Since 2010, the GBD has published age-specific mortality estimates for individual calendar years from 1950 onwards. Estimates of HIV-free U5MR and adult mortality are then used with a life table system model to generate age-specific HIV-free mortality rates.
Role of the funding source
Mean estimates and 95% uncertainty intervals (UIs; 25th and 975th estimates among the 1000 draws) were generated using the trait-level estimates. The estimated uncertainty of fertility and mortality estimates were useful inputs to the BCCMP model used in GBD 2019 to estimate the population.
Results Fertility
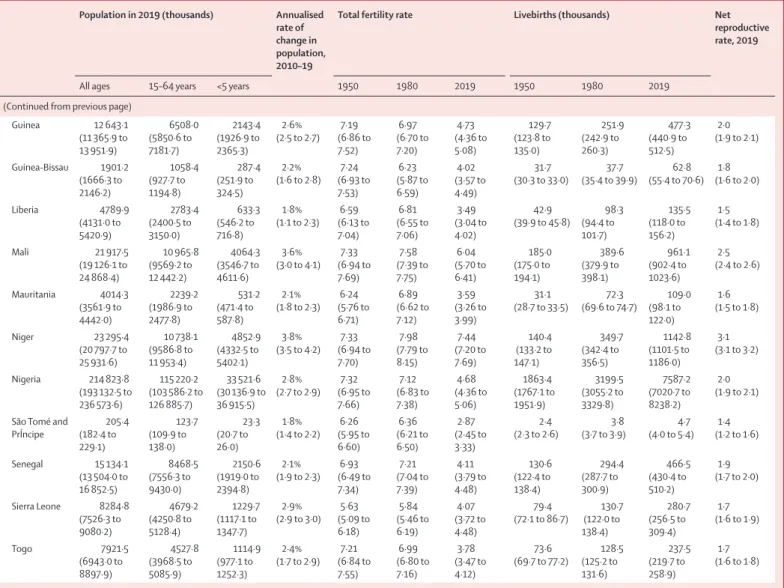
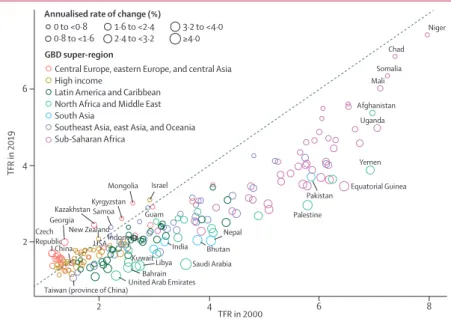
Saudi Arabia, Kuwait, Puerto Rico, Palestine, and Yemen experienced the fastest annual decline, at a rate of at least 3.6% per year. The decline in TFR has accelerated in most countries, with 128 (63%) experiencing a greater decline in 2010-19 compared to the previous decade. The result of these accelerated declines in fertility is that by 2019 half of all countries and territories (102 out of 204) had reached TFR below replacement level, with 43 of these having reached an ultra-low TFR of 1.5 or below.
In the last four decades, countries such as Belgium, the Czech Republic, Germany, Poland and Slovakia reached the lowest TFR in their history and then experienced increases in TFR. These increases are difficult to interpret because TFR, as a period measure of fertility level, is influenced by both levels of and changes in age-specific fertility rates of different maternal birth cohorts in that year. This includes all countries in sub-Saharan Africa and at least one country in every other superregion, such as Papua New Guinea, the Solomon Islands, Pakistan, Afghanistan, Yemen, Bolivia, Haiti, Israel, Tajikistan and Mongolia.
