Barker, II, MD Afdeling Neurochirurgie, Massachusetts General Hospital, Harvard Medical School, Boston, MA, VS. Shih, MD Afdeling Radiotherapie, Massachusetts General Hospital Cancer Center, Harvard Medical School, Boston, MA, VS.
General Principles
Epidemiology and Risk Factors
Introduction
The two most common types of brain tumors are gliomas and meningiomas, which together account for approximately 70% of all primary brain tumors; this chapter will focus on the epidemiology of these tumors.
Gliomas
However, another study of human maternal exposure to N-nitroso drugs found no increased risk of childhood brain tumors [68]. With the exception of ionizing radiation, published studies have found no consistent association between putative risk factors and brain tumors.
Meningiomas
To date, data supporting the increased risk of meningioma among oral contraceptive users are limited, although current literature does indicate an increased risk of meningioma associated with the use of hormone replacement therapy. There was also a trend for an increased risk of meningioma in parous women compared to nulliparous women.
Conclusion
In addition, this group reported a novel association between meningioma risk and three variants in the gene encoding BRIP1, which is involved in the repair of DNA double-strand breaks by homologous recombination. Another gene found to be associated with meningioma risk is ataxia telangiectasia mutated, or ATM, which is also involved in homologous and non-homologous DNA break repair [114,141].
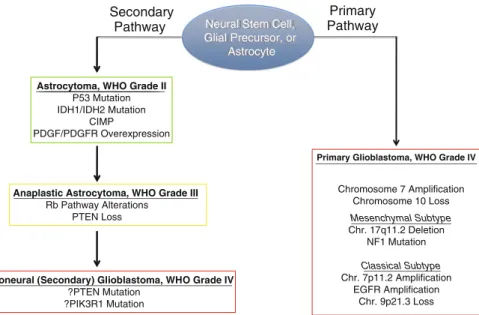
Molecular Pathogenesis
PDGF has also been implicated in the pathogenesis of low-grade astrocytoma in several ways. Important molecular changes associated with progression to anaplastic astrocytoma and ultimately secondary GBM include alterations in the Rb pathway and loss of portions of chromosome 10 and/or mutation of the PTEN tumor suppressor gene.
Cell of Origin and the Tumor Stem Cell Hypothesis Mouse Models
Recent developments have highlighted the potentially important role of a subpopulation of cells in a tumor called tumor stem cells in many tumors, including gliomas [85,86]. In some studies, these stem cells were defined by expression of the surface marker CD133 [89,90].
Cellular Origins of Malignant Glioma
The Cancer Stem Cell Polemic
After a transforming event, a stem cell (white) escapes one or more regulatory pathways, allowing it to proliferate uncontrollably (yellow). Additional stable epigenetic changes allow the cancer stem cell to generate partially differentiated daughter cells with a more limited potential for self-renewal.
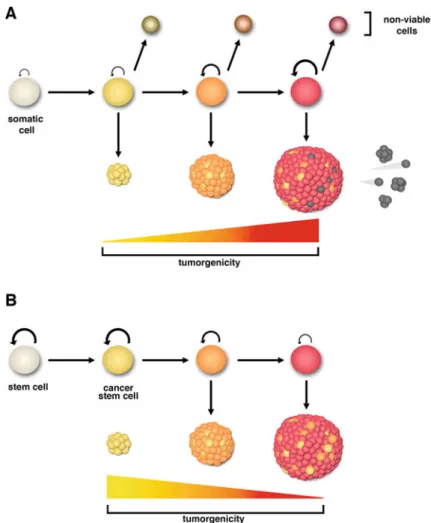
Glioma Stem Cells
Also consistent with the cancer stem cell hypothesis, CD133-positive glioma stem cells are selectively radioresistant [15]. CD133(+) and CD133(-) glioblastoma-derived cancer stem cells show different growth characteristics and molecular profiles.
