Weaknesses of the Japanese healthcare system include an inefficient primary care system and a lack of differentiation of healthcare providers and of standard clinical guidelines. Both the International Monetary Fund (IMF) and the Organization for Economic Co-operation and Development (OECD) have recently praised Japan's healthcare system. Part of the reason for these quotes is that Japan's healthcare spending is understated, which we will discuss in more detail in this report.
A lack of differentiation of health care providers and a lack of an efficient primary care system are weaknesses of the Japanese health care system. Unequal contributions are one of the most serious issues in the health care insurance system. Many of the problems facing the Japanese health care system today are due to the incompetence of the insurers.
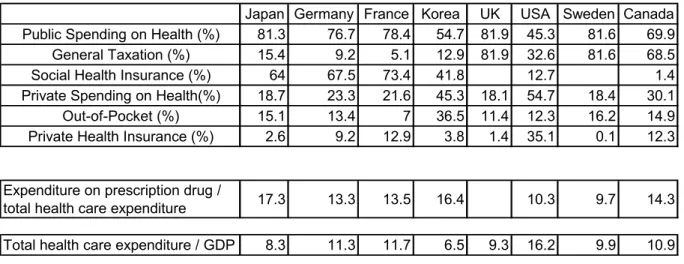
Each year, the OECD reports health care expenditure for each member country using the System of Health Accounts. However, due to the unavailability of data as described above, Japan's healthcare expenditure figures are underestimated. With this simple calculation, it is clear that Japan's national expenditure on health care is underestimated, by about one-third.
It is important that health policy is based on a solid understanding of the current reality.

Conclusion
For example, in 2007, national health care expenditure reported by the MHLW was ¥34.1 trillion, while total health care expenditure reported by the OECD was ¥41.9 trillion3. According to the Japanese National Accounts in 2007, economic activities in the health sector were £47.1 trillion. This number is the total of total government final consumption expenditures for the health sector (¥35.3 trillion) and household final consumption expenditures for the health sector (¥11.9 trillion)4.
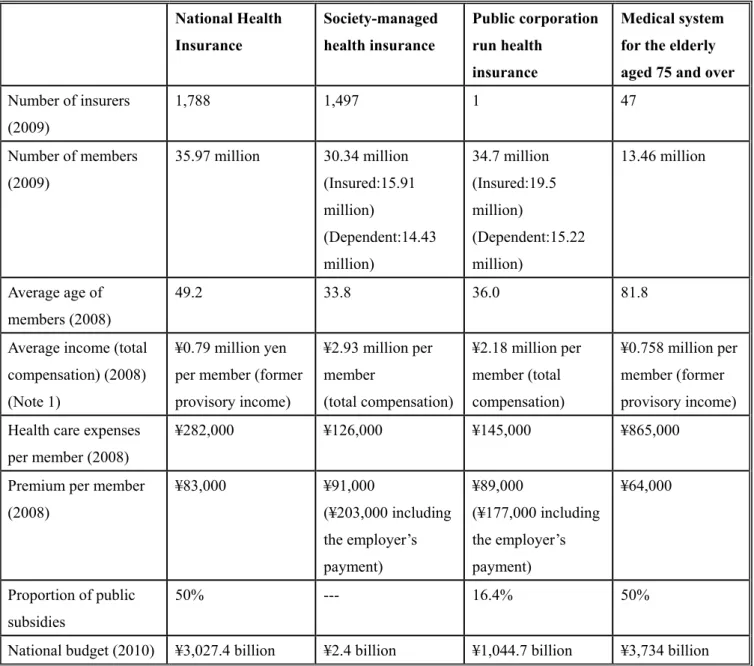
However, it is difficult to claim that health care policies to date have been formulated and implemented on the basis of solid, readily acceptable evidence. In order to move beyond the current situation, it is essential that the Japanese government takes responsibility for conducting statistical studies and making the resulting data public. corporation-based worker insurance, through pooled contributions from all the insurance schemes and tax revenue. About 50% is financed by government subsidy and about 40% from contributions from National Health Insurance and Employee Health Insurance.).
Among the many challenges for the Japanese health care system is the introduction of economic incentives to ensure quality and efficiency, especially in primary health care systems based on a solid database. Health care reforms focus on hospital reforms and seek to control hospital costs. Without an effective primary care system in place, our health system cannot be sustained in the face of this rapidly aging population.
