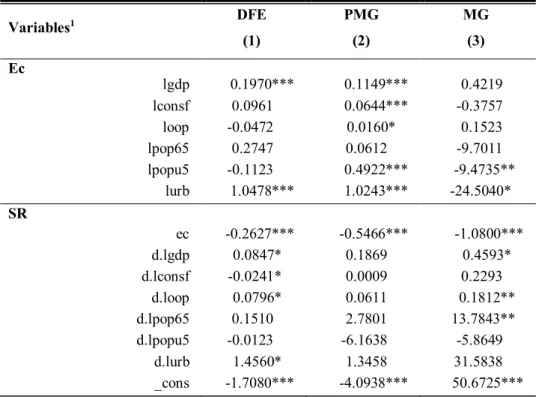
However, there is insufficient evidence on the determinants of access to health care to inform policy makers. The income elasticity of access to health care was 0.1149, suggesting that access to health care is not a luxury good.
Background
The literature notes that access to healthcare has proven to be an effective channel for vulnerable individuals to improve or maintain their health status (Tanaka, 2010). Second, unlike previous studies that used a single indicator, the current study used an access index to measure access to health care.
Research problem and the significance of this study
First, it takes a dynamic approach by attempting to determine the short- and long-term impact of determinants of access to healthcare using the ARDL model.
Research objectives
To determine whether there is a long-term relationship between access to health care and the identified factors;.
Methodology
Delimitation of the study
Structure of the dissertation
It focuses on important demand factors affecting access to health care in Africa. This chapter reviews the literature on access to health care in order to identify gaps.
Background to the interest in access to health care
Concepts of access to health care are reviewed in Chapter 3, the theoretical framework for studying access to health care is discussed in Chapter 4, and empirical evidence is analyzed in Chapter 5.
Access to healthcare: Process, Definition and Dimensions and Measurement
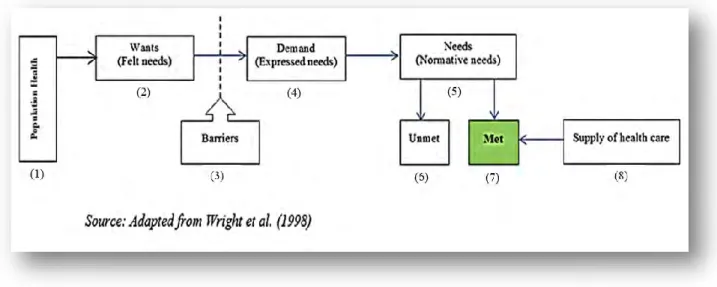
The process of access to healthcare
The health of the population is the starting point in the process of access to health care (Figure 2.1). If they want to access health care (5), they can find (7) or not (6) the care they want in health facilities (8).
Definition and dimensions of access to healthcare
The definitions of access to healthcare reveal two main dimensions: the demand dimension and the supply dimensions, with some variants. These variants relate to the geographical, financial, cultural and structural factors of access to healthcare.
Measurement of access to healthcare
For example, variations in the supply and demand perspectives include an environment conducive to patients' use of health care (Clark, 1983). Furthermore, utilization measures are silent on the quality or quantity of health care provided (Burstrom, 2002).
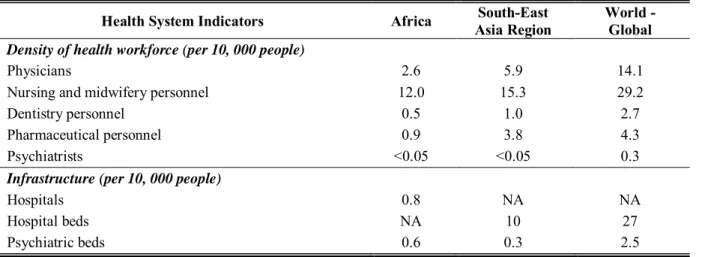
State of access to health care in Africa
Another factor affecting access to health care in Africa is the fact that such access is unequally distributed. Limited access to health care in the African context has given rise to a number of strategies to remedy the situation.
