS FOR SCREENING AND MANAGEMENT
This misconception arose from the observation of lower plasma glucose levels in premature infants, who were usually starved in the first days of life. These low values are no longer observed in premature infants due to early intravenous feeding and/or enteral feeding.
PEDIATRIC ENDOCRINE SOCIETY
It has long been believed that preterm infants had lower glucose levels than full-term infants during the first 3 days of life and tolerated these lower levels better. Gluconeogenic capacity is limited in premature infants, probably due to the immaturity of the enzymatic pathways.
RECOMMENDATIONS FOR SCREENING AND MANAGEMENT
The fundamental question of how best to manage asymptomatic neonates with low glucose concentrations remains unanswered. Persistence of such low glucose concentrations for long periods (hours, 0.2-3 hours, rather than minutes, although there are no studies in human newborns that determine this period).

DEFINITION OF HYPOGLYCEMIA
If treated and corrected at 48 hours of life, will the glucose level at 6 hours of life cause brain damage. This infant was described as vigorous in the delivery room and therefore, despite being macrosomic, was able to feed within the first hour of life.
OPERATIONAL THRESHOLDS
The child presenting with neurological symptoms requires a more urgent increase in plasma glucose concentration than the asymptomatic one, regardless of the individual plasma glucose concentration. However, the recommendations are not based on evidence of significant morbidity if no action is taken.
RESOLVING DIFFERENCES IN THE AAP AND PES RECOMMENDATIONS FOR CRITICAL
Similarly, there is no evidence that outcomes improve if action is taken at the operational threshold value.
PHYSIOLOGIC RESPONSES
TO HYPOGLYCEMIA AND BRAIN INJURY
Brain glycogen is stored in the astrocyte, making this vessel another important source of neuroprotection. In addition, ketone bodies increase further when the blood glucose concentration is low.
Identifying Risk Factors for Neonatal Hypoglycemia
There are significant differences in brain regional sensitivity to hypoglycemia that contribute to the pattern and distribution of damage, but the reported differences have not been consistent. Several animal and human neonatal imaging studies have shown vulnerability to hypoglycemia in the occipital region, striatum, cingulate cortex, and hippocampus.
NEURODEVELOPMENTAL OUTCOMES IN INFANTS WITH HYPOGLYCEMIA
It is unlikely that any intervention could reduce exposure to a short period of hypoglycemia. In the study by Coors et al., prophylactic dextrose gel did not reduce transient neonatal hypoglycemia or NICU admissions due to hypoglycemia.
WHICH INFANTS TO SCREEN
It is also possible that the exposure group had further exposure to hypoglycemia, as only the first two blood glucose levels were measured, and recurrent low glucose levels are common in children at risk during the first week. It is possible that a brief period of hypoglycemia is a marker for other perinatal problems, which may include side effects during abnormal intrauterine development.
WHEN TO SCREEN
Fortunately, blood glucose rises by 3 hours of age, even in the absence of enteral nutrition. Even in an infant at risk for hypoglycemia, it is best to avoid measuring blood glucose in the first 2 hours after birth in an asymptomatic infant.
LABORATORY MEASUREMENTS OF GLUCOSE
Blood glucose concentrations show a cyclic response to an enteral feeding, reaching a peak about one hour after feeding and a nadir just before the next feeding is due. Because the purpose of blood glucose monitoring is to identify the lowest blood glucose level, it makes the most sense to measure a value immediately before the next feeding.
CLINICAL SIGNS OF HYPOGLYCEMIA
It seems inappropriate to perform early blood glucose measurements in any infant during this drop immediately after birth, because a normal physiologic decrease cannot be distinguished from an abnormal one. No studies have demonstrated harm from a few hours of asymptomatic low glucose levels during this postpartum period to restore physiological homeostasis.
PERSISTENT HYPOGLYCEMIC DISORDERS
From Thornton PS, Stanley CA, DeLeon DD, et al: Pediatric Endocrine Society Recommendations for the Evaluation and Management of Persistent Hypoglycemia in Neonates, Infants, and Children, J Pediatr. It is reasonable to use the AAP algorithm for the first 24 hours and then use more than 45 mg/dL as a working threshold for 24 to 48 hours.
DEXTROSE GEL FOR TREATMENT OF HYPOGLYCEMIA
To increase the detection of these persistent hypoglycemic syndromes, it is prudent to use the AAP and PES recommendations. More data on the frequency and success of diagnosing persistent hypoglycemia will be needed to support this strategy.
CONCLUSION
Summary: Low blood glucose levels are one of the most common problems in the baby's room. The data needed to reach consensus on low blood glucose levels does not yet exist.
THE SERUM TOTAL BILIRUBIN
Not all degrees of hyperbilirubinemia are necessarily dangerous, but because of the potential for STB to continue to increase, phototherapy may be indicated. By facilitating the elimination of bilirubin, further growth of STB can be limited, thus preventing the neurotoxicity potential of bilirubin.
WHAT DOES IT REPRESENT?
Instead, after some background information on neonatal hyperbilirubinemia, the reader will be presented with a number of current clinical cases drawn from the authors' experience. The reader is encouraged to put themselves in the driver's seat and actually guide the patients, making clinical decisions based on the options presented.
The STB: a Delicate Balance of Forces
A third cause of imbalance may result from failure of the conjugation system in the absence of any hemolysis, as in Crigler-Najjar syndrome. Provided the drainage is functional, an inflow of water should not cause the water level to rise.
Is the STB Predictive of Bilirubin Neurotoxicity?