Health System Reforms in the People’s Republic of China
Progress and Further Challenges Hiroko Uchimura ∗
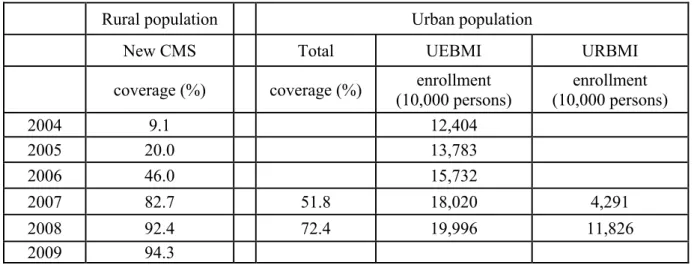
The difference in health systems between urban and rural areas has been one of the most critical features of China's health systems since before the economic reform. Along with the economic reforms that started in the late 1970s, socio-economic conditions have changed significantly in both urban and rural areas. The enrollment unit in the new CMS is a household, and all family members must enroll en masse in the new CMS.
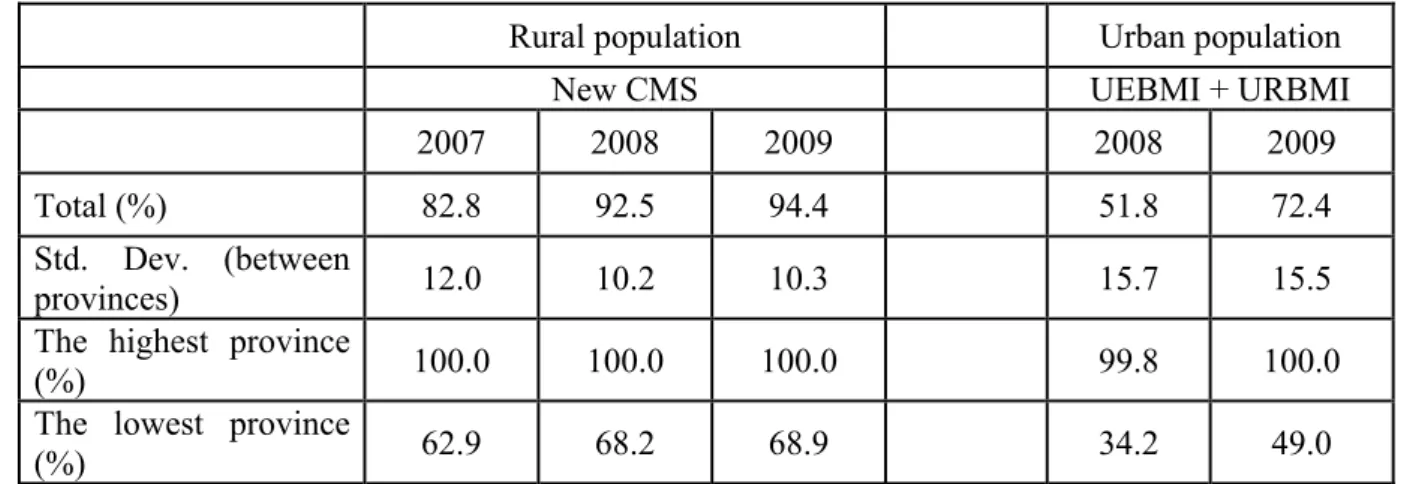
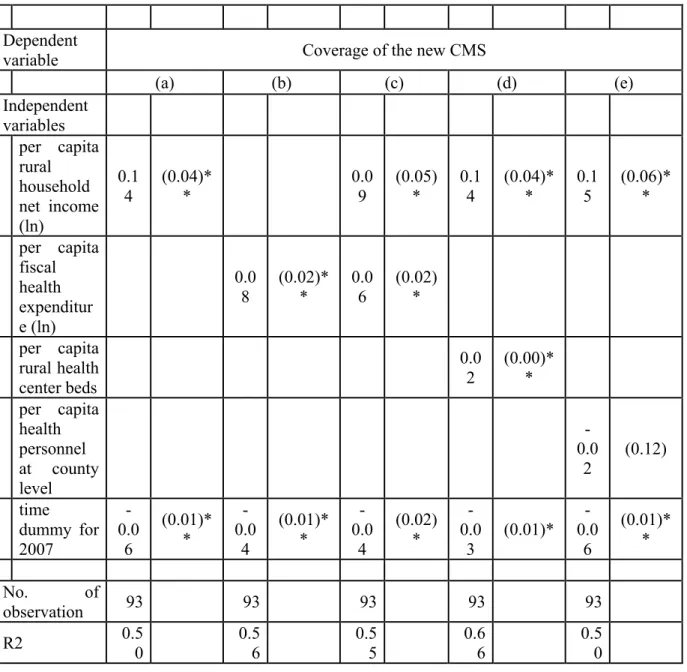
However, critical issues remain in the healthcare sector that prevent certain people from accessing necessary healthcare services. As we noted in the previous section, overall health insurance coverage has expanded significantly in both urban and rural areas; however, coverage varies between places. In addition, local health budget capacities can have an important effect on insurance coverage in China because local governments play an important role in the health care sector.