Principles of Supportive Care
Cerebral Edema
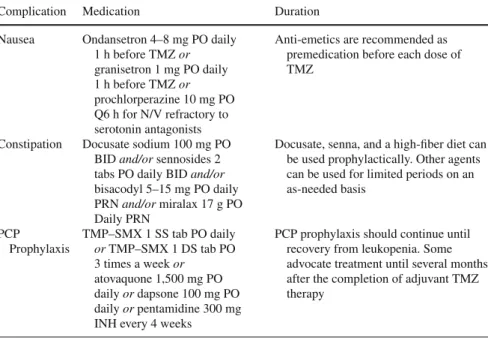
Although PJP is relatively rare in brain tumor patients, patients receiving corticosteroids or prolonged courses of daily temozolomide are at increased risk of developing PJP. All brain tumor patients receiving chronic steroids or prolonged daily courses of temozolomide should receive prophylactic therapy against PJP.
Seizures
The use of prophylactic anti-epileptic drugs (AEDs) in brain tumor patients is often based on the individual preferences of the treating physician rather than clinical evidence. Surgical treatment of brain tumor-related epilepsy is generally indicated only in patients with slow-growing tumors with a good prognosis.
Thromboembolic Complications Epidemiology and Pathophysiology
Prolonged use of LMWH as primary VTE prophylaxis in patients with newly diagnosed malignant glioma was evaluated in the PRODIGE trial [167]. To date, no randomized trials have directly compared LMWH with warfarin anticoagulation, particularly in patients with brain tumors.
Neurocognitive Symptoms
These drugs are generally well tolerated by brain tumor patients and may act as potentiators of antidepressants [203-206]. The norepinephrine-dopamine reuptake inhibitor bupropion is associated with lowering the seizure threshold and should be avoided in brain tumor patients.
Summary
Treatment of deep vein thrombosis and pulmonary embolism in patients with primary and metastatic brain tumors. Low molecular weight heparin versus a coumarin for prevention of recurrent venous thromboembolism in patients with cancer.
Principles of Clinical Trial Design and Response Assessment
Trials
Several articles address the need and complex design of Phase 0 studies in primary brain tumors [1]. These trials are similar to phase 0 pharmacologic endpoint studies, but they focus on the target tissue and the proposed mechanism of action of an agent.
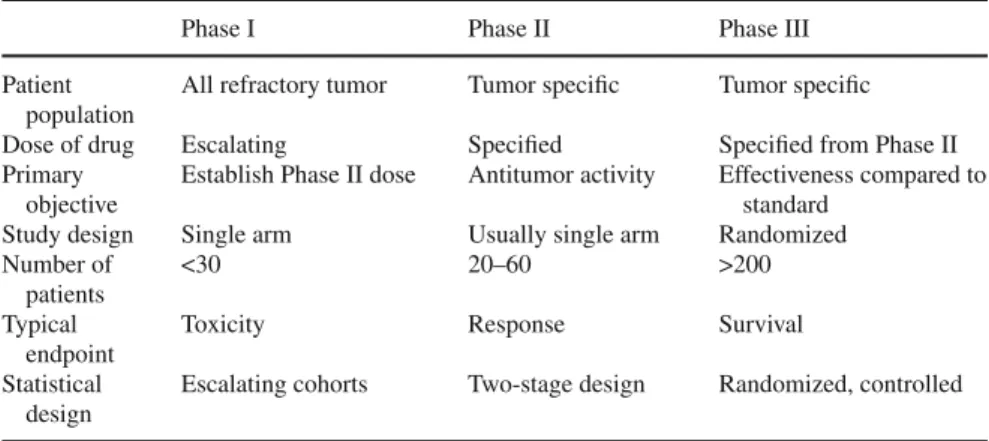
Trials Cytotoxic Agents
Although the goal of phase I trials of targeted agents remains to determine the recommended phase II dose, this dose is likely determined by biological endpoints and not necessarily by the MTD [16]. For example, a useful design may be to define the recommended phase II dose based on the MTD and the maximum target inhibition dose.
Trials Cytotoxic Agents
Another goal of phase II studies is to gain a more thorough understanding of the toxicity associated with the agent being tested. Such evaluation is even more important when considering that molecular agents may be given long-term and phase II studies may require evaluation of longer-term toxicity.