A partial blockage of the drain can cause a high water level even with a partially open tap. Kaplan et al have demonstrated this concept mathematically using a production-conjugation index that illustrates the contribution of the combined forces of bilirubin production and conjugation to STB at any given time.
If the STB Is Not a Good Predictor of Bilirubin Neurotoxicity, Then What Is?
Given the unreliability of hematologic indices reflecting hemolysis in the newborn, it may be difficult to distinguish between disorders associated with increased production or increased secretion. However, unbound bilirubin determination is currently largely unavailable for routine clinical use, and STB remains the main laboratory indication used for clinical decision-making in neonates with hyperbilirubinemia.
DEFINITIONS
Jaundice and Hyperbilirubinemia
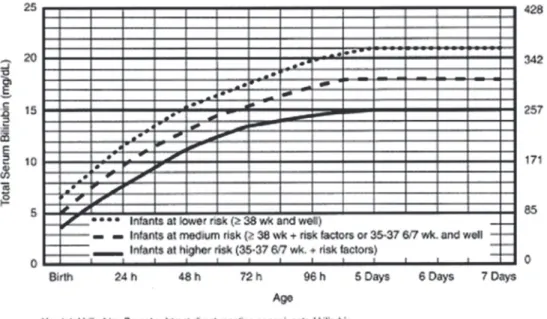
The Hour-Specific Bilirubin Nomogram
Bilirubin Encephalopathy and Kernicterus
PHYSIOLOGY OF BILIRUBIN PRODUCTION AND METABOLISM
Bilirubin Formation
Bilirubin Binding to Serum Albumin; Unbound Bilirubin
Bilirubin Uptake
Bilirubin Conjugation and Elimination
Genetic Control of Bilirubin Conjugation
Excretion of Bilirubin Into the Bowel and the Enterohepatic Circulation
Direct bilirubin is secreted into the bile and then to the intestine from where it is excreted in the stool. The presence of the enzyme beta-glucuronidase in the colon deconjugates bilirubin glucuronides and allows the reabsorption of bilirubin into the bloodstream, thus adding to the bilirubin pool.
INCREASED HEMOLYSIS: A RISK FACTOR FOR HYPERBILIRUBINEMIA AND BILIRUBIN
The resulting increased intestinal stasis with reduced secretion will allow for even greater reabsorption of bilirubin.
ABO ISOIMMUNIZATION CASE 2
IVIG in Immune Hemolytic Anemia
Increased Risk for Bilirubin Neurotoxicity Associated With Hemolysis
G6PD deficiency is particularly well known in demonstrating normal hemoglobin and hematocrit values in the presence of abnormally high STB values, most likely attributable to hemolysis. In cases of overt hemolysis including isoimmune hemolytic disease and G6PD deficiency, the AAP Subcommittee on Hyperbilirubinemia recommends a more aggressive approach to the management of hyperbilirubinemia, including initiation of phototherapy or exchange transfusions at lower STB levels. than in neonates without obvious hemolytic etiology.
G6PD DEFICIENCY: AN IMPORTANT CAUSE OF KERNICTERUS
This baby looks like a pumpkin!" While waiting to be seen by a doctor, the baby became apneic and required intubation and ventilation. The baby was admitted to the pediatric ward, an IV placed, antibiotics given, and phototherapy started.
Acute Bilirubin Encephalopathy: to Exchange or Not to Exchange?
Parents should have been instructed on how to recognize jaundice and what to do if their baby becomes jaundiced. The parents of this infant should have been warned of the high-risk nature of their ethnicity regarding the potential for G6PD deficiency.
CLINICAL EFFECTS OF SEVERE NEONATAL HYPERBILIRUBINEMIA
If the child had been born in Greece, G6PD deficiency would have been screened for as part of a national screening program and the parents given preventive instructions even before the screening results were available. Although the trigger for hemolysis in G6PD-deficient babies often cannot be identified, the parents of this baby should have been warned about the dangers of eating fava beans, using clothing that had been stored in naphthalene-containing mothballs, or using drugs or medications with - out consulting a doctor beforehand.
Acute Bilirubin Encephalopathy
Bilirubin toxicity – manifesting as acute bilirubin encephalopathy with the possibility of kernicterus or the less devastating bilirubin auditory neuropathy and bilirubin-induced neurological dysfunction (BIND) – will most likely not have been encountered by the majority of readers. Although a comprehensive account of bilirubin-induced neurological disease is beyond the scope of this chapter, in the following paragraphs we will briefly describe the clinical picture of neonates exposed to and affected by high levels of STB.
Chronic Athetoid Cerebral Palsy: Kernicterus
SUBTLE BILIRUBIN ENCEPHALOPATHY AND AUDITORY NEUROPATHY
Bilirubin-Induced Neurologic Dysfunction (BIND)
Auditory Neuropathy/Dyssynchrony
LATE PREMATURITY CASE 4
Every STB Value Should Be Plotted on the Bilirubin Nomogram
Jaundice Associated With Prematurity
Jaundice Associated With Late Preterm Infants
Nonhemolytic Jaundice”: Is There Such an Entity?
DIMINISHED BILIRUBIN CONJUGATION AND NEONATAL HYPERBILIRUBINEMIA
Gilbert Syndrome
BREASTFEEDING AND BREAST MILK JAUNDICE
Mutations of the UGT1A1 gene, including a promoter (TA)7 polymorphism (UGT1A1*28), or the G71R mutation (UGT1A1*6) may contribute to the development of hyperbilirubinemia in breastfed infants. Treat the infant with phototherapy to prevent STB concentrations from rising to potentially neurotoxic levels.
