Nonhlanhla Yende-Zuma – Statistician and co-author of the script Anushka Naidoo – Co-author of the script. It was originally submitted to the International Journal of Tuberculosis and Lung disease on 16 Oct 16 and revision 1 of the manuscript was resubmitted on 26 Nov 2016.
Chapter 1 presents the current scale of the HIV-TB co-infection epidemic, the importance of isoniazid preventive treatment (IPT), challenges in implementing IPT, the global and local impact of the TB and HIV epidemics, data on the provision and use of IPT, the need for HIV and TB treatment . This study is a secondary analysis of data on the initiation of an IPT program among clinical trial participants.
CHAPTER ONE: INTRODUCTION
Context for the study: The importance of IPT implementation
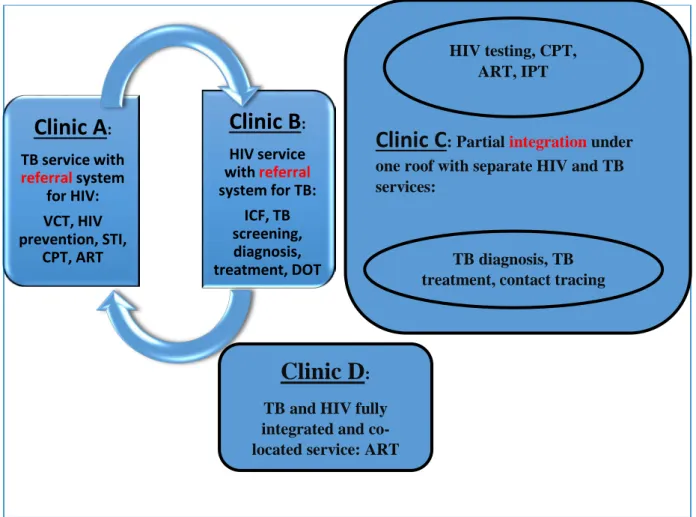
Best practices and models that have been used to integrate TB and HIV drug delivery can be applied to the delivery of IPT (22, 23). A fully integrated service is proposed in Figure 1, where a combined package of HIV and TB care is provided by health staff who are cross-trained to provide screening, treatment and preventive therapy in a standardized approach to TB and HIV service delivery.
Clinic A
Clinic B
Clinic D
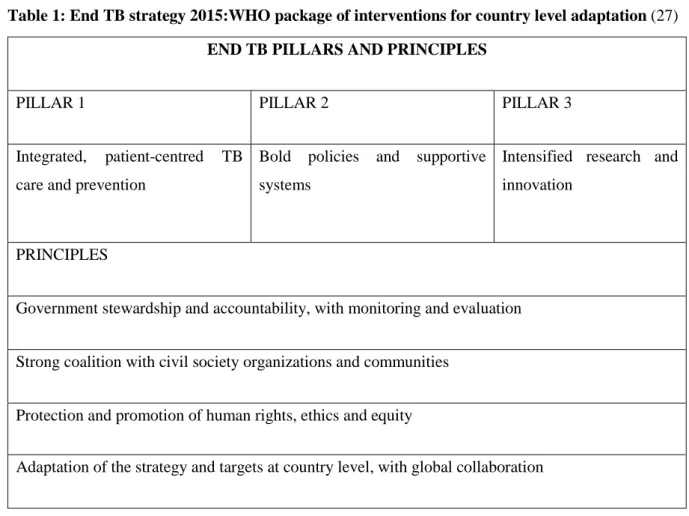
The STOP TB strategy disseminated the pursuit of high-quality DOTS; address the challenges of co-infection (TB/HIV) as well as MDR-TB; health system strengthening; involving all healthcare providers, people with tuberculosis and local communities, creating, promoting and improving research opportunities. Going forward, the END TB strategy (Table 1) takes the following approach: Integrated, patient-centred care and prevention, bold policies and supporting systems, intensified research and innovation (27).
1994 DOTS
2005 STOP
2015 END TB
Problem statement
Rapid re-infection and relapse rates of TB mitigate the conditions and hinder any progress made towards TB prevention. HIV/TB service integration is the gateway to successful implementation of TB prevention-based interventions such as IPT. However, most data published on IPT have been obtained from research conducted in the pre-ART era or in ART populations with no prior history of TB, and prior TB exposure is grounds for exclusion from IPT.
There is a consequent paucity of data on IPT outcomes and effect on TB incidence in ART and TB treatment experienced populations.