Local fiscal health expenditures used in the model are provincial health fiscal expenditures per capita. In addition, a time dummy for 2007 is included in the estimation model for the rural case. It suggests that the share of the working generation in the total population in China will reverse and decline in the near future.
These changes in the demographic structure may have a significant impact on the healthcare system in China. The ratio of the working population to the total population is expected to decline in the near future in China. Changes in the demographic structure of China will lead to further expansion of overall healthcare spending in the near future.
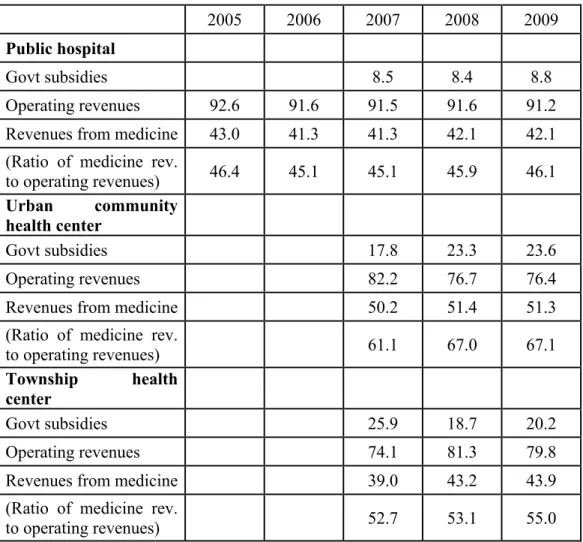
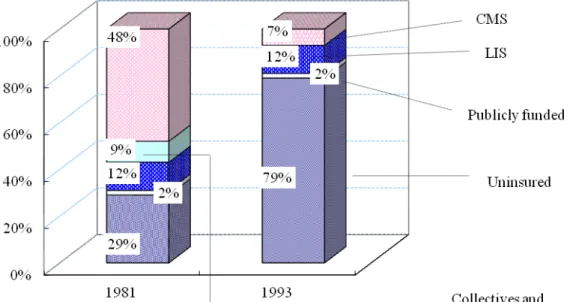
After the economic reforms started in the late 1970s, the conventional health systems decayed in both urban and rural China. The government did not pay much attention to the health sector in the 1980s and 1990s, which seriously prevented people from accessing necessary health services. In addition, aging will be a critical issue for the healthcare sector in the near future.
Further reforms of health insurance schemes will reduce the necessary fiscal subsidies for insurance funds that can be deployed for further challenges in the health sector. Public Expenditure in the Education and Health Sectors,” in Mei, Hong and Xioling Wong (eds.), China’s Budget System and the.
A Brief Review on Health Care Expenditure in the Past, Present, and Future in Japan
The figure shows the healthcare expenditure per person by age group with age intervals of five years. Health care expenditures per person increase steadily with age, and the increase accelerates after 50 years of age. The value for each group provides an unconditional average of health care expenditures and is therefore associated with two factors: total number of individuals who need care and how much each patient pays when he/she receives medical treatment or care.
At the same time, health care costs per patient increase with the age of a person due to greater chance of morbidity and disability for her/him. Thus, the health care expenditure of the nation is correlated with the demographic structure of the society through the two channels. Despite the accelerated aging of the population, as well as other factors known to be associated with high medical costs4, the Japanese healthcare system has managed to control national health expenditure at a fairly low level, especially compared to other OECD countries -countries.
The second reason is with the payment scheme in the Japanese health care system where fees for health services are centrally controlled to keep them uniform. The global revisions determine the basic health expenditure of the country, and the revision rates are associated with the economy of the country. However, if the second hypothesis is instead correct, the ratio of the patients will decrease.
Thus, projections of health expenditure at the macroeconomic level are often carried out in practice by using previously observed trends in socio-economic variables in a model. There has been increasing attention to the future of the health and health care system in Japan, and estimating the current national health expenditure and simulating the development of future health expenditure is of great concern to policy makers. In these analyses, healthcare costs per person often to increase over time.
The source of the increase in health care expenditures can be broken down into demographics (population size and structure), income, and other factors that can be explained by the residuals of the aforementioned two factors (such as advances in technology) (Horiuchi, 2011). We looked at the evolution of national health care spending in Japan and reviewed questions about forecasting future spending. Further studies are needed to better understand the mechanism of the association between population aging and health care expenditures.