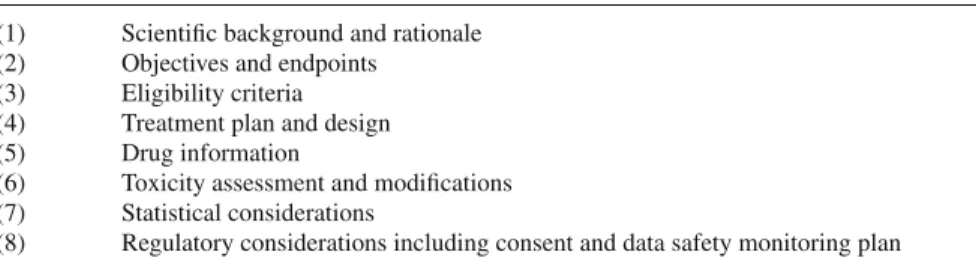
Clinical Trials
Special Challenges of Brain Tumor Trials
GNOSIS: guidelines for neuro-oncology: standards for investigational studies – reporting of phase 1 and phase 2 clinical trials. GNOSIS: guidelines for neuro-oncology: standards for investigational studies – reporting of surgically based therapeutic clinical trials.
Complications of Therapy
Pharmaceutical Therapy
In the past, CCNU (lomustine) was often used in combination with procarbazine and vincristine to create the regimen known as PCV, but this has largely been supplanted by BCNU or CCNU monotherapy after a retrospective review found no survival benefit for PCV compared to PCV. BCNU alone in the treatment of anaplastic astrocytoma [20]. Methotrexate is an antimetabolite and antifolate agent most commonly used by neuro-oncologists in the treatment of primary CNS lymphoma.
Complications After Radiation Therapy for CNS Neoplasms Introduction
Rare cases of severe CNS complications have been reported after administration of IT MTX, mainly in patients with severe disease that may disrupt CSF flow [93]. Intrathecal methotrexate is also frequently used in patients with hematological malignancies, as prophylaxis in patients without known CNS involvement [94] and as treatment in patients with CNS involvement [95].
Acute Toxicities Fatigue
In a retrospective review of pediatric and adult patients treated with CSI at Royal Marsden, Jefferies and colleagues reported a 33% rate of. The risk of hematological toxicity was found to be higher among the patients treated with electrons compared to photons and among patients younger than 6 years of age.
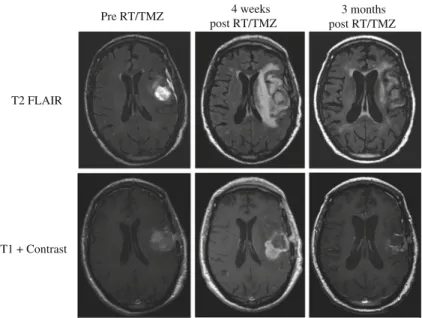
Subacute Toxicity Pseudoprogression
Surgical resection remains the gold standard for distinguishing treatment effect from true progression when indicated in the context of general patient care. It has been described in the context of multiple sclerosis, vitamin B12 deficiency, and head and neck injury [137].
Neurologic Late Toxicity
Neuropsychological Function and Quality of Life
Neurocognitive Function
Impact of the Tumor on Neurocognitive Function
Treatment Effects
Chronic radiation toxicity is also thought to involve changes in neurogenesis as well as metabolic abnormalities and inflammatory responses [20–23] . Neuropsychological studies of patients before and after radiation therapy document neurocognitive impairments consistent with frontal network dysfunction, including slowing, inattention, impaired executive function and memory, and a decrease in motor function, bilaterally, even in patients without evidence. of disease relapse [29].
Effects of Adjuvant Medications and Medical Complications
Steroids used to treat neurological and neurocognitive symptoms associated with peritumoral edema often have beneficial initial effects. Patients with seizures may become socially isolated because of the perceived stigma associated with having a seizure in a public area and/or around unfamiliar people.