Mortality
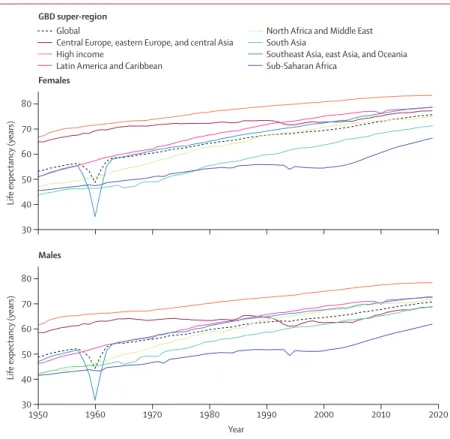
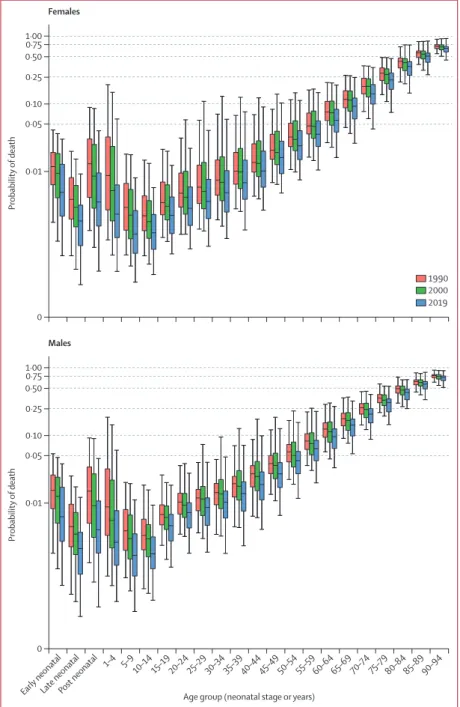
In five of the seven superregions, life expectancy at birth has steadily improved over the past seven decades (Figure 3). The annual change in under-5 deaths is defined as the simple difference between deaths in the under-5 age group in the current year and the previous year. Between 2000 and 2019, however, the width of the middle 95% decreased in the 20-24 and 70-74 age groups, while the width increased for the over-70-74 age groups for both sexes over the same time period . .
However, increases in the width of the total spread occurred between 1990 and 2000 in all age groups over 20 years. For age groups older than 75 years, the increase in the width of the middle 95% of the age-specific risk of death has been much more pronounced over the past three decades. While there have been improvements in survival across the age spectrum over the past seven decades, this is not universal.
Increases in mortality, especially among adult age groups, have been observed in countries that were hit hard by the HIV/AIDS epidemic in the 1990s and early 2000s. In recent years, similar increases in mortality have been seen among young adult age groups in the United States, Sweden, Great Britain, Norway, New Zealand, Malta, Israel, Iceland, Greece, Brunei, Belgium and Argentina.
HALE
Fatal disruptions due to events such as civil conflicts and natural disasters have also led to sharp increases in mortality.
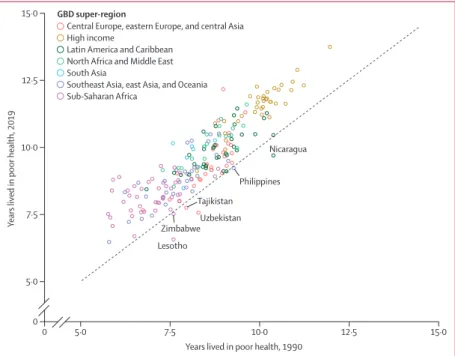
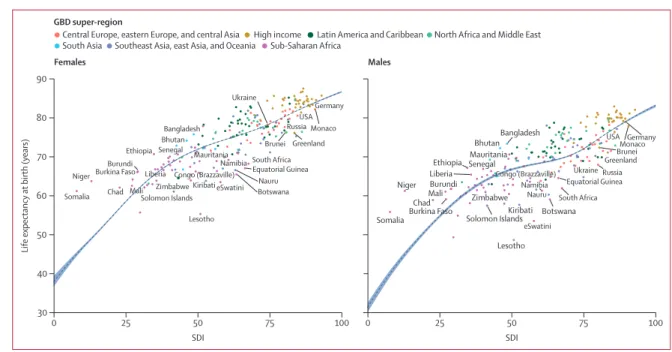
Observed versus expected life expectancy based on SDI Figure 6 shows for each country in 2019 the observed life
The five countries in this superregion that had male life expectancy at birth lower than expected are Brunei. For sub-Saharan Africa, 18 (39%) of 46 countries had male life expectancy at birth higher than the expected value based on SDI. The high-income GBD superregion also had the most countries proportionally (80·6%) and in absolute terms (n=29) with higher female life expectancy at birth than expected based on SDI.