Theoretical framework for access to health care
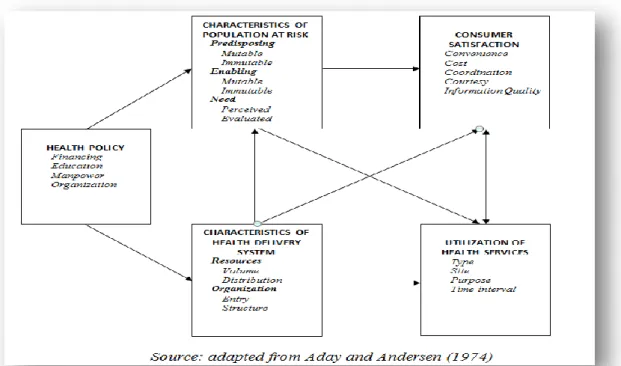
Aday and Andersen framework
The Alma-Ata Declaration (1978), emphasizing the importance of primary health care, is one of the strategies adopted by Africans. This is the most popular model for studying the utilization of health services by different population groups (Andersen, 1995).
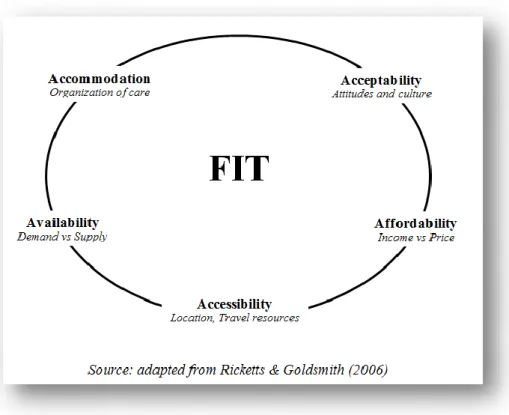
Penchansky & Thomas framework
They built Penchansky's "5 As", a model of access to health services, which divides the broad and ambiguous concept of access to health care into five interacting dimensions that determine the use of health services: availability, accessibility, availability, accommodation and affordability ( Figure 2.3). The advantage of Penchansky and Thomas' conceptualization of access to health care is that it is not only related to access or utilization of services, but also identifies different dimensions of the client-provider relationship.
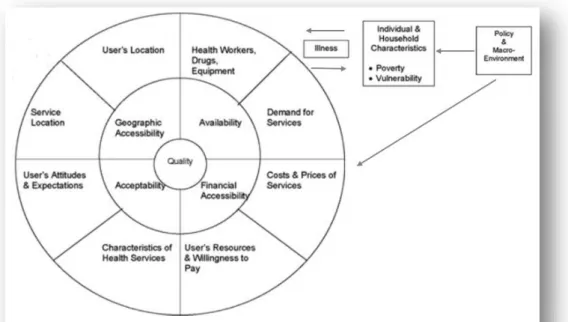
Peters-Garg-Bloom-Walker-Brieger-Rahman framework
This is also related to the technical ability of healthcare services to influence the health of individuals. To the right of the circle is a group of distal determinants of access to health care services, illustrated at the policy or macro-environmental level and at the individual and household level.
Empirical evidence
Further insight into access to health care can be gained by examining the empirical evidence. According to demand theory, income (GDP) is expected to be positively related to access to health care. Where access to health care (ha) is the outcome variable and independent variables are represented by income (Y), distance to health care facilities (D) and other control variables (Z).
The aim of this study was to investigate the demand side of the determinants of access to healthcare services in African countries. Findings from this study provide evidence that policymakers can use to improve access to health care in the long term. Remittances, Public Health Spending and Foreign Aid in Access to Health Care Services in Developing Countries, Halshs.
Access to health care in South Africa - the influence of race and class: original article.