Crigler-Najjar Syndrome
Phototherapy was instrumental in lowering the STB value, and the child was discharged only to be readmitted 3 days later with a STB value of 23.0 mg/dL. Discontinuation of breastfeeding and substitution with infant formula for 1 to 3 days usually causes a rapid decrease in STB concentration, especially when STB concentrations reach levels that may endanger the infant.
Hypothyroidism
A lack of proper technique, overwhelm, cracked nipples, small amounts of milk and fatigue can impair effective breastfeeding on the part of the mother. In the infant presented here, the sequence of reimaging and phototherapy repeated itself several more times.
EFFECT OF RACE AND ETHNIC BACKGROUND ON NEONATAL HYPERBILIRUBINEMIA
This infant is of African American heritage and is at very low risk for neonatal hyperbilirubinemia. Black ethnicity comprises 25% of the US-based Kernicterus Registry and was over-represented in the UK and Ireland survey.
Additional Racial Aspects of Hyperbilirubinemia
Within the African American population, there is a subgroup at risk for extreme hyperbilirubinemia and kernicterus. The low-risk categorization of black newborns may therefore no longer be appropriate, and answers A and B are incorrect.
PREDISCHARGE EVALUATION FOR PREDICTION OF HYPERBILIRUBINEMIA
Indeed, the AAP (2004) statement on hyperbilirubinemia lists black ethnicity among conditions that decrease the risk of hyperbilirubinemia. Some of these cases may be due to concurrent G6PD deficiency and others due to disadvantaged social status.
Universal Predischarge Screening
TRANSCUTANEOUS BILIRUBINOMETRY
In a recent study from California, Wickremasinghi et al. a lower incidence of moderate hyperbilirubinemia (STB $20 mg/dL) in black infants, an equal incidence of STB 25 mg/dL or greater in black and Caucasian infants, and an increased incidence of dangerous hyperbilirubinemia (STB $30 mg/dL) in black newborns compared to white infants. In their 2004 clarification of the AAP guidelines, Maisels et al suggest measuring STB if (1) TcB is 70% of the STB value recommended for phototherapy, (2) TcB is above the 75th percentile on the bilirubin nomogram or above the 95th percentile on a TcB nomogram, and (3) a post-discharge TcB value is above 13 mg/dL.
TREATMENT OF NEONATAL HYPERBILIRUBINEMIA
Weeks’ Gestation and Above
Reprinted with permission from the American Academy of Pediatrics Subcommittee on Hyperbilirubinemia: Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation, Pediatrics. Reprinted with permission from the American Academy of Pediatrics Subcommittee on Hyperbilirubinemia: Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation, Pediatrics.
Premature Infants ,35 Weeks’ Gestation
Therefore, the irradiation should be limited to that which controls the possible further increase of STB and allows its reduction. Phototherapy should be urgently instituted in cases of excessive hyperbilirubinemia, and procedures should be performed while the infant is receiving phototherapy.
Low Bilirubin Kernicterus
Irradiance of at least 30 mW/cm22/nm21 (verified with an appropriate irradiance meter calibrated over the appropriate wavelength range). Demonstration of a decrease in total bilirubin concentration during the first 4 to 6 hours of exposure.
SPECIAL INVESTIGATIONS IN KERNICTERUS MRI Findings in Kernicterus
Brainstem Auditory Evoked Response (BAER)
Cochlear Implants
SUGGESTED READING
An approach to the management of hyperbilirubinemia in preterm infants less than 35 weeks' gestation. Prospective surveillance study of severe hyperbilirubinemia in newborns in the UK and Ireland.
INDICATIONS
- continued)
- continued)
- continued)
- continued)
At least 1.5 g/kg/day of parenteral amino acids is necessary to prevent significant protein breakdown (catabolism). Protein intake of 4 to 4.5 g/kg/day is recommended for preterm infants with slow weight gain.
NUTRIENT REQUIREMENTS
Nevertheless, providing adequate nutritional support to high-risk preterm infants remains a significant clinical challenge. In addition, emphasis is placed on areas where further research is needed to determine optimal nutritional support to improve outcomes in this population.
INITIATION AND ADVANCEMENT OF ENTERAL NUTRITION
A standardized feeding protocol for VLBW that includes initiation of enteral nutrition within 6 to 48 hours of birth has been associated with improved outcomes, including reduced parenteral nutrition days, reduced risk of NEC, and reduced rates of late-onset sepsis. Several clinical studies have shown reductions in the number of days to complete enteral feeding, the total number of days withheld from enteral feeding, and the days of hospital stay.
Advancement of Enteral Nutrition
The presence of umbilical lines, including an umbilical arterial catheter, is not a reason to stop enteral feeding. Initiation of early enteral feeding should not be delayed until breast milk is available; donor human milk can be used as a bridge until the mother's milk supply is established.
Initiation of Enteral Nutrition
Several studies have shown a decrease in the incidence of NEC with the implementation of standardized feeding protocols. Of note, these investigators found no difference in the composite outcome of NEC or death between groups, although the study was not sufficiently powered to demonstrate a difference in NEC.
Intrauterine Growth Restriction (IUGR)
Investigators in the United Kingdom have recently completed the Speed of Growth of Milk Feeding Trial (SIFT; . NCT01727609). The primary outcome was the number of days of full enteral feeding in the first month after birth; infants randomized to early feeding progression were found to have a 2-day advantage in the number of days of full enteral feeding and a reduction in the number of days of parenteral feeding.