Patient Care and Management
Glucocorticoid use is ubiquitous and associated with a 5-50% incidence of steroid-induced psychiatric syndromes, including euphoria, mania, insomnia, restlessness, and increased motor activity. The impact of steroids on neurocognitive function is variable and partly related to dose and chronicity of treatment, with higher doses and longer treatment duration associated with greater risks of neurocognitive and neurobehavioral disorders [33].
Neurocognitive Interventions and Pharmacotherapy
However, an important limitation of the study was the absence of a control group, and therefore a placebo effect or a practice effect due to repeated neuropsychological testing could have at least partially accounted for the improvement in cognitive function and symptoms. 64] conducted a randomized, placebo-controlled, double-blind study of the effects of d-methylphenidate on fatigue and cognitive dysfunction in women undergoing adjuvant chemotherapy for breast cancer.
Symptoms and Quality of Life in Brain Tumor Patients Overview of QOL and Symptoms
There are limited studies examining the impact of symptoms and HRQOL in patients with primary brain tumors. In patients with malignant gliomas, depressive symptoms have been shown to be associated with worse overall survival and HRQOL [122].
Overview of Common Symptoms Fatigue
Several additional risk factors for the development of depression have been identified in patients with cancer. In patients with brain tumors, the constellation of symptoms associated with increased intracranial pressure (headache, vomiting and decreased consciousness) and symptoms related to focal disturbances based on the location of the lesion is recognized and often used in clinical care [116].
Conclusions
Effect of disease burden on health-related quality of life in patients with malignant gliomas. Effect of neurological dysfunction on health-related quality of life in patients with high-grade glioma.
Low-Grade Gliomas
Epidemiology
For these tumor subtypes, approximately low-grade gliomas are diagnosed each year in the United States [2]. The incidence of oligoastrocytomas ranges from 1.8 brain tumors according to the Central Brain Tumor Registry to 9.2% in the Norwegian Cancer Registry [4, 8, 9].
Pathology and Pathogenesis
Low-grade oligodendrogliomas (WHO grade II) lack immunoexpression of nuclear p53 protein, an observation consistent with their low incidence of TP53 mutation [ 14 ]. Promoter methylation of the DNA repair gene MGMT has also been detected in about 50% of diffuse astrocytomas and is associated with TP53 mutations [25].
Clinical Presentations
IDH1 and IDH2 mutations are common in secondary glioblastomas but are rarely found in primary adult or pediatric glioblastomas [43,46]. IDH1 mutations are strongly correlated with TP53 mutations and 1p/19 codeletics and, in some cases, have been demonstrated to co-occur with these genetic abnormalities, suggesting that the combination of IDH1 mutation and either TP53 mutation or loss of heterozygosity of 1p/ 19q is the earliest common genetic abnormality identified in LGG [43,46].
Imaging
Dynamic contrast-enhanced perfusion MRI (DCE-MRI) is a research technique that can distinguish between low- and high-grade glial neoplasms. MR spectroscopy (MRS) can also help distinguish between low-grade and high-grade lesions.

Prognostic Factors
In an attempt to summarize these prognostic factors, a preoperative prognostic classification system has recently been developed. Although the latter three factors were previously identified as negative prognostic factors, location in the eloquent cortex was a novel prognostic marker.
Surgical Management
A recent publication reviewed ten studies published between 1990 and 2008 in which the extent of resection of LGG was evaluated in terms of the relationship with overall survival and progression-free survival [79]. In patients with 100% resection, 8-year overall survival was 98%, progression-free survival was 48%, and malignant progression-free survival was 79%.
Innovations in Surgical Management of Gliomas
All three of the volumetric studies and six of the seven non-volumetric studies reviewed showed a survival benefit relative to increased extent of resection. In a comparison of patients with LGG who were resected without (between 1985 and 1996) and with (between 1996 and 2003) intraoperative cortical stimulation, major neurologic deficits occurred at one-third the rate (6.5% vs. 17%) and MRI confirmed that total resection was more than four times more likely (25.4% vs. 6%) in the latter period.
Radiation Therapy