Chapter summary
Access to healthcare: Dimensions used and Measurement
Dimensions used
The literature on health access reviewed in the previous chapter has noted that the concept of access to health care is complex. This study follows the demand perspective of Peters et al.'s (2008) framework and focuses only on two dimensions of access, namely economic access (cost of care, income) and geographic access (distance to facility). These two dimensions were selected because they are considered to include more objective factors affecting the demand side of access to health care that can be measured and are relevant for policy making.
Measuring access to health care
It could be argued that the weakness of this methodology is taking an unweighted average of all indicators to construct the index, as the indicators do not have the same weight. However, in the absence of weighting criteria, this built-in indicator provides an indication of access to healthcare that encompasses more dimensions of access than individual indicators could capture.
Determinants of access contemplated in the estimation
Variables of interest
At the macro level, it seems difficult to get indicators that capture the distance to health facilities as it is at the micro level. Whether the distance to health care at the micro or macro level depends on indicators such as the density of health services (Hjortsberg, 2003), the level of public infrastructure (Vos & Sánchez, 2014) or the Euclidean distance between the population and health. facilities (Larson et al., 2012). The consumption of fuel is expected to have a negative sign, meaning that distance to health facilities is negatively associated with access to health care.
Control variables
While the geographic accessibility dimension of access to health care is essential and the main concern of the rural area, access to health care discussions informing the distance between the patient and the provider should also allude to other factors such as community residences. However, the challenge, especially at the macro level, is to obtain an indicator or a proxy that could capture the entire aspect of distance to health care services; this limitation paves the way for further research.
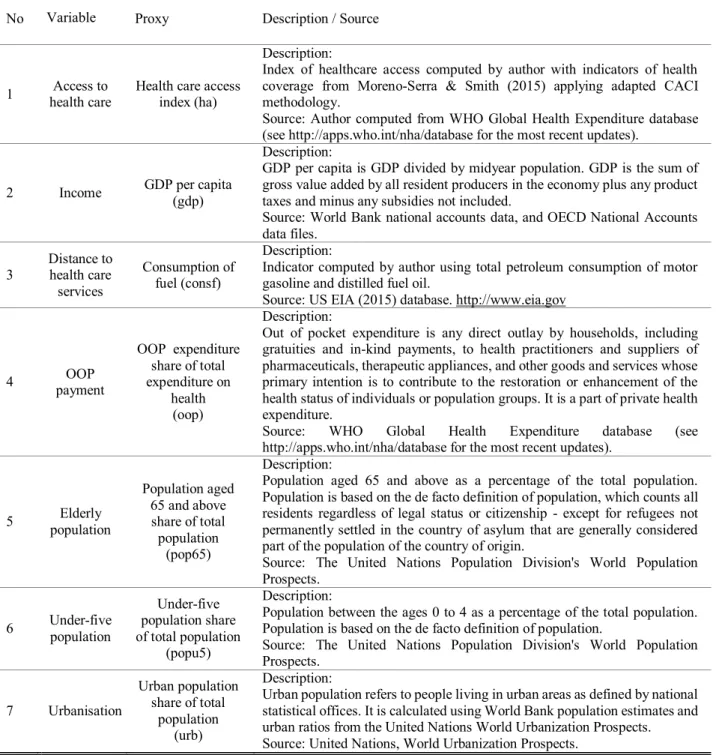
Data collection
Sources, period of analysis and variables definition
Variables summary
Modelling approach
- Panel data modelling
- Modelling in this study
- Specifications adopted and estimation techniques
- Estimation techniques
- Data analysis
This study used the Translog or Log-log model – the most popular flexible functional form – to guarantee the linearity of the model and to interpret the coefficient as elasticities. The coefficient 1i measures the long-run income elasticity for access to health care that is expected to be positive. Therefore, all coefficients can vary and be heterogeneous in the long-term and short-term.