HUMAN MILK CASE 2
- BANKED DONOR HUMAN MILK
- COMPOSITION OF PREMATURE HUMAN MILK
- FORTIFICATION OF HUMAN MILK
- PRETERM FORMULA
- and 4 are true; the remaining statements are all false
Pasteurized donor human milk is recommended for premature babies if mother's own milk is not available. In the first 2 weeks of lactation, the protein content of preterm human milk is typically 1.4 to 1.6 g/dL.
MONITORING GROWTH AND OUTCOMES
Postnatal Growth Failure – Incidence and Etiology
CONSEQUENCES OF POSTNATAL GROWTH FAILURE
The relationship between poor in-hospital weight gain and head circumference growth and adverse neurological outcomes, such as low Bayley cognitive scores, moderate to severe cerebral palsy, and severe neurodevelopmental disorders, is well established. Therefore, it is important to monitor not only weight, but also height (with height board) and head circumference weekly to identify and intervene in growth disorders in the neonatal intensive care unit.
SPECIAL CONSIDERATIONS
BRONCHOPULMONARY DYSPLASIA
Although the rate of postnatal growth failure among preterm infants is improving, it remains a significant problem, especially given that in-hospital growth failure occurs at a critical time in development. Indeed, improved linear growth is associated with significant increases in language, cognitive, and motor scores at 2 years of age.
Implementation of this practice varied across centers due to availability and cost issues.
POSTDISCHARGE NUTRITION
POSTDISCHARGE NUTRITION IN THE BREAST-FED INFANT
POSTDISCHARGE NUTRITION IN THE FORMULA-FED INFANT
Iron and Vitamin Supplementation
POSTDISCHARGE NUTRITION IN THE LATE-PRETERM INFANT
Data show that these infants—compared to term infants—are at increased risk for transient medical problems such as hypothermia, hypoglycemia, hyperbilirubinemia, respiratory distress, and poor feeding.
HOW TO APPROACH ANEMIA IN NEWBORN
Anemia is usually well tolerated in the newborn, especially if it is a gradual process, until a critical level or threshold is reached. In the premature baby, the bleeding may be clinically visible (pulmonary) or not (brain, liver capsule, etc.).
PHYSIOLOGY OF OXYGEN DELIVERY
Later anemia, after the second week, is usually the result of upstream conditions (as mentioned earlier) although in preterm it can be anemia of prematurity, while in the term newborn it is more typical of physiologic anemia. For this reason, we have begun the chapter with a short section on physiology to provide a foundation that will be useful throughout the chapter.
Step One: The Alveolar–Endothelial Interface
Step Two: From the Alveolus to the Bloodstream
Oxygen Transport to the Tissue
Flow of RBC in the Circulation
NORMAL HEMATOLOGICAL VALUES Hemoglobin
Ontogeny of Hemoglobin and Globin Chains
Hemoglobin vs. Hematocrit
Physiology of Red Cell Production
Erythropoietin (Epo)
This has been suggested as a biomarker of the extent and timing of fetal hypoxia (Buonocore et al, 1999). There have been many attempts to use the physiology of hypoxia as a guide to transfusion.
Iron Balance
The time response is over 24 hours duration, making this a potential "timer" of the degree of relatively chronic fetal hypoxia (Christensen et al, 2014).
Other Controllers of Erythroblastosis
Range of Normal Red Blood Cell Indices in the Fetus and Neonate
Rates of hemoglobin synthesis and erythrocyte production are low in the immediate postnatal period because of the dramatic increase in tissue oxygenation. This is further compounded by a shortened life span of red blood cells and plasma dilution with an increase in blood volume related to growth.
DISORDERS OF ANEMIA
This is mainly governed by three factors: the surface-to-surface/volume contact, the viscosity of the cell cytoplasm, and the intrinsic changes in the membrane of fetal and neonatal erythrocytes. These factors together lead to a significantly greater drop in hemoglobin concentration in the first weeks of life in premature infants compared to term infants.
Definition of Anemia
Reticulocyte counts subsequently increase in response to the Hb nadir due to erythropoiesis. This can be identified from either a change in the slope (steeper) of the oxygen delivery–.
Reduced Production
An example would be the determination of the Hb value adjacent to the onset of anaerobic respiration. Regardless of definition, the etiology of anemia can be considered under the broad headings of reduced output, hypovolemia, or bleeding.
Nutritional Anemia
Although this physiological approach to the definition of anemia may be ideal, it is too impractical for general application. Other less common deficiencies in newborns include vitamin E deficiency, which results in a hemolytic anemia.
Genetic Syndromes
This is further influenced by the shift towards delayed cord clamping and the likelihood of adverse intellectual development (Chaparro et al, 2006). Worldwide, avoiding childhood iron deficiency is the most important reason for using delayed cord clamping.
Fetal and Neonatal Hemorrhage
The use of Epo to prevent and treat anemia in premature babies can also lead to iron deficiency when iron supplementation is insufficient. B12 deficiency can also result from malabsorption in newborns with short bowel syndrome and with inborn errors of metabolism, including a deficiency of haptocorrin and.
Feto–Maternal Hemorrhage
Placental Abruption, Placenta Previa, and Vasa Previa
CONTINUED
An echocardiogram shortly after admission to the nursery shows a structurally normal heart with fractional shortening of 30% and a patent ductus arteriosus with left-to-right shunting throughout the cardiac cycle. An echocardiogram shortly after arrival shows a structurally normal heart with D-shaped flattening of the interventricular septum, fractional shortening 28%, and a patent ductus arteriosus with a completely right-to-left shunt.
