ADI Addis Statement on Immunization ASSAf Academy of Sciences of South Africa BCG Bacillus Calmette-Guérin Vaccine. The Academy of Sciences of South Africa (ASSAf) together with the Uganda National Academy of Sciences (UNAS) led the research.
Despite the global availability of proven efficacious and cost-effective vaccines for the past several decades, vaccine-preventable diseases
PROBLEM STATEMENT
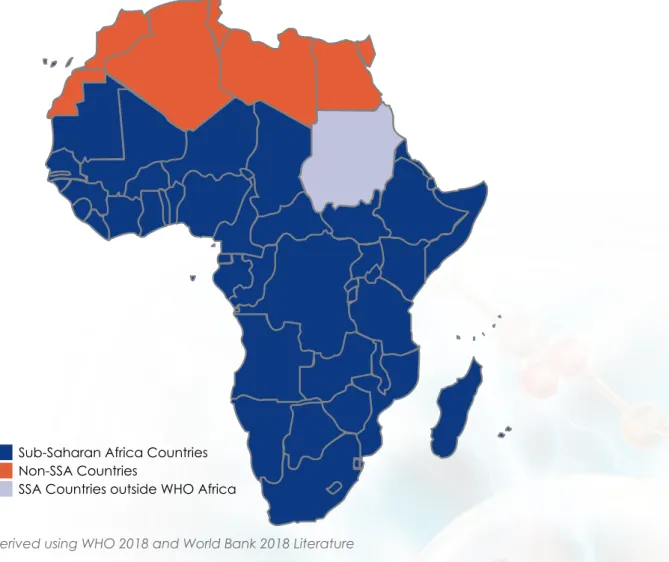
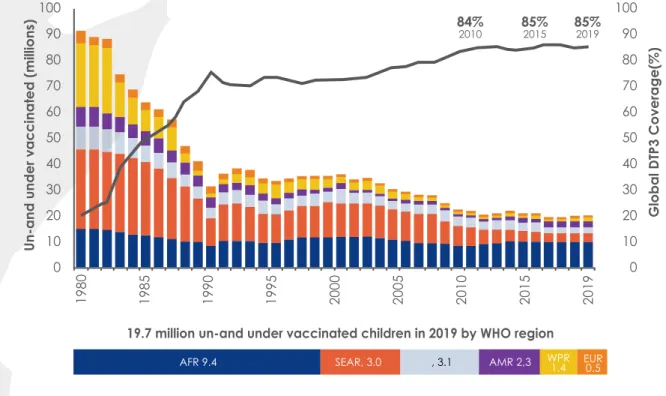
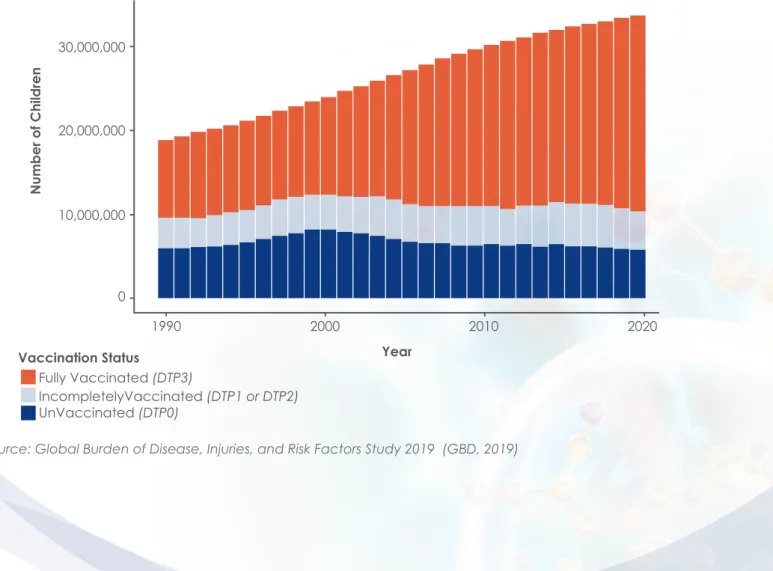
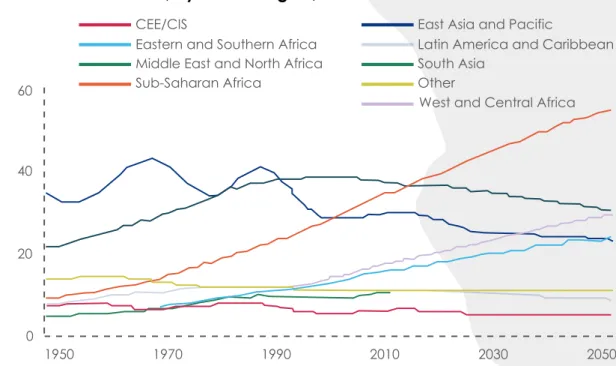
According to WHO, the Africa Region 1 accounted for approximately 43% of unimmunised and incompletely immunised infants in the world
SUMMARY AND
RECOMMENDATIONS
Confidence in the overall health care system directly affects confidence in the vaccination program in SSA. Political and socio-economic leaders should be aware in their actions of the sensitivity of the vaccination program to public trust in the health care system.