Chapter summary
The test provides seven test statistics (parametric and non-parametric) under zero or no cointegration in a heterogeneous panel with one or more non-stationary regressors. The final step was to present the demand-side determinants of access to health care derived from the estimation of the study model in Equation (3). Based on the literature reviewed in Chapter Three, Section 4 elaborates on the findings of the research.
Descriptive analysis and Preliminary tests
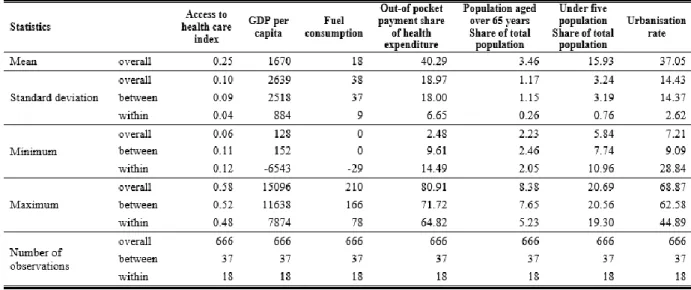
Descriptive statistics
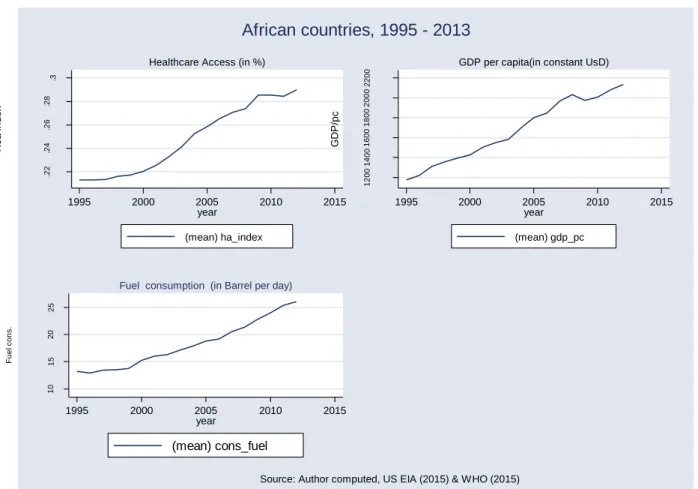
The main independent variables – GDP per capita and fuel consumption – also present large pooled SDs relative to their pooled means, indicating the same specificity as the index of access to health services and showing differences in wealth between African countries. It can also be observed in Table 4.3 that the within-SD is low compared to the between-country SD, indicating that access to health care or its dependent variables within countries do not vary much across African countries. Although access to health care and GDP per capita are flatter from 2008 to 2013, this does not appear to affect fuel consumption, meaning that an event that affects access to health care and GDP does not affect fuel consumption.
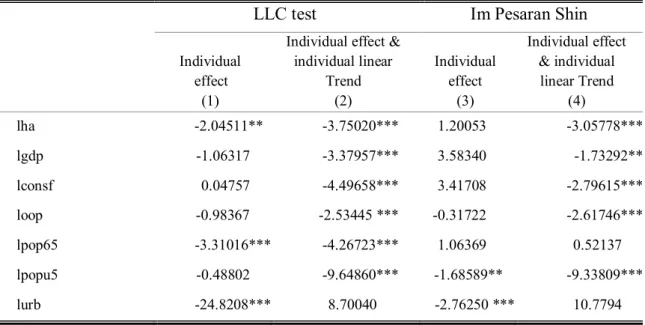
Preliminary tests
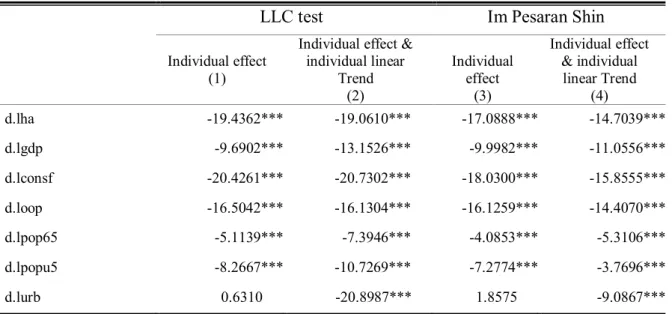
Then, the unit root test must be performed on first-differenced variables to determine whether the non-stationary variables are I(1). The unit root test results with the first differenced variables presented in Table 4.5 clearly show that all the series are stationary. Following the unit root test results, the study variables are a mixture of I(0) and I(1) series.
