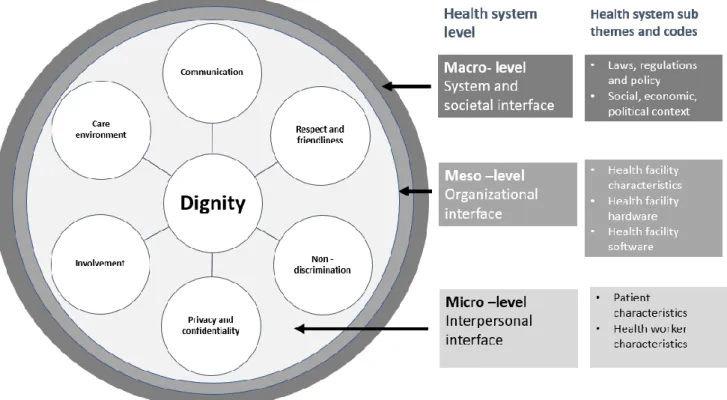
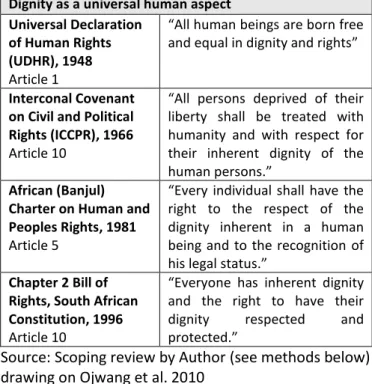
Meso-level Organizational interface representing local health systems, organizations and health facilities (Sheikh et al. 2011; Gilson 2012). Micro level Interpersonal interface representing individual actors and interactions between the two actors in the health system (Sheikh et al. 2011; Gilson 2012). According to many of these policies and protocols, dignity must be granted to each individual (see Table 1)1 (Ojwang et al. 2010).
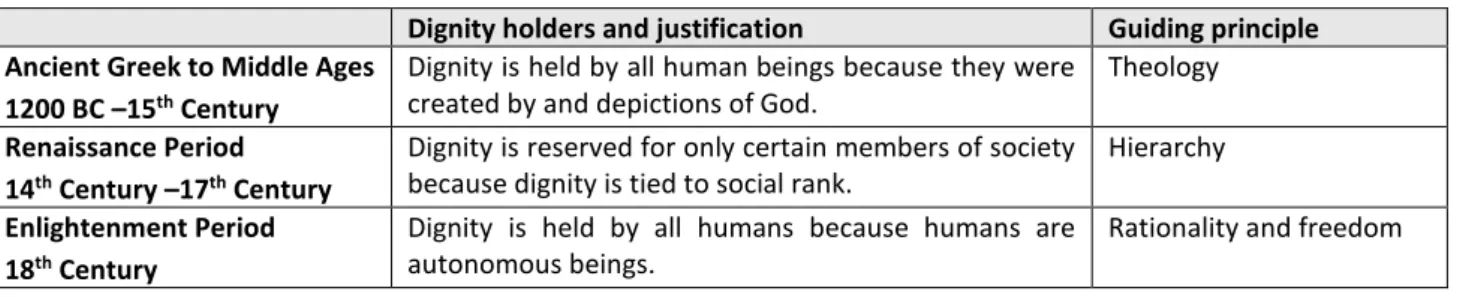
London et al. 2014) and in the pursuit of universal health coverage (UHC), the provision of quality services to all patients, including the most vulnerable, remains paramount (Ghebreyesus 2017). Although there is a consensus that today dignity is guaranteed to all people (Gostin et al. 2003; Jacobson 2007; Forms of indecent care (Ijadunola et al. 2019) In-depth interviews on the perception of dignity s.
13 dignity in the healthcare system includes dignified communication between clinical and non-clinical staff (Darby et al. When patients participate in decision-making, they feel dignified (Green and Baston 2003; Hosseini et al. 2018). While most of the six dignity themes were related to interpersonal cooperation with a healthcare professional (Kruk et al. 2014; Okafor et al.