Intrapartum Hemorrhage
CONTINUED
Hemolysis
Sepsis and Disseminated Intravascular Coagulopathy (DIC)
He has bloody meconium filling the endotracheal tube and a "white out" on the subsequent chest radiograph. Matthew likely has a number of concurrent problems, including a consumptive coagulopathy (DIC) with possible hemolysis (toxin derived) and blood loss.
Isoimmunization
The transfusion laboratory should be notified that an exchange transfusion may be required in the next few hours. The goal of exchange transfusion is to reduce unconjugated bilirubin and circulating maternal antibodies and increase Hb.
Congenital Red Blood Cell Defects
Practice varies, but in many countries the blood used for exchange transfusion is irradiated to destroy the donor's white blood cells, thereby reducing the risk of graft-versus-host disease (GVHD) in the host. Intensive phototherapy should be used initially, although exchange transfusion should be considered in this scenario, as the physician will have problems with unconjugated bilirubinemia and developing anemia.
Anemia of Prematurity (AOP)
It is inherited as an autosomal dominant condition, but it can also be the result of a new mutation. The laboratory often describes polychromasia, meaning many colors, when both mature and immature erythrocytes (nucleated red blood cells) are found in the circulation.
Scenario A
The timing and volume of transfusion in the first days of life in a very preterm neonate remains unclear despite a number of randomized trials. Before determining the volume of transfusion, one should first consider the likely volume status of the circulation—.
Scenario B
Nevertheless, many clinicians will use the PINT/IOWA studies (Kirpalani et al, 2006; Bell et al, 2005) or the Cochrane summary (Whyte and Kiriplani, 2011) to address transfusion thresholds. In addition, most physicians use a volume of 10 to 15 ml/kg, but there are few guidelines for this practice.
PART E AVOIDANCE AND MANAGEMENT OF ANEMIA
Deferred Cord Clamping
Erythropoietin and Anemia of Prematurity
Risks of Epo in Treating Anemia of Prematurity
Red blood cell alloimmunization during pregnancy during the years 1996-2015 in Iceland: A nationwide population study. Effect of the arterial oxygenation level on cardiac output, oxygen extraction and oxygen consumption in low birth weight infants receiving mechanical ventilation.
EFFECTIVE PRENATAL CARE FOR DECREASING RDS
In this case, which of the following prenatal interventions will have the MOST beneficial effect on reducing the severity of RDS. Delivery is advised because the child is moderately premature and the risk of RDS is negligible.
Antenatal Steroids for Pharmacologic Acceleration of Fetal Lung Maturity
Extensive research into the treatment of RDS has led to major improvements in the care of preterm infants and increased survival. Tocolysis to delay preterm labor would not be effective and therefore should not be offered given her previous preterm birth.
Transfer to Tertiary Facility
Longstanding recommendations from the American College of Obstetricians and Gynecologists call for routine administration of prenatal steroids to women between 24 and 34 weeks of gestation who are at risk for preterm labor. Antenatal corticosteroids should also be considered for pregnant women from the 23rd week of gestation and for pregnant women between 34 and 36 weeks of gestation, in light of recent evidence showing benefits for steroid-exposed infants born within this gestational age.
Tocolytic Therapy
DELIVERY ROOM STABILIZATION
Delayed Cord Clamping
Thermoregulation
Ventilation
Oxygenation
Provide continuous positive airway pressure (CPAP)
PROPHYLACTIC INTUBATION WITH SURFACTANT ADMINISTRATION VERSUS
INDICATIONS FOR INTUBATION AND SURFACTANT ADMINISTRATION
SURFACTANT THERAPY
Type of Surfactant: Animal-Derived Versus Synthetic
Dosing of Surfactant: Single Versus Multiple
Prophylactic Versus Selective Surfactant
Early Selective Versus Delayed Selective Surfactant
Alternative Methods of Surfactant Administration
Another strategy that avoids intubation and mechanical ventilation altogether is administration of surfactant via a thin intratracheal catheter placed under direct visualization by laryngoscopy in spontaneously breathing infants. She was supported on early CPAP at birth but eventually required intubation due to a rising Fio2.
MECHANICAL VENTILATION STRATEGIES IN RDS
Compared with the strategy of early CPAP at birth, as discussed previously, a meta-analysis of nine trials (1551 infants) showed no difference in outcomes between prophylactic INSURE or early CPAP. A meta-analysis of six RCTs involving a total of 895 infants demonstrated reductions in mechanical ventilation (RR 0.66, 95% CI) and the composite outcome of BPD or death (RR 0.75, 95% CI) using this less invasive method of surfactant administration .LISA) via thin catheter compared to traditional endotracheal tube administration.
Low Tidal Volume, Low Peak Inspiratory Pressure
After successful intubation and surfactant administration, the respiratory therapist asks about ventilator settings to turn on the patient. Rate of 30 breaths per minute (bpm), inspiration time of 0.8 seconds, peak inspiratory pressure (PIP) of 20 cm H2O for tidal volume of 8 ml per breath, PEEP of 8 cm H2O.
Moderate Positive End Expiratory Pressure
Fast Ventilator Rate and Short Inspiratory Time
Permissive Hypercapnia
EXTUBATION
OXYGENATION TARGETS
DIFFERENTIAL DIAGNOSIS OF RDS
Infection
Transient Tachypnea of the Newborn
Pneumothorax
Persistent Pulmonary Hypertension of the Newborn
Congenital Lung Malformations
Critical Congenital Heart Disease
Most babies with critical congenital heart disease are now detected by prenatal ultrasound. Of note, complete anomalous pulmonary venous return with occluded pulmonary veins is particularly difficult to detect on prenatal ultrasound and can closely mimic RDS postnatally.