Determinants of access to health care
Main regression estimation
Comparing the results of the three estimators, it can be noted that the coefficients for the main variables are all significant only in the PMG. This was selected in the test with the MG estimator, where the null hypothesis of no systematic difference in coefficients was not rejected, as the p-value is 0.4419. Based on the main results of this study, it can be said that access to healthcare services in African countries is determined by the proxy of GDP per capita for income and fuel consumption for the distance to healthcare facilities, but only in the long run term. walk.
Regression estimations by income class
A quick perusal of Table 4.8 shows that only the GDP long-run elasticity and the error correction coefficient are statistically significant across all income and FULL specifications. However, the GDP affects access in the countries' income groups differently, with the highest impact in the BMI (0.6167) and the lowest in the LI (0.3376). All the income class specifications (LI, BMI and UMI) show that access to health care in African countries is consistently driven by GDP per capita in the long run.
Regression at country level
Burundi, Ghana and Mauritius at the 5 percent significance level; and for Cabo Verde, Côte d'Ivoire and Rwanda at the 10 percent significance level. Apart from Burundi, Ghana, Mozambique and Rwanda, GDP per short-run capita elasticities have positive expected signs for all countries with significant coefficients; and these coefficients range from 0.2584 to 2.5079 with Congo Rep. More, the short-run fuel consumption elasticity indicates is only significant for Cameroon and Mozambique at the 1 percent significance level; for Angola, Cabo Verde, Equatorial Guinea, Ethiopia, Gambia, Morocco and Zambia at the 5 percent significance level; and for you.
Discussion of the results
This positive long-term income elasticity suggests that access to health care in Africa is not a luxury. The long-term coefficient of fuel consumption, a proxy for distance to medical facilities, shows a positive unexpected sign. The short-run distance to health care elasticity from the country-specific regressions is significant for Angola, Cabo Verde, Cameroon, Dem.
Conclusion
The study found that in African countries, the demand-side determinants of access to healthcare are socio-economic, behavioral and environmental factors. In this regard, the study contributed to the literature by analyzing the dynamic aspect of access to healthcare at the macro level. Using ECM, it was shown that the most important determinants of access to healthcare were income and distance to healthcare.
Recommendations
Mauritius where the short-term income elasticities are higher than one which rather suggests that access to health care services in these countries is a short-term luxury good. Additionally, this study explored the dynamic aspects of access to health care providing information on the factors that persistently drive access to health care in Africa. To the best of our knowledge, no study has been conducted on African countries on access to health care services that takes into account these two aspects raised in this study.
Limitations of the study
Access to primary health care and health outcomes: the relationship between GP characteristics and mortality rates. Measuring equity in access to health care: a case study of malaria control interventions in the Kassena-Nankana District of Northern Ghana. The elasticity of demand for health care in Burkina Faso: differences across age and income groups.
INDIVIDUAL COUNTRY REGRESSION RESULTS
REGRESSION AND TEST OUTPUTS
Automatic selection of lag length based on SIC: automatic selection of Newey-West bandwidth 0 to 3 and Bartlett kernel. Automatic lag length selection based on SIC: automatic selection of Newey-West bandwidth from 0 to 2 and Bartlett kernel. Automatic lag length selection based on SIC with maximum lag 3 Newey-West automatic bandwidth selection and Bartlett kernel.