24 Appendix 2 describes Banks et al. 2017) criteria used for measuring observable forms of non-dignified care.
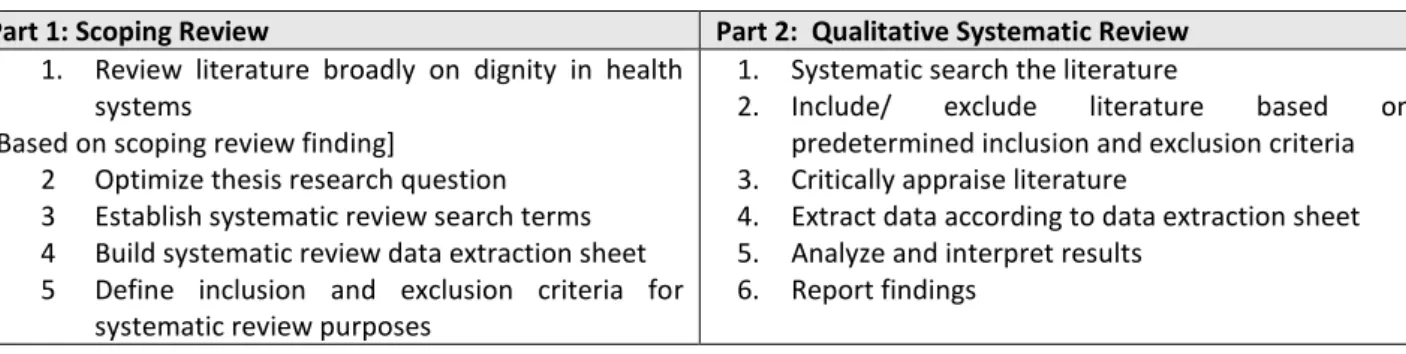
Qualitative systematic review
An extensive, unbiased search is one of the fundamental differences between a traditional narrative review and a systematic review” (Tranfield et al. 2003, p. 215). An overview of the key processes involved in this two-part qualitative systematic review study is described in Table 8. A qualitative systematic review was chosen due to the complex nature of dignity in healthcare systems.
As indicated in Table 8 above, the qualitative systematic review (Part 2) will begin with an electronic systematic literature search focusing on dignity in sub-Saharan African health systems. First, we will carefully record and present each step of the systematic review process in both the protocol and the final thesis (Dixon-Woods et al. 2006). As described above, the use of criteria assessment tools and a data extraction sheet will further support a rigorous systematic review (Tranfield et al. 2003; Dixon-Woods et al. 2006).
As a result, it could appear that this systematic review weakly considers facilitators of dignity in sub-Saharan health systems, when in fact such findings are characteristic of the wider evidence base. Second, due to budgetary constraints, only articles written in English will be considered in this systematic review.
Scoping review
Despite the potential for an uneven distribution of results, a systematic review closely identifying health systems' barriers to dignity will still provide important lessons for policy recommendations. A guide to writing a qualitative systematic review protocol to improve evidence-based practice in nursing and health care. Caring for the human spirit and the role of dignity therapy: a systematic review of dignity therapy research.
Disrespect and abuse of women during the childbirth process in healthcare facilities in sub-Saharan Africa: a systematic review and meta-analysis. Mannava P, Durrant K, Fisher J, Chersich M, Luchters S. Attitudes and behaviors of maternal care providers in interactions with clients: a systematic review. Role and outcomes of community health workers in HIV care in sub-Saharan Africa: a systematic review.
Barriers and facilitators to the integration of mental health care in primary health care: a systematic review. Effects of dignity therapy on dignity, psychological well-being and quality of life in cancer patients in palliative care: a systematic review and meta-analysis.

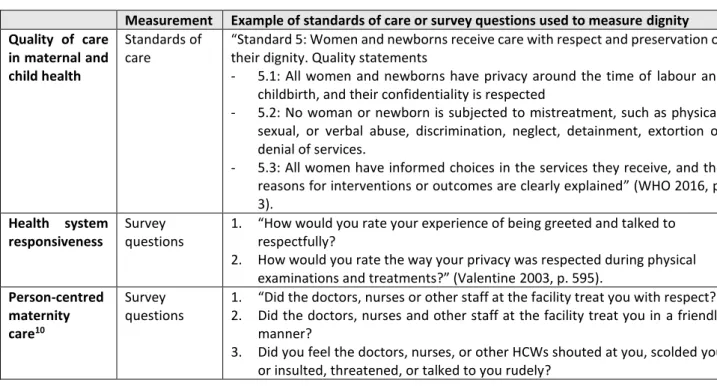
Survey questions and observational checklists used to measure dignity globally
Summary overview of 20 key articles on dignity in LMICs
Zambia Qualitative study of factors associated with health seeking practices in four rural areas of Zambia. HCWs identified “social preservation of dignity” (p.6) as a reason for prenatal clients' male partners' delay in seeking HIV testing. Qualitative study on access to health services for men who have sex with men (MSM), female sex workers and people who use drugs in South Africa found that interviewed patients avoided seeking care at health facilities as a result of demeaning experiences of being exposed for shame. , scolded and embarrassed by HCW.