REPORT OUTLINE
CONCISE
- Study objectives
- Study methodology
- Study design
- SUB-SAHARAN AFRICA IN
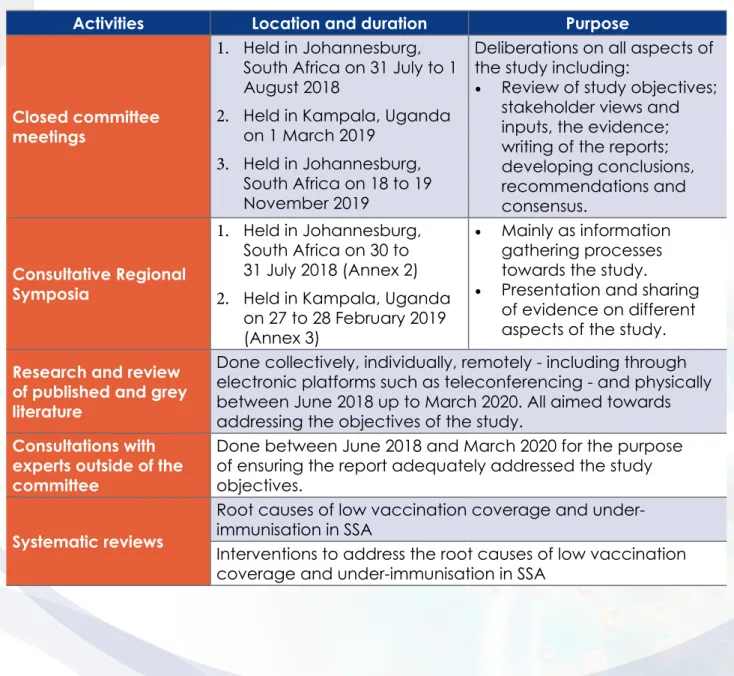
The research proposal (approved by the councils of both academies) outlined a combination of methodologies aimed at ensuring that the research objectives produced responses that: (i) are evidence-based, (ii) include local experiences and relevance (with examples of innovation), and (iii) provide contextualized and implementable recommendations. Conducted between June 2018 and March 2020 to ensure that the report adequately addresses the research objectives.
PERSPECTIVE
- Socio-demographic context
- Immunisation policy context and outlook
- Immunisation development agenda and timing of cycles
- Outlook for immunisation in Africa
- Unvaccinated and under-vaccinated children in SSA
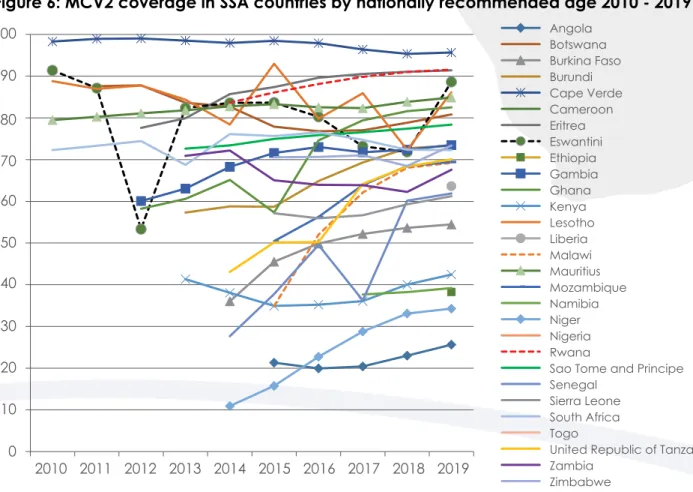
- Second dose of measles containing vaccine (MCV2) coverage
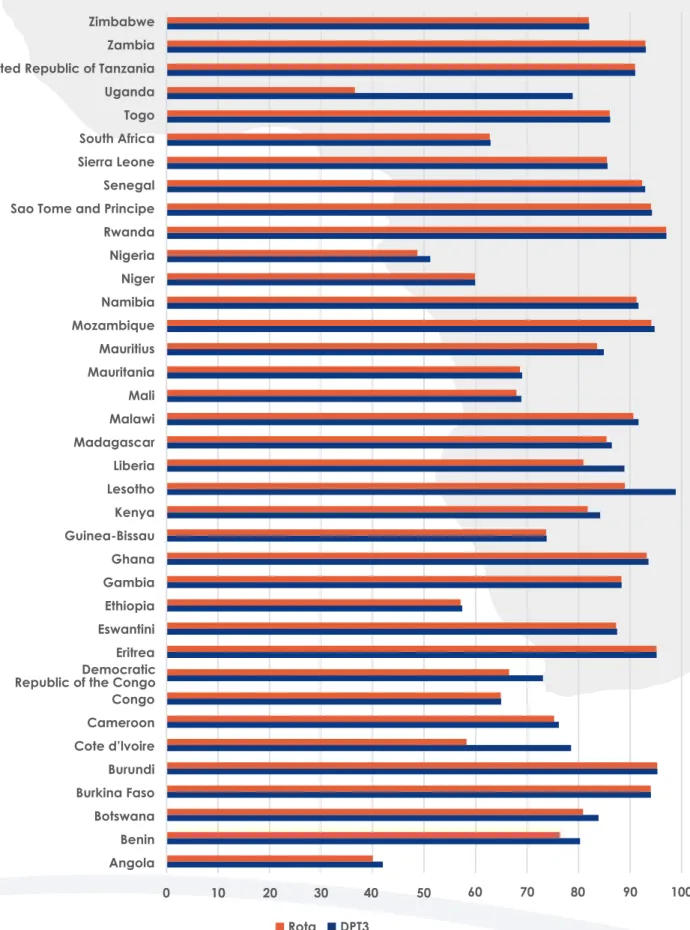
- Rotavirus vaccination coverage
- Introduction
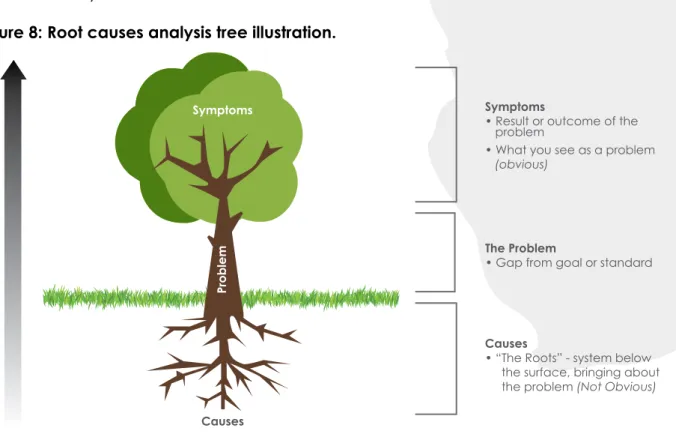
- Root cause analysis
- Theory of change
- ROOT CAUSE OF
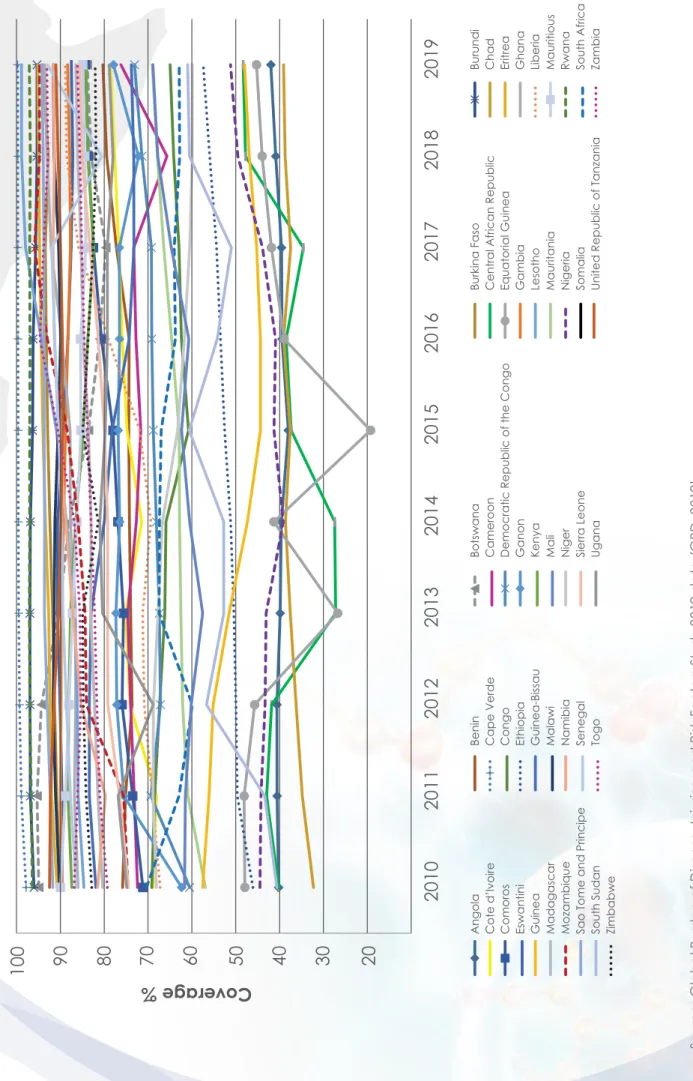
The Global Vaccine Action Plan (GVAP) target was at least 90% DTP3 coverage nationally and at least 80% coverage in each district by 2020 (World Health Organization, 2013). Of the five countries that account for more than 50% of all rotavirus deaths worldwide, three (Nigeria, DR Congo and Angola) are in SSA (Steel et al., 2019).
LOW VACCINATION COVERAGE
Knowledge - deficiencies and inaccuracies
- Demand-side knowledge deficiencies and inaccuracies