INITIAL DIAGNOSTIC EVALUATION IN RDS Chest X-Ray
Arterial Blood Gas
Sepsis Workup
Echocardiography
CASE STUDY 8
A and B only
PHARMACOLOGIC ADJUNCTS Caffeine
Vitamin A
Standard courses of vitamin A supplementation (5000 international units intramuscularly given three times a week for 4 weeks) are typically started within the first 4 days after birth.
Postnatal Steroids
Closure of PDA
PATENT DUCTUS ARTERIOSUS AND RDS
Pneumothorax
COMPLICATIONS OF RDS
Pulmonary Hemorrhage
Bronchopulmonary Dysplasia
Retinopathy of Prematurity
UNIQUE CHALLENGES IN MECHANICAL VENTILATION OF NEWBORN INFANTS
Safe and effective respiratory support of newborn infants requires a good understanding of pulmonary physiology, familiarity with the available evidence regarding the management of respiratory failure and knowledge of the capabilities of the ventilators at one's disposal. Blood gas analysis and chest radiographs complete the picture, but are not sufficient by themselves to provide a complete assessment of the adequacy of respiratory support.
Lung Mechanics
Invasive ventilation is largely reserved for a relatively small number of the most immature or very sick full-term infants, resulting in less experience for trainees and physicians. These more immature patients may be uniquely susceptible to lung injury due to the very early stages of lung development at which they are born, making the use of ventilatory strategies that minimize VALI all the more critical.
Uncuffed Endotracheal Tubes
The clinician must also recognize that individualized patient management is the best approach, and this requires frequent assessment of the patient's response to treatment and regular assessment of all available information, including physical examination, assessment of patient-. However, some degree of lung injury is probably inevitable in mechanically ventilated extremely preterm infants even with optimal respiratory support.
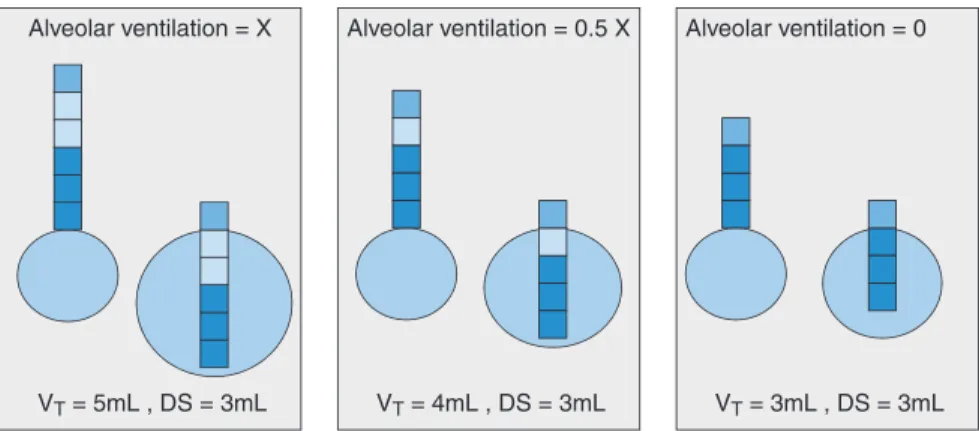
Measurement of Tidal Volume
This remote placement avoids the extra wires and added instrumental dead space of a flow sensor in the airway opening, but results in gross overestimation of the true VT, due to compression of the gas in the circuit, expansion of the circuit and flow. about ETT. The tidal volume loss in the circuit is proportional to the compliance of the ventilator and humidifier circuit (and the compressibility of the volume of gas they contain), relative to the compliance of the patient's lungs (Fig. 10.1).
INDICATIONS FOR MECHANICAL VENTILATION
In large patients with a cuffed ETT, the measured volume at the ventilator correlates reasonably well (with appropriate corrections) with the actual VT entering the lungs. In small infants whose lungs are very small and therefore relatively non-flexible, the volume loss to the circuit is proportionately much greater and not easily corrected, especially if there is a significant ETT leak.
CHOOSING THE VENTILATOR MODE AND INITIAL SETTINGS
EXTREMELY LOW BIRTH WEIGHT INFANT WITH RDS
The basic functionality of a conventional mechanical ventilator is much like that of the T-piece resuscitator (Fig. 10.2). Appropriate inspiratory time depends on the time constants of the respiratory system of your patient.
ASSESSMENT OF VENTILATOR SUPPORT AND SUBSEQUENT ADJUSTMENTS
Your goal is to get Fio2 below 0.30, so you should choose a PEEP of 6 cmH2O and increase in 1 cmH2O increments to a maximum of 8 cmH2O if high oxygen demand persists.
CASE 1, CONTINUED
It is important to understand that the tidal volume entering the lungs results from the combined inspiratory efforts of the infant (when present) and the positive inflation pressure delivered by the ventilator (Fig. 10.6). In this way, the work of breathing is gradually transferred from the ventilator to the baby.
TAILORING VENTILATOR SETTINGS AND STRATEGY TO UNDERLYING
TERM INFANT WITH MECONIUM ASPIRATION SYNDROME (MAS)
CONTINUED)
COMPLICATIONS OF MECHANICAL VENTILATION
PRETERM INFANT WITH RDS
CONTINUED)
CASE 3, CONTINUED
As a result, gas will preferentially enter the already ventilated part of the lung, causing overexpansion with each respiratory cycle, resulting in volutrauma even at normal tidal volumes. The atelectatic part of the lung is also adversely affected by the effusion of protein-rich edema fluid, which inactivates the surfactant.