Iran Qualitative study on patients' perception of dignity in Iran and hospital described four key aspects of dignity in a health facility setting: a respectful environment, privacy, attention and involvement in decision making. For example, interpersonal characteristics of the health professional (i.e., professional dignity) have been noted as facilitators of dignity. Although different experiences of dignity were not reported across different health facilities included in the study, experiences of dignity differed by patient characteristics (ie, only 8% of Muslim women compared to 22% and 28% of Buddhist and Muslim women were medically declared procedures. and process) thus suggesting inequitable distribution of dignity.
In addition, high-income and literate women were more likely to report positive experiences of dignity than low-income and illiterate women. Iran Qualitative research on the dignity perception of hospitalized adolescents in Iran reported that adolescents found dignity through the maintenance of privacy, autonomy, individualism and intimate communication. Uganda A qualitative study in Uganda into the expectations regarding high-quality deliveries has shown that the preservation of the dignity and the respectful attitude of the staff are core characteristics of quality.
India Secondary analysis of data related to health system responsiveness showed that experiences of dignity in the health system varied by income level in India. Based on findings from nearly 700 of India's health care users, the poorest were less likely to describe their experience of dignity at a health facility as "very good" compared to high-income users' assessment of dignity. The results show that socio-economic status can influence a patient's experience of dignity in the healthcare system regardless of facility type.
Tanzania Qualitative study of experiences and responses to neglect and abuse during childbirth by men and women in the Morogoro region of Tanzania. Iran Qualitative study on caregivers' perception of women's dignity during childbirth in Iran revealed that respect for privacy, respect for patient preference including involvement in treatment decisions or tolerance for religious practices, and full consideration including non-discrimination are the three most important aspects. importance of dignity. during birth. Iran Qualitative study in Tehran on women's perspectives on health system factors related to the choice of mode of childbirth attributed Iran's extremely high rates of caesarean sections to health system limitations that negatively affect dignity during childbirth.
Leading frameworks on respectful maternity care
Proposed data extraction sheet
Raphaelalani et al. 2021), and African inherent of the concept (see more below) (Murithi 2007), there are still several barriers to dignity in the health system (Gostin et al. Ojwang et al. 2010), but the implementation of such policies across the health the system is not clear. Barriers to policy implementation are complex (Hawe 2015) and well documented widely in health (Buse et al. 2005;.
Birhanu et al. 2021), this policy focuses on the dignity of patients in the healthcare system, not healthcare professionals.
Summary of search terms
Summary of full data extraction sheet
Health Policy and Planning Journal Guidelines
Authorship: Please note that there must be an LMIC (lower-middle income) named author from the region of the paper included in the paper. Final approval of the version to be submitted - all named authors must approve the paper before submission. A word count of the full article: Word limits do not include Abstract, References, Figure/Table legends.
Other financial and material support, specifying the nature of the support, must also be acknowledged. Authors should therefore check with the editor before speaking to members of the media or distributing papers. For specific chemicals or equipment, the name and location of the supplier should be given in brackets.
The discussion should be an interpretation of the results and their significance in relation to the work of other authors. The units in which the results are expressed must be given in brackets at the top of each column and not repeated in each row of the table. The statement may refer to original data obtained during the study or to third-party data analyzed in the article.
The sections should be organized as follows: i) Title page, ii) Abstract, iii) Introduction, iv) Body of the paper, and v) References. This series aims to support the development of the field of health policy and systems research by supporting methodological discussion. The sections should be organized as follows: i) Title page, ii) Abstract, iii) Introduction, iv) Body of the paper, and v) References.
In the main body of the paper, subheadings can be useful to indicate key elements of the reported experience. In original articles, this information should also be included in the methods section of the submitted manuscript. This image/content is not covered by the Creative Commons license terms of this publication.