- Supply-side knowledge deficiencies and inaccuracies
- Interventions to address knowledge deficiencies and inaccuracies
- Conclusions on knowledge deficiencies and inaccuracies as a root cause for low coverage and under-immunisation
- Recommendations on knowledge deficiencies and inaccuracies as a root cause for low coverage and under-immunisation
On the demand side, a systematic review of barriers to childhood immunization in SSA found that parental lack of knowledge about immunization was the most frequently and consistently reported barrier to childhood immunization (Bangura, et al., 2020), (Wiysonge, Uthman, Ndumbe, & Hussey, 2012). Braka, et al., 2012) also concluded through focus group discussions in Uganda that a general lack of information among caregivers about the benefits of immunization, concerns about the safety of immunization and misconceptions were the reasons for not taking children for immunization . However, (Bangura, et al., 2020), in their systematic review of barriers to immunization in SSA, found reports where healthcare providers lacked knowledge of vaccine indications and contraindications as well as counseling skills.
Oku, et al., 2017) reported that in some health facilities in Nigeria, caregivers said that most of the information they received from health workers in clinics focused on other child health strategies (nutrition, child care , personal hygiene) and reported missing information. vaccination information. Malande et al., 2019) attributed the lack of knowledge of health workers to a lack of adequate training. Wallace, et al., 2017) had similar findings in Nigeria, where only 55% of health workers interviewed were aware of the multi-dose vial policy to reduce vaccine wastage.
Ames, et al., 2017) reiterated the fact that how and by whom communication is done matters. Oku, et al., 2017) recommended that training of health workers should strongly address interpersonal communication skills, so that health workers can maximize any opportunities for strengthening on immunization and child health more generally.
Trust – relationships and allegiances
Rwanda, which has maintained one of the highest vaccination rates in SSA, uses two mobile health (mHealth) technologies, namely the RapidSMS and the mUbuzima applications (World Health Organization, 2013). RapidSMS is a text messaging tool used by community health workers to routinely monitor health events during pregnancy, childbirth, and a woman's first year of life. Because the vaccination rate in Rwanda was already very high when the impact of RapidSMS was evaluated, there is a 'ceiling effect'.
However, both tools are believed to have contributed to maintaining high vaccination rates in the country. MomConnect is a free mobile information and messaging service that is a project of the National Department of Health. This service supports maternal and child health by integrating mHealth technology into maternal and child health services, from pregnancy to the child's first birthday.
One of the objectives of the service is to deliver targeted health promotion messages to pregnant women to improve their health and that of their babies, and this includes vaccinations (Department of Health, Republic of South Africa, 2019).