Study hypothesis
To report on areas of implementation that require strengthening or modification to increase the quality and effectiveness of IPT delivery. To identify any trends in IPT discontinuation, IPT completion and reasons for IPT refusal.
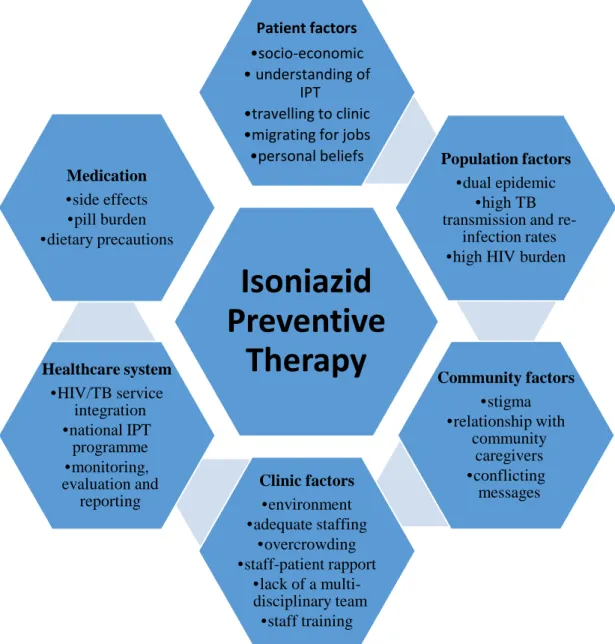
Conceptual framework
A lack of facilities and limited staff access to IPT training, standard operating procedures (SOP), policies and guidelines negatively impact staff's ability to adequately screen, educate and implement IPT use among patients (90). In turn, patients do not fully understand the importance of IPT for tuberculosis prevention, and this may affect their adherence. However, some clinic settings with well-trained staff, adequate privacy, and well-developed TB screening and IPT guidelines, counseling, and policies promote an improved patient experience that would increase their education, awareness, and subsequent compliance with the IPT course (119).
In contrast, it should also be taken into account that being on lifelong ART will promote adherence to IPT (48). The socio-economic status of patient impact on uptake, compliance, awareness and understanding of IPT as well. In addition, personal beliefs may hinder their commitment to IPT in terms of fear of side effects, fear of TB/HIV.
Isoniazid Preventive
Therapy
CHAPTER TWO: METHODS
Study location
The site is located next to the Prince Cyril Zulu Communicable Disease Center and offers facilities for TB/HIV care and serves the functional region of Durban. Consultation – The professional nurse verified that the patients are still suitable for IPT or enrollment on IPT by reviewing TB symptoms. Complicated cases, TB suspects and potential enrollees were referred to the clinic for further work-up.
Pharmacist's Role - The pharmacist reviewed the TB symptom checklist and confirmed eligibility for IPT monthly. Patients' questions, queries or concerns were forwarded to the pharmacist by the clinic staff and addressed during personal patient counseling in addition to the ASP, as the pharmacy was the last stop during the clinic visit. If active TB was diagnosed, INH was discontinued and the patient was referred to a neighboring TB facility located next to CAPRISA to begin TB treatment immediately.
VITALS
CONSULT
PHARMACY
- Study population, sample size and sampling strategy
- Inclusion and exclusion criteria
- Data collection
- Data analysis
- Ethical considerations and confidentiality
The master's candidate conducted a retrospective analysis of all records of the 402 patients with a previous history of TB enrolled in the TRUTH, who received ART at the CAPRISA clinic at the time of the implementation of the IPT program. Those who had no documented signs or symptoms of active TB and who met the criteria set out in the South African IPT guidelines in force at the time were considered eligible to receive IPT while accessing care within the TRUTH study. The pharmacy assessed patient understanding of the IPT counseling at the time of dispensing and, in addition, provided more motivating adherence.
The study statistician downloaded the raw data collected during CRF completion per TRuTH study participant and provided an MS Excel spreadsheet to the candidate to clean and extract the data for the secondary analysis. Number of tablets dispensed at the last clinic visit – [Number of tablets not taken] # x 100 Number of tablets dispensed at the last clinic visit. However, in the parent study CAP005 TRuTH, informed consent was obtained for the use of the clinical and demographic data.
CHAPTER THREE: MANUSCRIPT
Manuscript Implementing Isoniazid Preventive Therapy in a TB-treatment experienced cohort on ART experienced cohort on ART
We hypothesized that 6 months of IPT would reduce tuberculosis incidence in a high HIV/TB burden setting among a previously treated cohort. Univariate and multivariate log-binomial regression models were used to identify predictors of IPT completion. The modeled variables included age, sex, Hb, CD4, number of past TB episodes and years on ART.