VOLUME-TARGETED VENTILATION CASE 3, CONTINUED
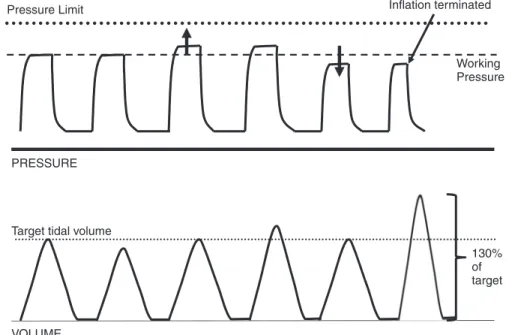
The previous inflation's exhaled VT is compared to the target value, and the inflation pressure for the next inflation is adjusted up, down, or unchanged based on that comparison. The difference is that with VTV, VT becomes the primary control variable and PIP oscillates to maintain VT.
CHALLENGING CLINICAL SCENARIOS CASE 4: TINY INFANT WITH RDS AND
CONTINUED)
The ventilator PIP is still occasionally close to PEEP level, but then rises to the limit when the baby stops her breathing effort. Note that the infant receives no inflation pressure above PEEP, resulting in what is basically endotracheal CPAP.
HIGH-FREQUENCY VENTILATION CASE 4 (CONTINUED)
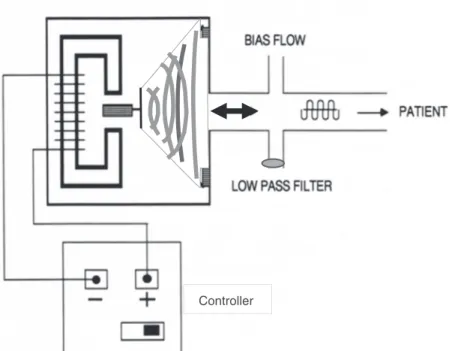
The balance between the inflow of fresh gas (bias flow) and the resistance of the low-pass filter determines the mean airway pressure. Bronchopulmonary dysplasia (BPD) is the most common and prognostically one of the most important complications associated with prematurity.
EPIDEMIOLOGY CASE 1
Chronic impairments in respiratory and cardiovascular health, poor growth and neurodevelopmental delay are all more common in preterm infants with than without BPD (Berkelhamer et al, 2013; Bott et al, 2006; Carraro et al, 2013; Cristea et al, 2013 ; Doyle et al, 2006; Ehrenkranz et al, 2005). The term bronchopulmonary dysplasia was introduced by Northway and colleagues in 1967 to describe the clinical, radiologic, and pathologic respiratory findings that developed in premature infants after resolution of severe respiratory distress syndrome (RDS).
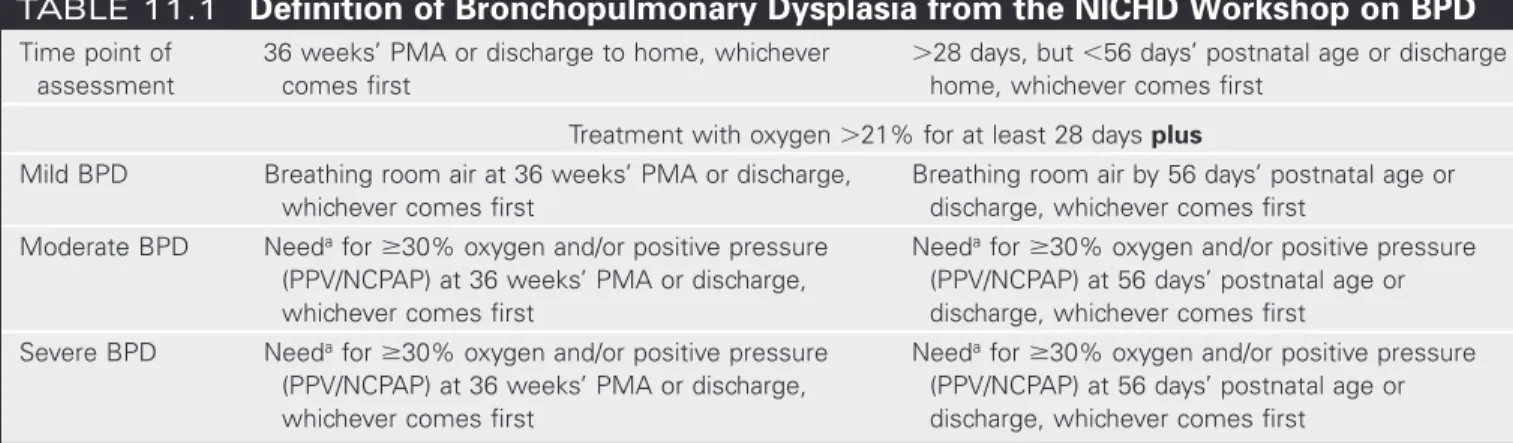
Diagnostic Criteria
Moderate BPD Needa for 30% oxygen and/or positive pressure (PPV/NCPAP) at 36 weeks' PMA or discharge, whichever comes first. Severe BPD Needa for 30% oxygen and/or positive pressure (PPV/NCPAP) at 36 weeks' PMA or discharge, whichever comes first.
Incidence of BPD
ANTENATAL DETERMINANTS OF BPD CASE 2
It was an uneventful pregnancy except for ultrasounds showing fetal growth restriction (10th percentile) of a female singleton. It is unknown if she is colonized with group B Streptococcus (GBS), but vaginal swabs are taken on admission.