Text Box 1: Country experiences of mHealth for Immunisation
- Demand-side trust issues
- Supply-side trust issues
- Interventions to build trust in immunisation programmes
- Conclusions on trust
- Recommendations on trust
- Convenience – access and reliability
- Demand-side convenience issues
- Supply-side convenience issues
- Interventions to improve convenience
- Conclusions on convenience
- Recommendations on convenience
- Political ownership – financing, community ownership, and enabling environment
- Immunisation financing
- Community ownership
Vaccine acceptance involves multiple levels of trust: trust in the product (the vaccine), the provider (specific health care professionals or administrative staff involved in providing and administering vaccinations), and trust in policy makers (the health care system, government, public health). researchers involved in approving and recommending the vaccine) (Larson, et al., 2018). A systematic review conducted by (Larson, et al., 2018), which looked at the impact of interventions used to gain confidence in the immunization program, found no literature from SSA on this topic. Tefera, et al., 2018) found that housewives had children with higher coverage of full immunization status (63%) than certain other occupations, such as merchants (51%) or public/private workers (56%), while mothers of incomplete vaccinated children cite lack of time as one of the reasons.
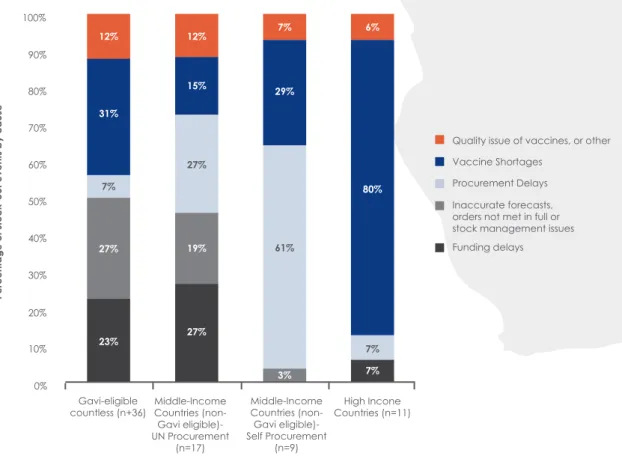
A study (Mbegue, et al., 2017) conducted in Senegal pointed out that one of the reasons for low vaccination rates is the logistical challenges of moving vaccines between regions. (Adamu et al., 2019) cited loss of vaccines as a cause of insufficient availability of vaccines in health facilities, resulting in missed opportunities for vaccination. Chadambuka, et al., 2012) attributed these health workers' vaccination challenges to inexperience, lack of sufficient training and work overload.
A systematic review by (Oyo-Ita, et al., 2016) also found that home visits by these cadres of workers can also increase childhood vaccination coverage in LMICs. Task shifting has also been used in cold chain maintenance, a specialist area chronically short of skilled workers in SSA (Bangura, et al., 2020). Similarly, Bangura et al.'s (2020) systematic review found that financial constraint was a major barrier impeding childhood vaccination in SSA.
Kamara, et al., 2008) reviewed financial sustainability plans (FSPs) of several low-income Gavi-supported countries, including twenty-seven countries in the WHO African region, and found that country strategies generally fell into three categories : (1 ) mobilizing additional resources, (2) increasing the reliability of resources, and (3) improving program effectiveness.
Coordination and surveillance
Hold governments accountable for delivering the vaccination services their entire populations need, especially the poorest and most marginalized members of society. Elevate the voices of communities by supporting and empowering them to participate in immunization processes and accountability mechanisms. Hold donor governments and multilateral institutions accountable for delivering on the commitments they have made to provide financing and support for immunization and ensuring this is aligned with national health plans and priorities.
Catholic Relief Services, 2019) provided documentation of OCD activities in SSA, showing that they contributed significantly to increasing immunization uptake in the region.
Social behaviour change
In Togo and Madagascar, civil society organizations used father role models to raise immunization awareness, serving as advocates and role models in their communities, while vaccination advocates were used in Guinea to address myths about infertility among vaccinated Wahhabi women, resulting in nearly 100 children from hesitant families. vaccination against polio.