Exposure to IPT resulted in a non-significant 33% reduction in tuberculosis incidence among IPT users. Age, sex, CD4, Hb, previous TB episodes, and years on ART were not identified as predictors of IPT adherence or completion in the univariate or multivariate analysis. Involved in the design and implementation of IPT Adherence Support Program (ASP) materials for ART/IPT consultants in the clinic.
CHAPTER FOUR
OVERALL DISCUSSION
Study limitations
The small sample size in this secondary analysis undermined our ability to demonstrate a statistically significant impact of IPT in preventing new cases of tuberculosis in patients who have previously had tuberculosis. The CAP 005 TRUTH study and these IPT subanalyses were unable to detect significant differences in tuberculosis incidence between those who initiated IPT and those who did not initiate IPT. This may have led to over-reporting of suspected tuberculosis and subsequent ineligibility for IPT or IPT interruptions.
Increased staffing and infrastructure resources enabled rapid confirmation or exclusion of incident TB and efficient identification of patients eligible for IPT. This may have contributed to higher IPT adherence and completion rates reported in the study. We also did not measure qualitative factors that may have had an impact on IPT uptake, such as patients' perception of TB risk, disclosure of HIV status, understanding of the importance of IPT for TB prevention, level of education or economic status at the time of IPT eligibility assessment.
Recommendations for clinical practice
One of the recommendations in the survey is that further research, such as risk-benefit assessments, be conducted to determine whether IPT drives INH resistance and to evaluate the continued effectiveness of IPT as INH resistance increases. Promote the use of point-of-care (POC) diagnostics to rule out TB and thereby speed the process of initiation to IPT, reduce course interruptions once initiated, and ensure re-entry to IPT and course completion. With the use of GeneXpert® for POC diagnosis of TB, the risk of false positives is of concern.
GeneXpert may continue to play a valuable role in the IPT setting as opposed to gene, until other point-of-care diagnostics with higher specificity become available for retreatment of TB. Innovative use of available technology beyond point-of-care diagnostics, such as mobile phone-based technology, has the potential to play a pivotal role in improving the delivery of IPT care to patients. Promote the use of computerized dispensing systems for improved accuracy and monitoring of drug dispensing processes, such as by improving access and availability of Rx solution systems rolled out in the public sector.
Recommendations for future research
Some researchers have identified the potential false-positive risk of GeneXpert in retreatment TB cases to be 1 in 7 (145). In the CAPRISA 011 IMPRESS study, some baseline data on cell phone penetration and capabilities among TB and TB/HIV co-infected patients were collected, which would help further develop this project. This type of intervention holds promise and should be further investigated in the South African context, with SA having the largest HIV and IPT programs in the world.
Such models could shed more light on the optimal way to approach TB prevention in this high-risk population and whether long-term protective benefits will be durable. More studies, more investigational drugs repurposed for TB prevention, as well as other interventions need to be broader. Raise awareness within the pharmacy fraternity and issue a call for more research on the pharmacist's role in TB prevention.
Concluding statements
Completion of isoniazid preventive therapy and survival in HIV-infected, TST-positive adults in Tanzania. Completion of isoniazid preventive therapy and survival in TST-positive HIV-infected adults in Tanzania. Beneficial effect of isoniazid preventive therapy and antiretroviral therapy on tuberculosis incidence among people living with HIV in Ethiopia.
Effect after treatment of preventive therapy with isoniazid on the incidence of tuberculosis in HIV-infected persons receiving antiretroviral therapy. Preventive therapy with isoniazid for tuberculosis in South Africa: a review of the local evidence base. Perceived barriers to implementation of isoniazid preventive therapy for people living with HIV in resource-limited settings:
APPENDICES
Supervisor / Student Memorandum of Understanding
Product labels: labels generated have the amount of study material resupplied and/or reissued, the next appointment date, the participant number, participant initials, etc. review of the IPT and ART prescribing process. This is based on the Pack Date as well as the months of inventory or can be adjusted manually.
The pill count function can be used to check compliance and then enter the amount of pills returned from the previous pack issued. It shows the drug name and the dose (based on the prescription you have already captured). On this screen you can change the quantities, the batch from which the medication was given as well as the amount of labels to print.
A column to inform the user how much stock is left of the fabric (Pack in stock). If you used the pill counter function, this will be the amount they came back with plus the amount you dispensed.