Intrauterine Growth Restriction and Small for Gestational Age at Birth (Table 11.5)
Preterm infants with birth weights more than 1 standard deviation below the mean had an over threefold higher risk of BPD (Bose et al, 2009). There is evidence that postnatal growth restriction, often observed in very immature preterm infants (Cooke et al, 2004) and resulting from inadequate nutrient intake, represents an additional risk factor for the development of BPD (Bhatia and Parish , 2009; Moya, 2014). , emphasizing the importance of adequate nutrition in this group (Bhatia and Parish, 2009).
Chorioamnionitis
Also of interest are recent studies demonstrating a reduced risk of BPD despite compromised postnatal growth in exclusively breastfed preterm infants (Spiegler et al, 2016). A 2012 systematic meta-analysis that included the majority of these studies (0.15,000 preterm infants) found an association between histological chorioamnionitis – but not clinical chorioamnionitis – and BPD (Hartling et al, 2012).
Antenatal Corticosteroids (Table 11.6)
A prospective national cohort study in France that included 2513 preterm infants under 32 weeks' gestation found no association between histological chorioamnionitis and BPD (Torchin et al, 2017). These late adverse side effects suggest caution for the use of ACS after pregnancy at 24 to 34 weeks' gestation (Jobe and Goldenberg, 2018).
Gestational Age Dependence
ACS treatment has been extended to viable pregnancies before 24 weeks' gestation, mostly defined as pregnancies at 220⁄7 to 236⁄7 weeks (Jobe and Goldenberg, 2018). 6 for 2017 recommended the individual consideration of ACS in discussion with the family in pregnancies over 200⁄7 weeks' gestation (American College of Obstetricians and Gynecologists & Society for Maternal-Fetal Medicine, 2017).
Genetic Factors
A 2015 Cochrane meta-analysis found a reduced incidence of RDS with repeated ACS treatment, but no benefits in mortality, IVH and NEC. In growth-restricted fetuses, questions remain about the benefit of ACS treatment (Torrance et al, 2009).
Other Antenatal Determinants
DELIVERY ROOM MANAGEMENT OF AT RISK NEONATES
Supplemental Oxygen During Resuscitation
CPAP as Initial Respiratory Support
Sustained Lung Inflation
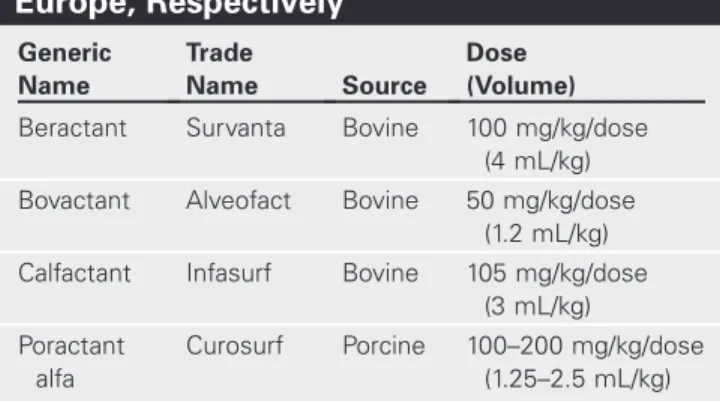
A number of animal-derived surfactants are available for use in preterm infants with RDS, partly differing in their composition (Table 11.7; . Sardesai et al, 2017; Singh et al, 2015). Some data indicate lower incidences of severe IVH in preterm infants treated with LISA compared with standard intubation and ventilation (Isayama et al, 2016; Kribs et al, 2015; Langhammer et al, 2018).
NICU MANAGEMENT OF AT-RISK NEONATES CASE 4
The procedure is embedded in a package of measures consisting of ACS, early CPAP and early caffeine treatment (Gopel et al, 2015; Mehler et al, 2012). During LISA, a fine and flexible catheter or feeding tube is inserted into the trachea of a premature infant who is breathing spontaneously on CPAP (Gopel et al, 2011; Kribs et al, 2015).
Mechanical Ventilation: Ventilator-Induced Lung Injury and Modes of Ventilation
Oxygen Toxicity
Infection and NEC
PHARMACOLOGIC THERAPIES FOR PREVENTION OF BPD
Noncorticosteroid Therapies
A meta-regression of RCTs showed that when the risk of BPD in the control population was less than about 33%, corticosteroids significantly increased the risk of death or CP (Doyle et al, 2014). A meta-analysis of data from all trials showed a reduction in risk for BPD and death or BPD with inhaled corticosteroid therapy (Shinwell et al, 2016).
There was no difference in the rate of neurodevelopmental impairment between groups at 18 to 22 months of corrected age (Bassler et al, 2018). Follow-up conducted up to 3 years of age found no difference in motor or cognitive function between the groups (Venkataraman et al, 2017).
LONG-TERM OUTCOMES CASE 6
Furthermore, available long-term follow-up studies raise concerns about impaired neurodevelopmental outcome (Sriram et al, 2018). The following section summarizes current data on long-term pulmonary and neurodevelopmental outcomes associated with BPD.
Pulmonary Outcome
This finding emphasizes that immaturity-related factors contribute to long-term pulmonary dysfunction with or without manifestation of BPD at 36 weeks PMA (Malleske et al, 2018). Exposure to adverse environmental factors, such as respiratory infections, tobacco and pollution, can impair the resolution of BPD and increase the risk of long-term lung disease (Davidson and Berkelhamer, 2017; McEvoy and Spindel, 2017; Morrow et al., 2017).
Neurodevelopmental Outcome