Stronger community level systems and services
Advocacy
- Enabling environment
- Armed conflicts, humanitarian emergencies, and immunisation
- Immunisation in pandemic situations
- Conclusions on Political Ownership
- Recommendations on political ownership
- Overarching conclusions and recommendations
Grundy & Biggs, 2019) also found that low immunization coverage and VPD outbreaks are of great concern in conflict-affected countries, particularly in the sub-regions most affected by conflict. In Cameroon, attacks on medical facilities and health workers were recorded in the conflict in the north-west and south-west regions of the country. In the Central African Republic, the use of 'low-tech' vaccination systems has been used with success.
Furthermore, in the face of potential supply shortages, the use of fractional-dose vaccines in these settings may be key to improving coverage (Nnandi, et al., 2017). Peyraud, et al., 2018) report that in a chronic humanitarian emergency in the Central African Republic, preventive multi-antigen vaccination campaigns resulted in a significant and rapid increase in vaccine coverage after three rounds of vaccination. In the Lake Chad region, efforts have been made to integrate nutritional assessments and interventions with polio vaccination (Nnandi, et al., 2017).
Disease pandemics disrupt healthcare provision and can lead to a decline in vaccination rates, as evidenced by Liberia and Guinea, where there was a sharp decline of more than 25% in the monthly number of children diagnosed with measles in 2014 due to an Ebola outbreak. was vaccinated. and 2015 compared to previous years (Masresha B.G., et al., 2020). & Wiysonge, 2020), using a causal approach, have demonstrated the multifaceted impact of increased COVID-19 infections on immunization in Africa, showing that there would be a reduction in the number of health workers available to provide routine immunization services while she would be deployed for tasks related to COVID-19.
Accessed from: https://www.ilo.org/africa/media-centre/pr/WCMS_444474/lang- -en/index.htm. Report of the Committee on Securing Land Ownership of Africa's Development Agenda in the Post-2015 Era." Kampala. Accessed from: https://blogs.unicef.org/blog/getting-children-immunized-going-the-extra-mile-in-car/.
Accessible via: https://www.unicef.org/eca/press-releases/new-funding-will-allow-countries-secure-sustainable-vaccine-supplies-and-reach. Accessible from: https://data.worldbank.org/indicator/SP.DYN.LE00.IN?locations=ZG World Health Organization.
ANNEXURES
List of committee members with short biographies
- Prof Shabir Madhi (South Africa), Co-chair
- Prof Harriet Mayanja-Kizza (Uganda), Co-Chair
- Prof Richard Adegbola (Nigeria)
- Dr Juliet Kiguli (Uganda)
- Dr Annet Kisakye (Uganda)
- Prof Sileshi Lulseged Desta (Ethiopia)
- Dr Helene Mambu-Ma-Disu (Democratic Republic of Congo)
- Prof Jeffrey Mphahlele (South Africa)
- Ms Diana Kizza Mugenzi (Uganda)
- Prof Helen Rees (South Africa)
- Prof Charles Shey Wiysonge (Cameroon and South Africa)
He previously served as Head of the Department of Pediatrics and Child Health and Director of Clinical Epidemiology Service at Addis Ababa University. She served as a regional advisor for the WHO Africa Regional Office and was a WHO Resident Representative in several countries in the region, before retiring in 2008. He is also the former head of the department of virology, former co-director of the SAMRC's research unit on diarrheal pathogens and co-founder of the South African Vaccination and Immunization Center (SAVIC) at Sefako Makgatho Health Sciences University.
He is a member of the National Advisory Group on Immunization (NAGI) as well as a member of the Academy of Science of South Africa (MASSAf). Prof Rees is the founder and Executive Director of the Wits Reproductive Health and HIV Institute (WRHI), South Africa. Prof Charles Shey Wiysonge is the Director of the South African Cochrane Center at the SAMRC and a professor at both Stellenbosch University and the University of Cape Town in South Africa.
He is a former member of the WHO Strategic Advisory Group of Experts on Immunization and the Gavi Independent Review Committee. He is a member of the WHO working group on measuring behavior and social drivers of vaccination and a member of the Academy of Sciences of South Africa (MASSAf).
Symposium Programme (South Africa, 30-31 July 2018) Root Causes of Low Coverage and Under-Immunisation in
DAY ONE: 30 JULY 2018
DAY TWO: 31 JULY 2018
Business Engagement
Symposium Programme (Uganda, 27-28 February 2019) DAY ONE: 27 February 2019
Session Five: Stakeholder's talking point - Create solutions together Moderator: Jeffrey Mphahlele, Medical Research Council (South Africa BREAK.
Root Causes of
Low Vaccination Coverage and Under-Immunisation
A Consensus Study Report