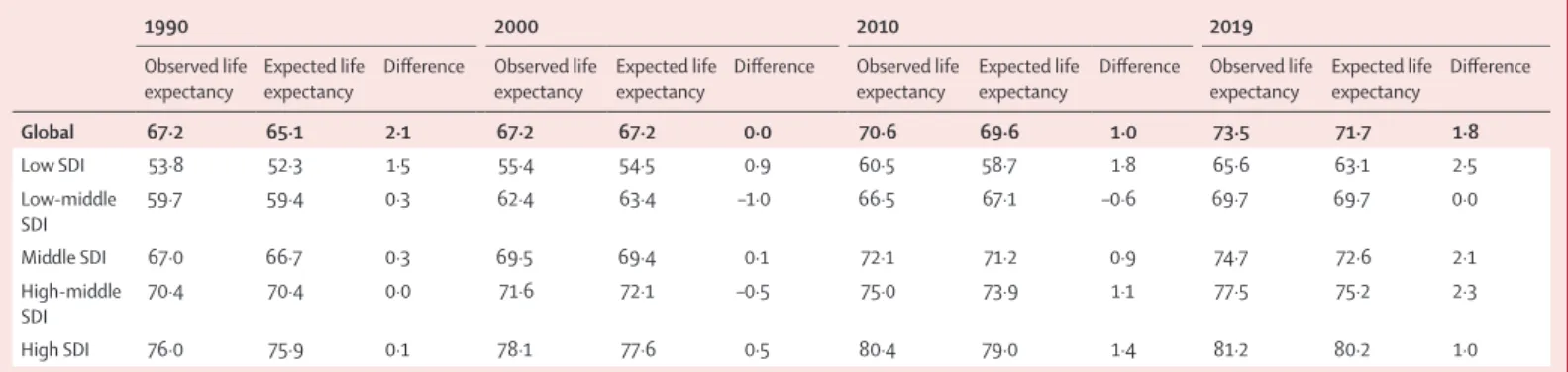
Between 1950 and 1980 there was a general improvement in the average difference between observed and expected life expectancy at birth for both sexes combined (Figure 7). Such a trend is visible when we examine the observed versus expected life expectancy at birth by SDI quintiles (Table 3). For 2019, for example, the difference between observed and expected life expectancy at birth is positive across all SDI quintiles.
Population
Demographic transition
Data points show the difference between observed life expectancy and expected life expectancy at birth based on HDI by country or territory for every tenth year between 1950 and 2010 and for 2019. Southeast Asia, East Asia and Oceania Sub-Saharan Africa Figure 6 : Life expectancy at birth and adjusted life expectancy based on SDI, 2019. The scatterplot shows estimated life expectancy at birth in years for 204 countries and territories colored by super-region for 2019.
The dashed black line represents the life span predicted based on the SDI, with 95% confidence intervals shaded. In 1970, 94 countries were in late transition: 46 with net emigration and 48 with net emigration. In 2019, 131 countries were in late transition, 81 of which had net emigration and 50 net emigration.
Discussion Main findings
Global population health improvement
Implications for future progress
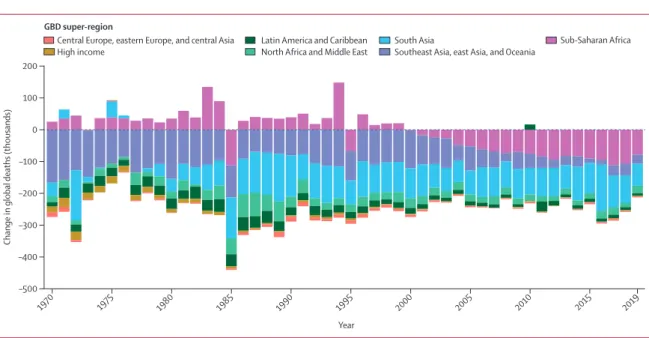
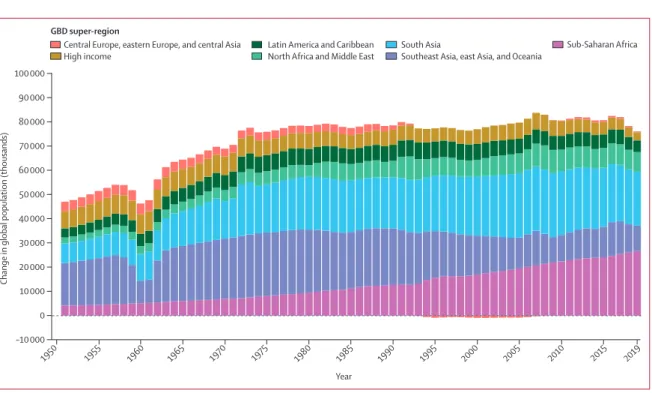
The proportion of under-5 deaths globally occurring in sub-Saharan Africa has increased steadily in recent decades (figure 2). This shift towards contributing a higher proportion of global under-5 deaths, combined with the region's higher TFR compared to other regions, indicates that the pace of improvement in reducing under-5 deaths globally has and will suffer further slowdowns due to compositional shifts. For example, trends in fertility rates will have a significant impact on future global population size, which will have potentially large carbon consequences.
Reversals in the global improvement in mortality have been observed in countries across the SDI spectrum. In the 1990s, countries in East and Southern Africa, Eastern Europe and Central Asia experienced increases in mortality (appendix 2 table S3A). In the past two decades, some countries in the high-income superregion have seen increases in the probability of death in mature age groups.
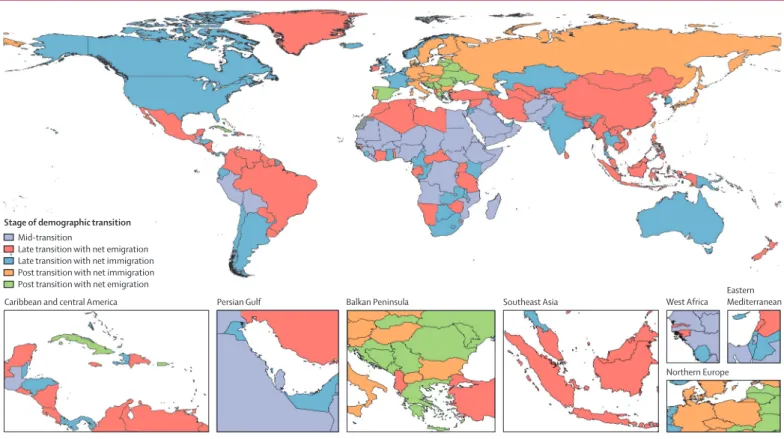
Stages of demographic transition
In these places, socio-economic, political and religious influences on both fertility and mortality have contributed to demographic profiles that are quite different from the post-transition group.49,50 The presence of the 102 countries and territories where TFR is above replacement level in the mid-transition - and late-transition groups under scores the persistence of above-replacement-level fertility together with a delay in the realization of the lowest observed mortality. Yet it is far from certain that fertility will increase or converge in the long term. Cohort-completed fertility by age 50 years (CCF50) is a much better measure than TFR of the true level of fertility, because the measurement of fertility by birth cohort controls for general shifts in the timing of fertility.
The strong relationship between fertility behavior, socioeconomic indicators of education, and fulfilled need for contraceptives also suggests that fertility is unlikely to recover and converge to replacement levels in the long run. Since it is influenced by both the sex ratio at birth and the death rate, the replacement level fertility varies over time and by location. Based on our current estimates of fertility, mortality and sex ratio at birth, replacement level fertility in 2019 ranged from 2·05 to 2·44.
Comparisons between GBD demographic estimates and other demographic estimates
Since the 1940 birth cohort, the CCF50 has peaked and begun to decline in all countries and territories (1969 represents the last birth cohort for which we have complete age-specific fertility data between 15 and 50 years). The replacement level fertility is realized when the net reproduction rate is 1.0, which means that a female gives birth to one daughter if she is subject to the current age pattern of mortality and fertility.
Limitations
A standalone migration model that estimates age-specific and sex-specific immigration and emigration is needed to have more consistent estimates of all major components of the demographic equilibrium equation: fertility, mortality, migration, and population. The paucity of census data in certain locations and the delay between censuses affected our completeness estimate for vital and sample registration systems, and for the recall of household deaths in census and surveys. The mortality analysis for the adult age groups at sites without a vital registration system relied heavily on indirect estimates of adult mortality based on sibling survival data, recall of household deaths from censuses and surveys, and covariates in low data periods.
The availability and quality of migration data is generally poor compared to data on mortality and fertility. There may be overdispersion in some of the data we used, leading to inaccurate estimates of data variance. Since the sampling errors in the mortality and fertility data we used from vital registration and civil registration systems are likely to be much smaller than the non-sampling errors, we do not expect such a change to have a significant impact on our estimates.
Future directions
Third, this study faced a number of limitations due to the availability of high-quality data or the use of lower-quality data. In locations where these systems do not exist, nationally representative sample registration or disease surveillance systems should be established. This is true even for high-income countries, which generally keep more accurate accounts of immigration, although this is less true of emigration.
When migration data are collected, questionnaires tend to be non-standard, which makes it difficult to compare and integrate information on migration from different sources. This is particularly a problem for low HDI countries, which are both the source and destination of most migration in recent years. As the most influential international survey, only about 25% of all demographic and health surveys include any questions that can be used to elicit information on migration.
Conclusion
S James reports grants from Sanofi Pasteur and employment from Genentech, outside of the submitted work. V Jha reports grants from Baxter Healthcare, GlaxoSmithKline, Zydus Cadilla and Biocon, and personal fees from NephroPlus, outside of the submitted work. J Mosser reports grants from the Bill & Melinda Gates Foundation, during the conduct of the study.
S Nomura reports grants from the Ministry of Education, Culture, Sports, Science and Technology, both during the conduct of the research and outside the submitted work. T Pilgrim reports grants and personal allowances from Biotronik and from Boston Scientific, and grants from Edwards Lifesciences, outside of the submitted work. A Thrift reports grants from National Health and Medical Research Council Australia, outside of submitted work.